
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Biomechanical invasive reconstruction of the distal oblique band of the interosseous membrane with extensor carpi radialis longus in radioulnar instability: A new clinical therapy for athletes
Alberto Giménez Ros1; Vicente J León Muñoz2; Fernando Santonja Medina2; José Luis Calvo Guirado3; Francisco Martínez Martínez2*
1Hospital Universitario Virgen del Castillo de Yecla, avenida de la feria s/n, 30510, Yecla, Murcia, Spain.
2Hospital Clínico Universitario Virgen de la Arrixaca, ctra. Madrid-Cartagena s/n, 30120, El Palmar, Murcia, Spain.
3Associate Research, Universidad Autonoma de Chile; Private Practice Murcia, Spain.
*Corresponding Author : Francisco M Martínez
Hospital Clínico Universitario Virgen de la Arrixaca, ctra. Madrid-Cartagena s/n, 30120, El Palmar, Murcia, Spain.
Email: fmtnez@gmail.com
Received : Jul 26, 2022
Accepted : Aug 16, 2022
Published : Aug 23, 2022
Archived : www.jcimcr.org
Copyright : © Martínez FM (2022).
Abstract
Distal Radioulnar Joint (DRUJ) instability is a pathology without a clear reconstructive procedure. Throughout history, numerous techniques have been described whose objectives have been to increase stability as well as relieve pain. The main stabilizing element is the Triangular Fibrocartilage Complex (TFCC) and, there are also secondary stabilizers among where the Distal Oblique Bundle (DOB) is consistently located. We performed a biomechanical study with three cadaveric arms to verify the influence of DOB on joint stability and performing a new reconstruction technique with hemi tendon of carpi radialis longus extensor to get distal radio cubital stability for fiber cartilage repair. There are positive results in the volar and dorsal displacement of the ulna on the radius with the reconstruction technique presented to restore joint stability. The proposed technique is a valid and biomechanically effective option to restore joint stability as a complement to the repair of the TFCC or as a unique technique if the TFCC is irreparable. This technique became important when you cannot repair TFCC in athletes, the recommended alternative can be done and distal oblique soft plasty.
Keywords: Distal radioulnar joint; Instability; Distal oblique bundle; reconstruction; Biomechanics; Triangular fibrocartilage complex.
Citation: Ros AG, Muñoz VJL, Medina FS, Guirado JLC, Martínez FM, et al. Biomechanical invasive reconstruction of the distal oblique band of the interosseous membrane with extensor carpi radialis longus in radioulnar instability: A new clinical therapy for athletes. J Clin Images Med Case Rep. 2022; 3(8): 2010.
Introduction
The Distal Radioulnar Joint (DRUJ) allows the human forearm pronation and supination. The DRUJ motion is limited to a physiologic range composed with DRUJ stabilizers including bone and soft tissues: The Triangular Fibrocartilage Complex (TFCC), dorsal and palmar radioulnar ligaments, musculotendinous units, primarily the extensor carpi ulnaris and the pronator quadratus. The epidemiology of sports-related injuries of the TFCC has been described in literature suggesting that 3% to 9% of all athletic injuries involve the hand and wrist [1,2]. Elite athletes require the comprehension of each athlete’s set of circumstances and priorities when they got TFCC injury. Is so common in most of the athletes because of the acute and chronic, repetitive loads on the ulnar side of the wrist, are detected by wrist arthroscopy for helping athletes for the quickly return after this preinjury treatment [3]. The main findings of this review are that most patients will return to sport following surgical management of TFC tears. A functional TFCC is important for many athletes but may be especially critical in baseball and tennis players due to TFCC contributes to DRUJ stability and helps the dynamic motion that is essential for power grip. All of them are expected to return to play as rapidly as possible after surgical arthroscopic evaluation of the wrist [4-5]. Fortunately, TFCC injuries with (DRUJ) instability or a distal ulna fracture in football players these are the injuries that are less complicated to be resolved, making the attachment of the ligamentum subcruentum, fracture fixation or TFCC open repair [6]. Ferrara and Cohen wrote that racquet sports have the repetitive impact of the upper extremities increasing the risk of tissue fatigue and injury [7]. Welcome et al. published that the