
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Binder’s syndrome and its management in a tertiary hospital
Harsha Vardhan*; Vijay Kumar; Veerendra Prasad; Divya Narain Upadhyaya
Department of Plastic Surgery, King George’s Medical University, Lucknow, UP, India.
*Corresponding Author : Vardhan Harsha
Department of Plastic Surgery, King George’s Medical University, Lucknow, UP, India.
Email: harshaok@yahoo.com
Received : Jul 26, 2022
Accepted : Aug 11, 2022
Published : Aug 18, 2022
Archived : www.jcimcr.org
Copyright : © Harsha V (2022).
Abstract
Binder’s Syndrome or Maxillonasal dysplasia is an uncommon condition that presents as retrusion of the midface. This varies in severity, ranging from minor involvement of the nose to severe hypoplasia of the maxillary complex. Depending upon the severity, different types of procedures are required. In this paper we present our experience with managing such patients.
19 patients were admitted with the diagnosis of Binders syndrome in our department in the last three years. 3 were males and 16 were females. Most of the patients belonged to the 15 to 30 year age group. The patients had varying degrees of midface hypoplasia. Occlusion was maintained in most patients with compensation noted in some cases. The main complains of the patients were usually cosmetic. Depending upon their severity they were treated by either Rhinoplasty (17 cases) or Orthognathic Surgery (2 patients).
Parents of young females, approaching marriageable age, commonly seek treatment for Binder’s Syndrome. This presumption is supported by the patient demographics in our study. Such parents frequently request the bare minimum treatment to obvious deformity, usually reluctant to correct the underlying deformity. Patients accept the newly protuberant nose, and are usually satisfied with the surgical outcome.
Citation: Vardhan H, Kumar V, Prasad V, Upadhyaya DN. Binder’s syndrome and its management in a tertiary hospital. J Clin Images Med Case Rep. 2022; 3(8): 2005.
Introduction
Noyes first reported the features seen in maxilla-nasal dysplasia in 1920s, however it was Binder, in 1962, who described the constellation of facial features which has now become synonymous with his name. The classic features are an arhinoid face, an increased nasofrontal angle and a short columnella. On radiographic evaluation, there is absence of the anterior nasal spine, the antero-posterior length of the maxilla is decreased and the class 3 malocclusion. The procedure of choice in the classical deformity is a LeFort 2 osteotomy and advancement. This addresses the whole gambit of midface anomalies including the nasal platform as well as the occlusional problems. However, this is an invasive surgery, with significant morbidity. An alternative is a LeFort 1 osteotomy along with a nasal augmentation. The LeFort 1 addresses the occlusion and the nasal augmentation camouflages the nasal hypoplasia. If the occlusion is unaffected, then a dorsal nasal augmentation is often an agreeable option to the patients.
There is scant literature available from India reporting the presence of Binder syndrome [1-6]. The aim of this paper is to describe our experience with the management of Binder’s syndrome.
Methods
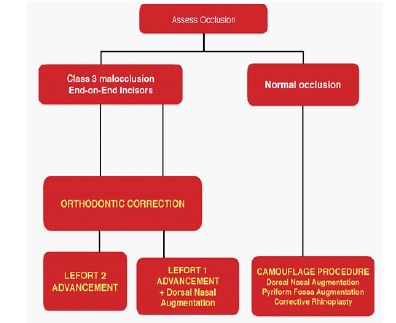
This is a retrospective review of cases operated in the department of Plastic Surgery. A review of the cases of Binder’s Syndrome for three years, from 2016 to 2019 was performed. The management options for our patients are given in Figure 1. Ethical clearance was waived as it is a retrospective review of charts and no details of the patients have been given.
Procedure
Dorsal nasal augmentation
The procedure was performed in general or regional anaesthesia. The patient lies supine on the table with slight extension of the neck provided with support under the shoulder. Dorsal nasal augmentation was done using the open rhinoplasty approach. A vertical mid-columnellar incision is made to access the dorsum. Even a transcolumnellar incision with extension in the nasal vestibule can be made as done in classical open rhinoplasty. This approach provides good visualization of the nasal framework, but is really not required for a dorsal nasal augmentation per se. Alternatively a transverse incision at the root of nose can also be used. This allows the dorsum to be dissected. The additional advantage is that rigid fixation of the bone graft can be done with the help of screws. Infrequently, coronal approach may be used.
Whatever the approach, a subcutaneous pocket is created in the dorsum of the nose. It is important to keep the pocket in the midline, to prevent deviation of the graft towards one side. The soft tissue is freed from the bony nasal septum and the anterior surface is abraded with a rasp. This allows for the graft to be placed on raw bone, which is essential for the survival and longevity of the bone graft.
