
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Congenital absence of the left circumflex artery associated with RCA dominancy: Case report
Mohammad Shojaie1; Helia Ariapour2*; Reza Elmafshar3
1Professor, Interventional Cardiology, Jahrom University of Medical Science, Jarom, Iran.
2Medical Intern, Jahrom University of Medical Science, Jarom, Iran.
3Assistant Professor of Cardiology, Jahrom University of Medical Science, Jarom, Iran.
*Corresponding Author : Helia Ariapour
Jahrom university of medical science, Jarom, Iran.
Email: drariapour@gmail.com
Received : Jul 25, 2022
Accepted : Aug 12, 2022
Published : Aug 19, 2022
Archived : www.jcimcr.org
Copyright : © Ariapour H (2022).
Abstract
The patient was a 62-years-old man that known case of hypertension for 15 years and had a history of cerebrovascular accident 10 days ago was admitted to our hospital due to chest pain and dyspnea, after evaluation and workups, coronary angiography revealed an absence of left circumflex artery with right coronary artery dominancy.
Keywords: LCX: Left Circumflex Artery; RCA: Right Coronary Artery; RCA dominancy; CALCx: Congenital Absence of the Left Circumflex Artery.
Citation: Shojaie M, Ariapour H, Elmafshar R. Congenital absence of the left circumflex artery associated with RCA dominancy: Case report. J Clin Images Med Case Rep. 2022; 3(8): 2006.
Introduction
Coronary artery abnormalities are one of the most significant disorders that may recognize during coronary angiography with a range of occurrence from 0.64% to 1.3% [1]. This unusual situation called CALCx is a rare coronary anomaly that is reported in a few cases all over the world but on the other hand, it is a benign abnormality that can be classified as, atresia, congenital ostial stenosis, or a new acronym [2,3].
We reported a patient with Congenital Absence of the Left Circumflex Artery (CALCx) that supported the myocardium with the super dominant Right Coronary Artery (RCA).
Case report
We report a case of a 62-year-old man with atypical chest pain and dyspnea since 10 hours ago who was admitted to our hospital. His past medical history was having hypertension for 15 years while was on medication. He reported a history of having angiography 15 years ago and a history of Cerebrovascular Accident (CVA) 10 days ago. The ECG and his physical examination were normal without any considerable signs. Echocardiography reported 50% for Ejection Fraction (EF) amount.
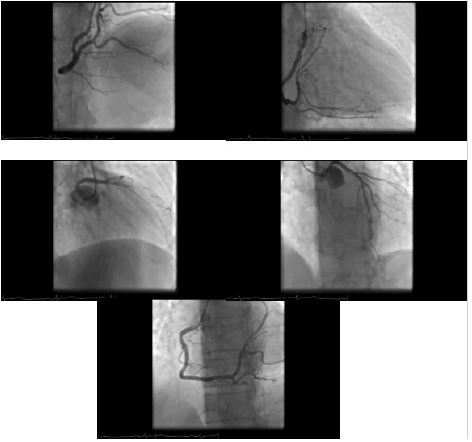
After evaluation and workups, coronary angiography revealed a single LAD with non-significant proximal plaque, absence of LCX and super dominant RCA with a non-significant proximal plaque after PLV branches extended and formed OM branches (Figure 1).
Discussion
In articles, the absence of LCX is typically defined as an extremely rare abnormality of coronary arteries [4]. which occurs due to the abnormal development of the LCX in the left atrioventricular groove [3]. However, some authors believe that this variant is a normal condition that LCX naturally originates from the distal of RCA which is present at birth [5].
Although this condition is defined as a benign disease and has no significant clinical symptoms, it can be symptomatic during childhood or later in life, for example, angina-like symptoms, especially during physical activity, or coronary artery disease, which happened in our case too [6]. The etiology of these symptoms is unknown [7]. In a normal heart, RCA and LCX pass the atrioventricular groove and make a circle to perfuse their territories. In cases with a small or absence of LCX, having a developed and dominating RCA compensates for posterolateral and lateral wall blood supply beside RCA’s natural territory which is the right and inferior heart wall [7,8].
In this case, the absence of LCX hasn’t any particular clinical manifestation for a long time. With LCX’s absence, RCA’s dominancy will become serious [9]. This patient had a very developed dominant RCA.
Conclusion
Dominancy of RCA in the patient with the absence of LCX and passing the full course of the LCX is an uncommon anomaly with no associated harmful incident. RCA perfuse the myocardium remarkably and may not have particular symptoms. In some cases, it may show atherosclerotic coronary artery symptoms with exertion. Recognition of this condition is important for us because atherosclerotic lesions have diminished oxygenation in the myocardium.
References
- Kapur PR, Jain R, Vashist GP. Congenital absence of left circumflex coronary artery: Role of computed tomography coronary angiography. Hong Kong J Radiol. 2014; 17: e1-4.
- Srinivasan KG, Gaikwad A, Kannan BRJ, Ritesh K, Ushanandini KP, et al. Congenital coronary artery anomalies: Diagnosis with 64 slice multidetector row computed tomography coronary angiography: A single-centre study,” Journal of Medical Imaging and Radiation Oncology. 2008; 52: 148-154.
- Jariwala P, Jadhav K, Kale SS. Congenital absence of the left circumflex artery: Case series and review. Asian Cardiovascular and Thoracic Annals. 2021; 29: 826-835.
- Sayit AT, Çamlıdağ İ, Çelenk Ç. Absence of the Left Circumflex Artery Detected by Coronary Computed Tomography Angiography. Istanbul Medical Journal= Istanbul Tip Dergisi. 2019; 20: 574.
- Villa AD, Sammut E, Nair A, et al. Coronary artery anomalies overview: The normal and the abnormal.World J Radiol. 2016; 8: 537-555.
- Varela D, Teleb M, Said S, Fan J, Mukherjee D, Abbas A, et al. Congenital absence of left circumflex presenting after an emotional stressor. Polish journal of radiology. 2015; 80: 529.
- Majid Y, Warade M, Sinha J, Kalyanpur A, Gupta T. Superdominant right sdcoronary artery with absent left circumflex artery. Biomed Imaging Interv J. 2011; 7: e2.
- Rawala MS, Ahmed AS, Iqbal MA, Iqbal A, Budde PK, Rizvi SB. Congenital anomaly of coronary artery: Absence of left circumflex artery. Journal of community hospital internal medicine perspectives. 2019; 9: 140-142.
- Shaikh SS, Deshmukh V, Patil V, Khan Z, Singla R, Bansal NO, et al. Congenital absence of the left circumflex artery with super-dominant right coronary artery: Extremely rare coronary anomaly. Cardiology research. 2018; 9: 264.
- Ullah S, Khan M, Khan NA, Zeb H, Patel R, et al. Absence of left circumflex artery: A rare congenital disorder of coronary arteries. Case reports in cardiology. 2017; 2017.
- Varela D, Teleb M, Said S, et al. Congenital absence of left circumflex presenting after an emotional stressor. Pol J Radiol. 2015; 80: 529–531.
- Pun B, Shrestha A, Karki B, Tuladhar AS. Congenital absence of left circumflex artery with right coronary dominance. Clinical Case Reports. 2021; 9: 570-571.