Hand-Arm Vibration (HAV) is directly associated to the Hand-Arm Vibration Syndrome (HAVS), affecting wrist, and arm [8]. Distal Radioulnar Joint (DRUJ) instability is one of the major unresolved problems in hand surgery. Throughout history, numerous techniques have been described whose objectives have been to increase stability as well as relieve pain. These techniques have varied from Triangular Fibrocartilage Complex Repair (TFCC) to rescue procedures arthroplasties in those patients who associate degenerative alterations [9]. Anatomically, we are talking about a very complex joint, stabilized by various structures, among which we can highlight the articular congruence of the sigmoid fossa of the radius with the ulnar head, the TFCC, the square pronator muscles and ulnar extensor of the carpus, and finally the Distal Oblique Band (DOB). This last structure has gained importance in recent years. One of the most common treatments outcomes is the arthroscopic treatment of TFCC tears in adolescents with good to excellent results and overall patient/parent satisfaction was high [10]. DOB is a ligamentous reinforcement of the most distal portion of the interosseous membrane, present in 40, 50, or even 70% of individuals, according to the consulting study, taking its origin in the distal 1/6 of the ulnar diaphysis inserted into the lower edge of the sigmoid fossa of the radius; it intervenes in the stability of DRUJ in all positions of rotation of the forearm. Under normal conditions it is a secondary stabilizer of DRUJ, however, when there is a TFCC lesion, it becomes an important stabilizer of the joint, both in palmar and dorsal deviation [11-14]. Because of this, in recent years various techniques have been developed that try to reconstruct this ligamentous reinforcement [15-20]. Other way to improve the DRUJ stability is to protect wrist band brace in both normal and TFCC-torn wrists [21].The proposed technique wants to validate the biomechanically effective option to restore TFCC in athletes (baseball, racquet, handball, volleyball players and other sports which use their hands), the recommended alternative can be done when the TFCC is irreparable or to complement its repair.
Materials and methods
Procedure
The biomechanical study was carried out at the Institute of Biomechanics of Valencia. Three complete cadaveric arms (which we will call MU18-0207, MU18-0208 and MU18-0210) were available for the study. The specimens were frozen at -25°C and were thawed at room temperature before the measurement processes. Subsequently, the work was carried out with conditions of 22-23°C and a controlled humidity between 39-41%. These three specimens were subjected to the same measurement sequence, in basal conditions, in progressive destabilization and after their reconstruction. Three specimens were chosen in which the dissection found integrity of the CFCT and the presence of BOD (Figure 1).
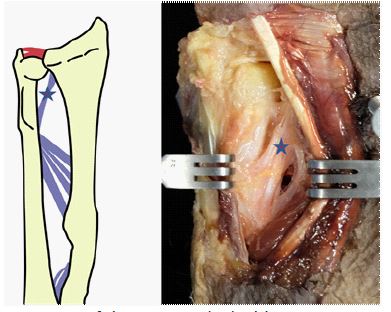
These three specimens were subjected to the same sequence of measurement, progressive destabilization, and reconstruction. Three specimens were chosen in which TFCC integrity and DOB presence were found at the dissection (Figure 1).
The process was subdivided into six phases. In all of them, the same biomechanical measurements of volar and dorsal displacements of the ulna with respect to the radius are made: In the first phase (phase A), the measurements are made with the specimen intact. In phase B, it is measured after detaching the triangular Fibrocartilage (FCT). In phase C, the section of the Distal Oblique Band (DOB) is added. Later in phase D the FCT is repaired, and in phase E reconstruction with the BOD plasty is added. Finally, in phase F, maintaining the BOD reconstruction, the FCT is removed again, to see the isolated effect of the proposed surgical technique.
Surgical technique
First, after having performed the stability measurements of phase A (which will be explained in the stability test), the CFCT is disinserted, severing the dorsal and volar radio-ulnar ligaments from their ulnar insertion (deep insertion or subcruemtum ligament and superficial insertion). Once the measurements of phase B have been made, the BOD is disinserted, separating it subperiosistically from the ulna in its entirety, in order to be able to perform the measurements of phase C. For phase D, the CFCT is reinserted, making a transosseous suture in the ulnar styloid with highly resistant suture.
