
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
The impact of psycho-education on health knowledge of depression and adherence to treatment in depressed patients
Arvin Hedayati1; Negin Norouzi1; Seyed Ali Hossein Zahraei2*
1Psychiatry Department, Shiraz University of Medical Sciences, Shiraz, Iran.
2Medical Doctor, Shiraz University of Medical Sciences, Shiraz, Iran.
*Corresponding Author : Zahraei SA Hossein
Medical Doctor, Shiraz University of Medical Sciences, Shiraz, Iran.
Email: zmohsen14@gmail.com
Received : Jul 16, 2022
Accepted : Aug 15, 2022
Published : Aug 22, 2022
Archived : www.jcimcr.org
Copyright : © Hossein ZSA (2022).
Abstract
Depression is a major public health problem associated with increased functional impairment and mortality. In the United States in 2010, the estimated annual direct and indirect medical costs of depression were more than $200 billion.
Depression is very common worldwide and its prevalence has increased over time. For example, two national surveys were conducted on the prevalence of depression in the United States, one in 1991-1992 and the other in 2001-2002. The prevalence of depression has more than doubled during this period (3% and 7%). However, factors such as diagnostic methods may play a role in this increase in prevalence. Major depression is more common than persistent depression [1].
Keywords: Depression; Psychoeducation; Depressed patients.
Citation: Hedayati A, Norouzi N, Hossein ZSA. The impact of psycho-education on health knowledge of depression and adherence to treatment in depressed patients. J Clin Images Med Case Rep. 2022; 3(8): 2009.
Introduction
General
Epidemiology: Depression is a major public health problem associated with increased functional impairment and mortality. In the United States in 2010, the estimated annual direct and indirect medical costs of depression were more than $200 billion.
Epidemiology: Depression is very common worldwide and its prevalence has increased over time. For example, two national surveys were conducted on the prevalence of depression in the United States, one in 1991-1992 and the other in 2001-2002. The prevalence of depression has more than doubled during this period (3% and 7%). However, factors such as diagnostic methods may play a role in this increase in prevalence. Major depression is more common than persistent depression.
Lifetime prevalence: A review of studies conducted in 14 countries has estimated that the prevalence of major depression and persistent depressive disorder (dysthymia) in adults is 12%.
Gender: The prevalence of depression is approximately twice as high in women as in men. A review of studies in 15 countries has shown that the prevalence of depression during life is 1.9 times higher in women than in men. The prevalence of depression in both genders is different because the cause of depression can be different in each gender.
Race: A study in the United States found that the lifetime prevalence of depression was 18% in whites, 13% in black Caribbeans, and 10% in African-Americans. However, depression in Caribbean and African-American blacks was more chronic and associated with more functional impairment compared to whites.
Age: Major depression is more common in young adults than in older adults. A study on 9000 American adults showed that the lifetime prevalence of depression, according to the DSM-IV criteria, was significantly lower in people aged 65 years than in younger age groups (10% vs. 19-23%). The prevalence of spots was significantly lower in the age group of 65 years (1% vs. 3-4%). The prevalence of depression in older adults decreases with age.
Etiology
Pathogen: Depression appears as a group of heterogeneous disorders that are similar in terms of phenotype. Therefore, depression can be considered the final common path of various diseases that occur in a biological, psychological and social chain. Major depression occurs more in people with specific risk factors. These multiple factors are placed in three groups.
1- Internal factors: genetics, neuroticism, low self-confidence, early onset of anxiety disorders, previous history of major depression.
2- External factors: drug use, behavioral disorder, genetics.
3- Exacerbating factors: trauma in childhood or adulthood, stressful life in the past years, loss of parents, low parental warmth, a history of divorce, problems with spouse, low social support, low education. [1]
Signs and symptoms:
-Depressed state: the main feature of depression is depressed state and boredom (dysphoria). Dysphoria can take many forms. Such as feeling sad, disappointed, discouraged, etc.
- lack of enthusiasm and pleasure
-Changes in appetite and weight that can increase or decrease.
-Sleep disorders that are frequently seen in people with major depression, which can manifest as insomnia or hypersomnia.
- Feeling tired and lacking energy
-Functional and cognitive impairment in the form of impairment in attention, concentration, planning, problem solving, memory, fluency and social dysfunction.