Graft harvest
The preferred donor site of bone graft is olecranon. Other areas from which graft can be harvested are from the rib, calvarium or the iliac crest. The advantages of the olecranon are many. The procedure can be performed in regional anaesthesia and the need for general anaesthesia is avoided, which is especially important in resource-constrained settings. A bony strut of adequate thickness can be obtained. There is no donor site morbidity. The post-operative pain is lesser, as compared to other donor sites like the rib and the iliac crest. Performed under tourniquet, it can be harvested with minimal blood loss.
Under tourniquet control, a curvilinear incision is made over the olecranon. This incision is deepened upto the bone and the periosteum is incised. A ‘canoe’ shaped bone graft is harvested of the required dimensions. The wound is sutured in layers over a suction drain. It is prudent to provide a splint over the elbow to prevent direct trauma to the olecranon. This splint is removed by two weeks.
The graft is further refined on the table and then is placed in the tunnel created. The graft is placed with the thin edge cranially and the thicker edge caudally. The cancellous bone is in contact with the raw bone in the nose to allow better take of graft. Too high placement of the graft, or placing the thick end cranially will result in the obliteration of the nasofrontal angle, giving an appearance of a different ethinicity.
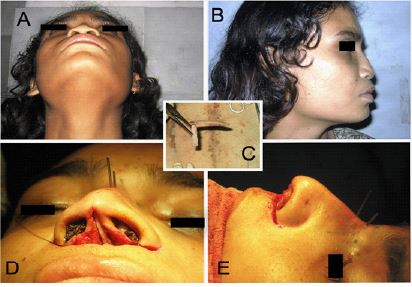
The graft is fixed with two cancellous screws. This type of fixation results in the graft fixed in a cantilever fashion. In case of a short columnella, a columnellar strut is placed. A fossa is made in the dorsal graft into which the strut is hitched. On the other end the graft is placed on the anterior nasal spine (Figure 2).
Often there is deficiency of the nasal base in addition to a depressed dorsum. This can be camouflaged with a pyriform fossa augmentation. Additional bone graft can be placed in the pyriform region. The can be done through a vestibular mucosal incision [7]. Injection of hydroxyl-appatite fillers can also be used to augment the nasal base.
Orthognathic surgery
Nasal intubation is performed and throat pack is placed. Hypotensive anaesthesia keeps the blood loss minimum and adequate volume replacement is kept at standby. The patient lies supine with the neck extended. After adrenaline infiltration, oral mucosal incisions are made on either side of midline. The incision is made in the gingiva, preserving the tooth roots, but not in the depth of the vestibule. This allows suturing of the mucosal incision, without difficulty and subsequent scarring. The incision is deepened upto the periosteum and the maxilla is freed.
Osteotomies are done depending upon the type of LeFort planned. The cuts can be made with a motorized saw or an osteotome and mallet. Advancement is done and once the teeth fit well on the occlusional wafer, the movement is maintained by an intermaxillary fixation. Definitive fixation is done maintain the position, using plate and screws. Larger distance of advancement is covered by distraction.
Once the advancement is attainted, the wound is sutured and intermaxillary fixation is made. If distraction is to be done, distraction is started on the first postoperative day.
Results
A total of 29 procedures were performed in 21 patients with Binder’s Syndrome. 81% of the patients were females and 19% were males. Out of the 21 patients, 10 were more than 20 years old, 10 were between 11 to 20 years and 1 was less than 10 years of age. Dorsal nasal augmentation was the most commonly performed procedure. It was performed in 18 cases.(FIGURE 3) Corrections to the nose were done in 11 cases and 2 patients underwent Orthognathic surgery. Lefort 1 osteotomy was performed in 1 patient and Lefort 2 was performed in another patient. The facial analysis is shown in Table 1 (Figures 4,5).



Discussion
Management of Binder’s syndrome focuses on two aspects, the functional and the cosmetic. The functional deformity is due to malocclusion. Occlusional deformities give rise to abnormal dental relationships and crowding of teeth. The concave shaped appearance of the face, along with absence of the nasal projection constitutes the cosmetic deficiency.
Table 1: The course of endoscopic treatments.
| Patient 1 | Patient 2 | |||
|---|---|---|---|---|
| PREOP | POST OP | PREOP | POST OP | |
| SNA | 76 | 80 | 76 | 80 |
| SNB | 81 | 80 | 83 | 82 |
| ANB | -5 | 0 | -7 | -2 |
| Effective Maxillary Length (mm) | 67 | 75 | 72 | 78 |
| Advancement | 8 mm | 6 mm | ||
Figure 1 demonstrates the management protocol followed at our institute. Occlusion is the central criteria for determining the management plan. Patients with class 3 malocclusion have undergone dentoalveolar compensations and may have incisor end-to-end bite. These patients are suggested orthodontic corrections to unmask the actual occlusion, following which orthognathic surgery is planned. A LeFort 2 osteotomy addresses the occlusion and the midface hypoplasia both. It elevates the nose as well as the nasal platform and is a single solution for all the deformities of Binder syndrome. This is, however, not without its morbidity. An alternative is to perform a Lefort 1 osteotomy to correct the occlusional anomalies and a nasal augmentation. This reduces the morbidity of the orthognathic surgery, but increases the number of surgeries required. If the occlusion is normal, augmentation of the nose is performed. Augmentation of the nose and the nasal platform can also be used to camouflage the hypoplastic midface.