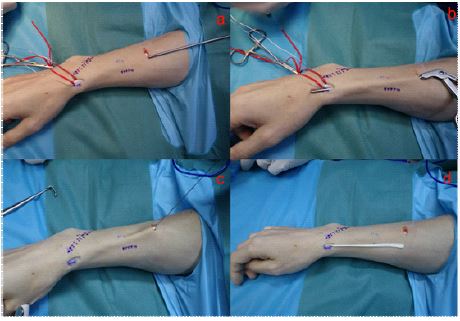
In phase E, we carry out the new proposed technique; To obtain the ERCL autograft (Figure 2), the ERCL tendon is located in the second dorsal gutter and in the myotendinous junction with the aid of ultrasound (it is left referenced with a marker prior to the preparation of the surgical field). Two small longitudinal incisions are made, one at each location. At the distal level, the tendon is subdivided into two equal parts and is crossed with a strand of a fine metallic cerclage, creating a loop over the radial hemitendon that we are going to use. An arthroscopic grasping forceps are introduced through the proximal incision and below the aponeurosis, until reaching the distal incision where the two ends of the cerclage are grasped and it is pulled proximally to divide the tendon along its entire length. In this way, and once the tendon has been divided, the radial half is sectioned in the proximal incision, extracting the fully divided hemitendon from the distal incision with gentle traction.
Once the hemitendon is obtained, the bone tunnels are made with the support of radioscopy and a C guide, which we place in the radius 1 cm proximal to the styloid and in the 1/6 distal of the ulnar diaphysis. With the help of the guide, a 1.6 mm Kirschner needle is passed in an oblique direction from the styloid of the radius to the proximal limit of the sigmoid fossa of the radius; once checked with radioscopy, the brocade is drilled with a 3.5 mm cannulated drill to the second cortical of the radius. To avoid iatrogenesis on the transosseous membrane we perform the same process from the cube, passing the two cortical. Once the hemitendon has been obtained, the bone tunnels are made with fluoroscopy support and with a C-shaped guide, which we place in the radius 1 cm proximal to the styloid and in the distal 1/6 of the ulnar diaphysis (Figure 3).
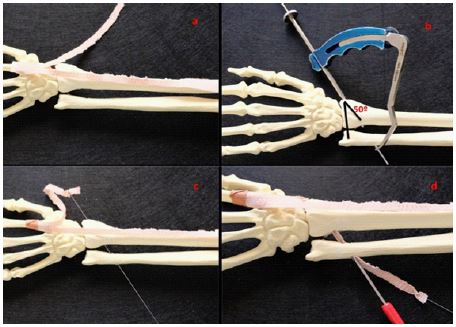
With the aid of the guide, a 1.6 mm Kirschner wire is passed obliquely from the styloid of the radius to the proximal limit of the sigmoid fossa of the radius; Once verified with fluoroscopy, the drill was carried out with a 3.5 mm cannulated drill bit up to the second cortex of the radius. To avoid iatrogenesis on the interosseous membrane, we carry out the same process from the ulna, passing the two cortices. The plasty is prepared with a 4/0 non-absorbable braided suture according to the Krakow technique and to pass the plasty from the radial tunnel to the ulnar one we use a tendon passer or similar from the cubital tunnel, recovering it through the origin of the radial tunnel, introducing the suture of the plasty and by pulling its ends, we proceed to recover the plasty which is fixed in the radial and ulnar tunnels using a 3 x 8 mm biotenodesis screw in each of the tunnels, with the forearm in 60º of supination. Finally the hemitendon is sectioned at its entry into the radius. To finalize phase F of the test, the anchoring suture of the CFCT is cut so that the proposed plasty is the only source of stabilization.