-Psychomotor disorder that occurs in the form of restlessness or retardation. Restlessness in the form of excessive and ineffective activity, repetitive tasks, feeling of inner tension. Retardation in the form of slowing down body movements, thinking or speaking.
-Feeling of worthlessness and guilt
-Thinking about suicide or attempting it [2].
Subtypes of depression
Major depression and persistent depressive disorder are heterogeneous syndromes. Based on DSM.IV criteria, the following subtypes are considered for depression.
Anxiety, Atypical, catatonic, Melancholic, Mixed features, Peripartum, Psychotic, Seasonal
Treatment
For the initial treatment of major unipolar depression, pharmacotherapy plus psychotherapy is recommended (instead of pharmacotherapy or psychotherapy alone). Although drug therapy or psychotherapy alone are the answer.
Many combinations of specific antidepressants are available, and no single combination has been proven to be superior to the other. Many classes of antidepressants are available for the treatment of major unipolar depression, and the effectiveness of different antidepressants is comparable in general and among their classes.
For patients with major unipolar depression who are initially treated with antidepressants, we recommend SSRIs over other antidepressants. Although Serotonin-nonepinephrine reuptake inhibitor drugs. Atypical antidepressants and serotonin regulators are good alternatives. Tricyclic antidepressants and monoamine oxidase inhibitors are usually not used for primary treatment because we are concerned about their safety and side effects.
Many psychiatrists are able to treat unipolar depression. For patients who have major unipolar depression and have started their initial treatment with psychotherapy. We recommend Cognitive Behavioral Therapy (CBT) or interpersonal psychotherapy over other psychotherapy methods. Anyway, the rest of the alternative treatment methods include behavioral activation therapy for couples and families, problem solving therapy, psychodynamic psychotherapy and supportive psychotherapy.
Patient education
To promote adherence to treatment, the following should be explained to patients who start psychotherapy at the beginning of treatment:
1- Take the recommended medicines
2- There may be an interval of several weeks until the response to the treatment
3- Complications occur intermittently in the first days, but usually they will be resolved within a week after starting drug therapy.
4- Continuing the treatment even without feeling better and raising complications and any other concerns and questions
Prognosis
Initial treatment of mild to moderate unipolar depression patient question score 15 and does not have features of psychosis and suicidal behavior, with antidepressants 50-60% of patients go towards response and recovery. An analysis of 182 randomized trials has shown that (n>23,000 patients who were treated with antidepressants for an average of 7 weeks) the response was a reduction of more than 50% of symptoms in 54% of patients [3].
Research background
In 2007, Roget and Aubrey conducted a systematic review of the articles on psychological education in bipolar patients published in Pub sMed and Medline until 2006. Most of the studies showed that psychoeducation either alone or as part of more complex interventions caused improvement. The process of the disease is improved by increasing the information of the patient and his family regarding the disease and treatment choices, and reducing the risk of recurrence of manic and depressive episodes and hospitalization, as well as improving the patient’s cooperation. So, according to the results of published studies, psychoeducation should be part of the treatment of bipolar patients [4].
In 2005, Callum and Lam conducted a systematic study on psychoeducation in the recovery of bipolar patients. Using the keywords Bipolar, Psychoeducation, cognitive behavioral, Relapse prevention in Medline articles, current contents conducted a systematic study that showed that psychological treatments are especially useful for preventing relapse in bipolar disorder along with mood stabilizing drugs. Most of the recently published psychotherapy studies showed that psychotherapy has positive results both as a maintenance treatment and as an additional treatment in periods of depression. Psychoeducation increases the patient’s cooperation and satisfaction, increases and early identification of prodromal symptoms, the importance of a regular lifestyle, and also improves patients’ beliefs and awareness of the disease [5].
In 2013, Javadpour and his colleagues conducted a study on the effect of simple psychoeducational programs on quality of life, relapse, or medication adherence in bipolar patients. In this study, 108 patients were equally and randomly divided into two groups, and the control group received only drug therapy, and the intervention group received education in addition to drug therapy. These two groups were followed for two years. The intervention group received 8 50-minute training sessions and was followed up monthly by phone. Each group was evaluated every 6 months for a period of 18 months in terms of quality of life, symptoms of relapse and drug cooperation, and the number of hospitalizations due to relapse of bipolar disease. The result of this study showed that the intervention group had significantly better drug cooperation and quality of life than the control group. Also, the periods of relapse and hospitalization in this group were less than the control group [6].