Although congenital, Binder’s frequently has social implications. Although males and females are equally affected [8], our series had a female predominance. The reason for this is social. Most of the females belonged to “pre-marriage” age. The usual reason for seeking treatment was impending marriage, with the family feeling that correction of this deformity would make for a more ‘suitable’ bride. Male patients do not face this situation. It is for this reason that most of the patients opt against the orthognathic correction, choosing to camouflage the deformity with a dorsal nasal augmentation only. In a study by Deshpande and Juneja [5], 2 out of 15 patients underwent orthognathic surgery, that also Lefort 1 advancement. Augmentation is usually performed after maxillary advancement [9]. This gives an idea regarding the need and degree of camouflage required. Sun and Steinbecker [10] described the situations where simultaneous orthognathic surgery and rhinoplasty may be performed.
Some authors prefer to use cartilage graft instead of bone graft to augment the nose [11]. Rune et al [12] studied the properties of bone graft in Binder’s syndrome. They did not find resorption of the bone grafts with serial roentegenographs. They suggested that bone grafts are a favourable option in Binder’s syndrome, considering the amount of graft required and the tension of the overlying envelop. Cartilage may not be able to resist the pressure of the tight nasal skin. Cartilage is however softer and gives a less rigid tip [13]. Augmentation of the nasal base is also done as part of the camouflage procedure. This can be done using cartilage [6] or bone.
Conclusion
The management of Binder’s syndrome requires a team approach in collaboration with the orthodontist, to formulate a plan. Although these patients have both cosmetic and functional deformities, the cosmetic problem seems to be more trouble some to the patient. Social indications supersede the medical indications with augmentation procedures most commonly performed in these patients.
References
- Yamani VR, Ghosh S, Tirunagari S. Nasal correction in nasomaxillary hypoplasia (Binder’s syndrome): An optimised classification and treatment. Indian J Plast Surg. 2016; 49(3): 314–21.
- Veeramani A, Sawh R, Steinbacher DM. Orthognathic surgery and rhinoplasty to address nasomaxillary hypoplasia. Plast Reconstr Surg. 2017; 140(5): 930–2.
- Rao K, Babu S, Castelino R, Bhat S. Binder′s syndrome: Presentation of a rare case. CHRISMED J Heal Res. 2016; 3(3): 232.
- Mudgade D, Patel J, Nasiruddin M, Motghare P. Binder′s syndrome: Report of two cases. J Indian Acad Oral Med Radiol. 2014; 26(2): 196.
- Deshpande SN, Juneja MH. Binder’s syndrome (maxillonasal dysplasia) different treatment modalities: Our experience. Indian J Plast Surg. 2012; 45(1): 62–6.
- Balan JR, Mathew S, Kumar P. Case Report Binder’s syndrome and aesthetic improvement: A case report. Vol. 1, International Journal of Aesthetic and Health Rejuvenation. 2020; 1(3): 20.
- Converse JM. Restoration Of Facial Contour By Bone Grafts Introduced Through The Oral Cavity. Plast Reconstr Surg. 1950; 6(4): 295–300.
- Quarrell OW, Koch M, Hughes HE. Maxillonasal dysplasia (Binder’s syndrome). J Med Genet. 1990; 27(6): 384.
- Holmström H, Kahnberg KE. Surgical approach in severe cases of maxillonasal dysplasia (Binder’s syndrome). Swed Dent J. 1988; 12(1–2): 3–10.
- Sun AH, Steinbacher DM. Orthognathic Surgery and Rhinoplasty. Plast Reconstr Surg. 2018; 141(2): 322–9.
- Bhatt YC, Vyas KA, Tandale MS, Panse NS, Bakshi HS, Srivastava RK. Maxillonasal dysplasia (Binder’s syndrome) and its treatment with costal cartilage graft: A follow-up study. Indian J Plast Surg. 2008; 41(2): 151–9.
- Rune B, Åberg M. Bone Grafts to the Nose in Binder’s Syndrome (Maxillonasal Dysplasia): A Follow-Up of Eleven Patients with the Use of Profile Roentgenograms. Plast Reconstr Surg. 1998; 101(2): 297–304.
- Goh RCW, Chen YR. Surgical management of Binder’s syndrome: Lessons learned. Aesthetic Plast Surg. 2010; 34(6): 722–30.