Stability test
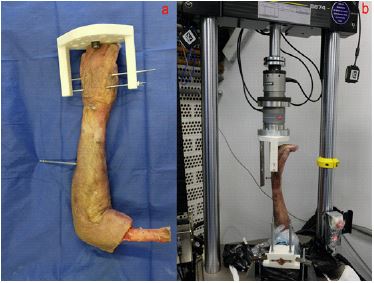
For each condition, the assembly that we will describe below was carried out. The equipment used to carry out all the tests was an INSTRON 8874/711 test machine and a caliper (Figure 4). All the surgical techniques performed were carried out by the same orthopedic surgeon specializing in hand surgery and with the same materials
Three fresh cadaveric pieces have been used where the integrity of the TFC complex and the existence of DOB was previously verified.
The hand was fixed to an auxiliary element, which is anchored to the testing machine, by means of 2 transfixing Kirschner wires on the second to fifth metacarpals; and for the forearm, a 5 mm pin has been inserted in the diaphysis of the ulna, fixing it to the bench of the testing machine. The humerus has been stabilized by means of a sandwich-like jaw to the testing machine in order to keep the elbow at 90º of flexion during the tests. In addition, a screw has been implanted at the level of the third extensor compartment of the wrist, with a vertical direction to measure the volar and dorsal translational movements with respect to a fixed element of the machine.
The operating mode for each of the phases has been:
1) Assembling the arm in the testing machine in the neutral position and taking measurements of the volar and dorsal translation.
2) Measurement of volar and dorsal translation with 60º supination.
3) Measurement of volar and dorsal translation with 60º pronation.
Measurements were made 3 times in each position.
The positions of 60º of pronation and 60º of supination have been reached by controlling the angular displacement at aspeed of application of the same of 3°/s.
The volar and dorsal translation was measured by applying manual pressure on the radius until maximum resistance was found.
After one phase, the surgeon prepares the cadaveric piece for the next phase, and the described process is repeated until all the phases are completed.
Study variables
The main study variables are:
-Volar and dorsal displacement or translation measured in Millimeters (mm). The translation of the radius from the resting position to the dorsal and volar positions was measured, applying manual effort to maximum resistance.
Statistical analysis
The statistical analysis of the data has been developed using an ANOVA (Analysis Of Variances) of a mixed model in which the factors have been the Condition, Repetition, and Random Variables of the Sample in which the measurements have been made.
In this way, the influence of the different stability conditions of the DRUJ has been analyzed, as well as the influence of making several measures (repetition), discounting the variability due to each arm.
The free statistical analysis software R [16] was used in combination with the user interface Deducer [22,23]. The analysis consists of the following points:
1. Descriptive (N, maximum, minimum, mean, and standard deviation).
2. Diagram of study group boxes.
3. ANOVA of the mixed model.
The results obtained are represented graphically using box plots. It has been decided to opt for this type of diagram to provide a graphic summary of the descriptives obtained for each of the configurations, as well as the dispersion and atypical values. Subsequently, the average results of the three specimens have been compared to see if significant differences are detected between the stability conditions of greatest interest:
- The intact state and each of the subsequent stages
- The breakage of the TFC and its corresponding repair
- The rupture of the membrane and the TFC with the repair of the isolated membrane without TFC and with the TFC repaired.
Results
Table 1 shows the results of the stability test classified by sample and condition. The negative sign of the measures of volar displacement only indicates that they were taken in the opposite direction to the measurements on the dorsal. The order of the phases has been altered in the table and graphs, to obtain a faster view of the results, however, the surgical performance and preparation followed the order already mentioned.
Table 1: Stability test results.