In 2009, Donker and colleagues conducted a meta-analysis of psychoeducation for depression and anxiety disorders. A search was conducted in cochrane, psycinfo, pubmed in 2008 and a total of 9010 abstracts were found. Of these, five articles that described four researches about passive psychology training in depression and anxiety disorder included the inclusion criteria and after meta-analysis, it was determined that although it is generally believed that psychoeducation has no effect. But this meta-analysis showed that passive training can reduce symptoms for people with depression and anxiety disorders. These interventions are easy, can be applied immediately, and are inexpensive. Studies have shown that the quality of these trainings is important and effective in reducing symptoms [7].
In 2013, Torsi and his colleagues conducted a systematic study on the effect of psychoeducation on depression. LILACS, Psycinfo, Pubmed, SCOPUS and ISI WEB were searched with the keywords Psycho education, psychoeducational intervention and depression. 50 articles were included in the study, of which 13 articles examined the effect of psychoeducation in depressed patients. 10 articles evaluated in-person education and 3 reviewed distance education. In addition to these, an article on psychoeducational interventions for families and the responses of patients’ families was evaluated. The findings show that the increase in education about depression and its treatment is associated with better prognosis and a reduction in psychosocial burden. Psychotherapy is a well-known psychological therapy alongside drug therapy. However, there are few studies on its effectiveness in adults with major depression. Although the publications in this field are limited, the articles selected in this review show that psychoeducation is effective in improving the clinical course, adherence to medication, and psychological and social functioning of depressed patients [8].
In a study on 69 bipolar patients who had experienced at least one recurrence of the disease in the past year, the role of patient education in timely diagnosis and the absence of possible damage from recurrence was confirmed [9].
Materials and methods
Objectives & hypothesis
The main objective:
Determining the effect of psychoeducation on depression health literacy and treatment adherence in depressed patients
Specific objective:
-Determining the effect of psychoeducation on depression health literacy in depressed patients
-Determining the effect of psychoeducation on treatment adherence in depressed patients
-Comparison of the effect of psychoeducation on health literacy based on the severity of depression based on the score obtained from the Hamilton questionnaire.
-Comparison of the effect of psychoeducation on treatment compliance based on the severity of depression based on the score obtained from Moriski questionnaire.
Functional objective:
Using this cheap and simple available method as part of the treatment of patients with major depressive disorder in order to improve the symptoms and outcome of the disease.
Assumptions or research questions:
-Psychoeducation is related to depression health literacy in depressed patients
-Psychoeducation is related to treatment adherence in depressed patients
-The degree of effect of psychoeducation on depression health literacy in depressed patients is related to the severity of depression
Statement of the intervention method (in this part, the evaluation indicators, how to measure them before and after the intervention, the intervention method along with the relevant details, the sample size and the statistical methods used should be mentioned)
Based on previous studies and statistical consultation, the minimum sample size is 212. Number of people for whom outpatient treatment has been started with the diagnosis of depression, it has been determined that according to the entry criteria:
-Age 18 to 60 years
- The ability to work with a mobile phone
- Literacy for reading and writing
- Absence of dementia and mental retardation
And exit criteria:
- The patient’s unwillingness to cooperate
- Suffering from drug abuse at the same time
They enter the study. These people are randomly divided into two intervention and control groups equally. After obtaining written consent to participate in the study and completing the demographic information, the mobile numbers of the people are also taken.
Hamilton’s questionnaire
Morisky questionnaire
Results
The following information was obtained from 212 patients whose information was extracted purely without any problem and divided into two trained and control groups:
In terms of gender, 166 people were female and 46 were male, which is 78% to 22% of the classification.
In terms of age, the patients of each group were classified into three categories: 18-30 years, 30-45 years, and 45-60 years, and a total of 73 people, 92 people, and 47 people were placed in these groups, respectively.
Two important factors in this study included the level of anger and depression, which were calculated in stages through a questionnaire to determine the significance and relationship between education and the changes of these two factors, as well as the relationship between the two factors, considering the significance level of p value less than five percent. were evaluated. The results indicated that education did not have a significant role in the changes of anger in these groups with a p value of 700, which may be due to the knowledge of the disease and its stability, because a person who is informed of the disease in his existence has a lot of anger. It is his attention that shows degrees with or without training anyway.