| Sample | Condition | Neutral position | Supination 60º | Pronation 60º | |||
|---|---|---|---|---|---|---|---|
| Dorsal (mm) | Volar (mm) | Dorsal (mm) | Volar (mm) | Dorsal (mm) | Volar (mm) | ||
| MU18-0207 | Intact | 12,5 | -9,0 | 9,5 | -4,6 | 2,3 | -2,1 |
| 16,2 | -10,8 | 11,1 | -8,9 | 4,0 | -2,0 | ||
| 16,0 | -12,5 | 20,5 | -7,5 | 3,9 | -2,2 | ||
| Rep TFC | 9,80 | -7,2 | 6,3 | -5,7 | 1,4 | -1,0 | |
| 9,10 | -8,7 | 6,7 | -6,0 | 1,0 | -1,7 | ||
| 9,10 | -7,7 | 6,5 | -5,7 | 1,4 | -1,1 | ||
| Rep Memb | 9,70 | -7,8 | 7,4 | -6,8 | 1,9 | -1,7 | |
| 10,0 | -8,0 | 6,5 | -4,0 | 2,0 | -1,0 | ||
| 10,1 | -9,4 | 7,9 | -6,6 | 1,4 | -1,3 | ||
| Rep Memb+TFC | 9,20 | -7,0 | 5,5 | -6,5 | 1,0 | -1,8 | |
| 8,0 | -7,0 | 6,6 | -6,0 | 2,0 | -1,0 | ||
| 9,0 | -7,5 | 6,4 | -5,8 | 0,5 | -2,0 | ||
| Rot TFC | 14,0 | -12,0 | 21,0 | -10,3 | 4,2 | -4,8 | |
| 16,0 | -12,4 | 22,0 | -8,0 | 4,6 | -3,6 | ||
| 14,9 | -12,2 | 21,8 | -8,0 | 4,4 | -3,1 | ||
| Rot Memb | 20,5 | -13,5 | 24,0 | -11,0 | 6,2 | -3,8 | |
| 16,0 | -14,1 | 20,0 | -10,0 | 6,0 | -4,0 | ||
| 16,8 | -14,0 | 19,4 | -10,1 | 5,8 | -3,2 | ||
| MU18-0208 | Intact | 7,5 | -3,5 | 6,9 | -2,9 | 5,5 | -3,3 |
| 6,2 | -2,3 | 6,2 | -4,0 | 3,5 | -0,5 | ||
| 4,5 | 4,2 | 6,0 | -4,0 | 4,5 | -1,5 | ||
| Rep TFC | 9,8 | -3,8 | 6,5 | -1,7 | 3,4 | -2,5 | |
| 9,0 | -4,4 | 6,4 | -2,1 | 2,0 | -3,0 | ||
| 8,9 | -4,8 | 6,8 | -1,7 | 2,0 | -3,4 | ||
| Rep Memb | 9,8 | -5,2 | 7,5 | -2,5 | 3,0 | -3,2 | |
| 10,0 | -3,3 | 6,3 | -3,3 | 3,0 | -2,9 | ||
| 9,0 | -5,1 | 7,0 | -4,0 | 3,2 | -3,8 | ||
| Rep Memb+TFC | 9,7 | -4,7 | 2,1 | -2,9 | 3,0 | -3,0 | |
| 8,0 | -5,5 | 7,3 | -1,9 | 1,7 | -3,3 | ||
| 7,7 | -3,6 | 6,2 | -2,0 | 2,6 | -3,1 | ||
| Rot TFC | 5,1 | -4,8 | 6,0 | -4,8 | 3,0 | -1,9 | |
| 6,3 | -4,5 | 8,1 | -4,3 | 3,0 | -2,0 | ||
| 6,0 | -4,6 | 7,0 | -4,6 | 2,8 | -2,2 | ||
| Rot Memb | 7,0 | -4,7 | 7,8 | -4,4 | 3,6 | -1,4 | |
| 9,0 | -3,5 | 7,6 | -3,8 | 3,0 | -3,2 | ||
| 8,8 | -3,7 | 3,8 | -5,2 | 1,5 | -2,7 | ||
| MU18-0210 | Intact | 3,1 | 0 | 3,1 | -1,5 | 0,4 | -0,9 |
| 2,7 | -1,1 | 2,5 | -1,5 | 1,8 | -0,2 | ||
| 3,3 | -1,4 | 3 | -0,8 | -0,6 | -2,4 | ||
| Rep TFC | 3,6 | -2,3 | 3,5 | -1,8 | 1,1 | -1,3 | |
| 3,6 | -5,8 | 3,8 | -1,4 | 1,2 | -1,1 | ||
| 3,8 | -3,6 | 3,6 | -3,6 | 0,6 | -1,2 | ||
| Rep Memb | 2,5 | -2,1 | 2,9 | -0,2 | 0,6 | -0,6 | |
| 2,3 | -1,6 | 2,2 | -0,8 | 1,7 | -0,3 | ||
| 2,9 | -1,1 | 1,8 | -0,5 | 0,5 | -0,8 | ||
| Rep Memb+TFC | 2,7 | -1,2 | 1,1 | -0,8 | 0,3 | -0,7 | |
| 2,6 | -0,5 | 1,5 | -0,6 | 1 | 0 | ||
| 2,3 | -2 | 2,3 | -0,5 | 0,2 | -0,8 | ||
| Rot TFC | 2,6 | -2,9 | 3,5 | -1 | 0,8 | -1,2 | |
| 3,5 | -3,8 | 4,5 | -0,7 | 0,8 | -0,7 | ||
| 2,8 | -1,7 | 4 | -1,1 | 0,9 | -0,9 | ||
| Rot Memb | 4,1 | -4,4 | 6,8 | -5,8 | 2,7 | -3,3 | |
| 5 | -6,3 | 5,5 | -6,2 | 2,2 | -2,6 | ||
| 3,9 | -6,8 | 4,5 | -3 | 1,1 | -1,8 | ||
REP: ROT repair; FCT tear: triangular fibrocartilage; BOD: Distal oblique band.
Descriptive volar displacement.
In Table 2, detailing the descriptive extracted from the R program of the mean dorsal displacement in a neutral position, supination, and pronation for each condition.
Table 2: The volar average displacements in the three positions studied is shown.
| Condition | Base | Deviation st | Min | Max |
|---|---|---|---|---|
| Neutro | ||||
| Intact | 8,00 | 5,49 | 2,7 | 16,2 |
| Rep_TFC | 7,41 | 2,83 | 3,6 | 9,8 |
| Rep_Membrane | 7,37 | 3,62 | 2,3 | 10,1 |
| Rep_membrane_TFC | 6,58 | 3,10 | 2,3 | 9,7 |
| Rot_TFC | 10,12 | 6,13 | 3,9 | 20,5 |
| Supination | ||||
| Intact | 7,64 | 5,64 | 2,5 | 20,5 |
| Rep_TFC | 5,57 | 1,46 | 3,5 | 6,8 |
| Rep_Membrane | 5,50 | 2,46 | 1,8 | 7,9 |
| Rep_membrane_TFC | 4,33 | 2,52 | 1,1 | 7,3 |
| Rot_TFC | 10,88 | 8,17 | 3,5 | 22,0 |
| Rot_Membrane | 11,04 | 7,78 | 3,8 | 24,0 |
| Pronation | ||||
| Intact | 2,81 | 2,00 | -0,6 | 5,5 |
| Rep_TFC | 1,57 | 0,82 | 0,6 | 3,4 |
| Rep_Membrane | 1,92 | 1,00 | 0,5 | 3,2 |
| Rep_membrane_TFC | 1,37 | 1,01 | 0,2 | 3 |
| Rot_TFC | 2,72 | 1,56 | 0,8 | 4,6 |
| Rot_Membrane | 3,57 | 1,97 | 1,1 | 6,2 |
Descriptive of dorsal displacement
Table 3 is detailing the descriptive extracted from the R program of the mean dorsal displacement in a neutral position, supination, and pronation for each condition.
Mixed model results
The statistical analysis of the results has been made based on the mixed model and the complete series of the three specimens. Below is the segmented analysis of the displacement results for the three positions in which the arms were studied: neutral position, supination, and pronation.
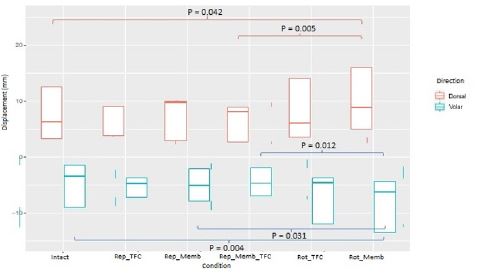
Neutral position displacement: Figure 5 shows the box plot associated with dorsal and volar displacements in a neutral position. Values joined with lines are those that have shown a statistically significant difference, adding the value of this significance.