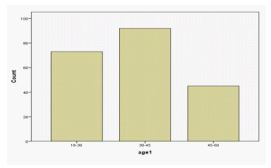
| Age | Number |
|---|---|
| 18-30 | 73 |
| 30-45 | 92 |
| 45-60 | 47 |
Also, the level of anger and the incidence of depression in each group were compared, and again, no significant relationship between the level of depression and anger in the individual, whether in the trained group or in the control group, was observed with P values of 8 percent, 1 percent, and 23 percent, respectively.
In relation to the changes in depression and comparison between the two groups, we came to the conclusion that training had a significant relationship with treatment adherence and reduction in depression scores, which indicated that the p value was less than 500 in each.
Also, no significant relationship was found between the level of literacy and the incidence of depression with a P value of 2 and 33 percent.
Another point from the statistics obtained from the patients was that about 40% of the patients in the two groups had a sense of guilt, which attracted attention after the depressed mood, which is the main characteristic of these patients.
Discussion & Conclusion
According to the results obtained in chapter 4 of this research, we find that despite having a wide age range used in the patients participating in this project, age and age in both trained and witness groups did not have a significant relationship with the incidence of depression.
Also, in spite of many researches conducted in this field, which state that psychoeducation has not had a significant effect in reducing depression disorders, we have seen that in the group where psychoeducation was applied, the effectiveness of treatment and the reduction of depression scores have been observed. Others [5,7,8] have also reported this effect.
Also, in researches in which cases of bipolar disorder were used, this effectiveness was also reported in the recurrence and reduction of the depression phase of this disease. The level of anger and depression did not have a significant relationship with each other, and psychoeducation did not have an effect on reducing anger, which could be due to the patient’s awareness of the disease condition, which, however, has a negative effect on mood and causes anger.
In this study, the level of education and literacy did not have an effect on the reduction of depression symptoms, which is probably due to the external and environmental conditions that caused depression, and the presence of depression symptoms at any level of literacy causes mental discomfort.
From the symptoms that were obtained in the cases of this study in each group by questionnaires, it is possible to mention the feeling of guilt after the depressed mood, which is the basis of the depression disease, which did not find a specific reason for its high prevalence.
It is suggested to use more gender-appropriate cases in future research because the majority of the cases in this research were women.
References
- uptodate 2018 available from: https://www.uptodate.com/contents/unipolar-depression-in-adults-epidemiology-pathogenesis-and neurobiology? topic Ref=91774 & source=see_link
- uptodate 2018 available from: https://www.uptodate.com/contents/unipolar-depression-in-adults-clinical-features? Topic Ref=1722 &source=see_link
- uptodate 2018 available from: https://www.uptodate.com/contents/unipolar-depression-in-adults-and-initial-treatment-general-principles-and prognosis? Search= major % 20 depression % 20 prognosis & source=search_result & selected Title=1~150 & usage_type=default & display_rank=1
- Rouget BW, Aubry JM. Efficacy of psychoeducational approaches on bipolar disorders A review of the literature. Journal of Affective Disorders. 2007; 98: 11-27.
- Colom F, Lam D. Psychoeducation: Improving outcomes in bipolar disorder. European Psychiatry. 2005; 20: 359-364.
- Javadpour A, Hedayati A, Dehbozorgi GR, Azizi A. The impact of a simple individual psycho-education program on quality of life, rate of relapse and medication adherence in bipolar disorder patients. Asian Journal of Psychiatry. 2013; 6: 208-213.
- Donker T, Griffiths KM, Cuijpers P, Christensen H. Psychoeducation for depression, anxiety and psychological distress a meta-analysis. BMC Medicine. 2009; 7: 79-87.
- Tursi MFS, Baes CVW, Camacho FRB, Tofoli SMC, Juruena MF. Effectiveness of psychoeducation for depression: A systematic review. Australian & New Zealand Journal of Psychiatry. 2013; 47: 1019–1031.
- Perry A, Tarrier N, Morriss R, Mc Carthy E, Limb K, et al. Randomised controlled trial of efficacy of teaching patients with bipolar disorder to identify early symptoms of relapse and obtain treatment. Bmj. 1999; 318: 149-153.