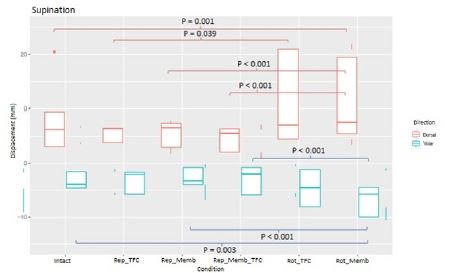
.Supination displacement: Figure 6 shows the box diagram associated with dorsal and volar supination displacement
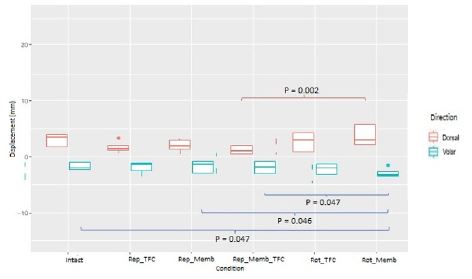
Pronation displacement: Figure 7 shows the diagram of boxes associated with dorsal and volar pronation displacement.
Table 3: The mean of the dorsal displacements in the three positions studied is shown.
| Condition | Base | Deviation st. | Min | Max |
|---|---|---|---|---|
| Neutro | ||||
| Intact | -4,98 | 4,60 | -12,5 | 0,0 |
| Rep_TFC | -5,37 | 2,13 | -8,7 | -2,3 |
| Rep_Membrane | -4,84 | 3,04 | -9,4 | -1,1 |
| Rep_membrane_TFC | -4,33 | 2,65 | -7,5 | -0,5 |
| Rot_TFC | -6,54 | 4,35 | -12,4 | -1,7 |
| Rot_Membrane | -7,89 | 4,61 | -14,1 | -3,5 |
| Supination | ||||
| Intact | -3,97 | 2,75 | -8,9 | -0,8 |
| Rep_TFC | -3,30 | 1,98 | -6,0 | -1,4 |
| Rep_Membrane | -3,19 | 2,46 | -6,8 | -0,2 |
| Rep_membrane_TFC | -3,00 | 2,45 | -6,5 | -0,5 |
| Rot_TFC | -4,76 | 3,46 | -10,3 | -0,7 |
| Rot_Membrane | -6,61 | 2,99 | -11,0 | -3,0 |
| Pronation | ||||
| Intact | -1,68 | 0,99 | -3,3 | -0,2 |
| Rep_TFC | -1,81 | 0,92 | -3,4 | -1,0 |
| Rep_Membrane | -1,73 | 1,26 | -3,8 | -0,3 |
| Rep_membrane_TFC | -1,74 | 1,20 | -3,3 | 0,0 |
| Rot_TFC | -2,27 | 1,35 | -4,8 | -0,7 |
| Rot_Membrane | -2,89 | 0,86 | -4,0 | -1,4 |
Discussion
Based on the observed results in terms of destabilizing the set, the rupture of the TFCC does not cause greater displacement to volar or dorsal in any of the three configurations. Therefore, the breakdown of the TFCC does not seem to cause radio ulnar instability as long as the subject has DOB, as were our cases. Riggenbach proposes a technique that is not percutaneous, and that does not provide any specific graft. It is a reconstruction of the BOD imitating its original anatomy, but we think that the technique has a higher risk of iatrogenic fracture since it makes bone tunnels that leave a cortical bridge of just 3-5 mm [16]. Brink presents a technique that is similar to the one proposed in this article, but with the differences that it uses the palmar long (or palmar major if it does not exist) and they completely dissect it, so it loses its function, in addition to specifying an additional incision [17]. De Vries does a similar technique although it is based on the use of a suspension technique with suture-botton [18]. In the study proposed by Aita and Low the surgical technique is also more aggressive, with the complete loss of the brachioradialis muscle, which they use as a stabilizing graft through a tunnel that crosses the radius and ulna. It also requires the use of a temporary Kirschner needle blocking the joint, which must then be removed [19,20]. On the other hand, the BOD rupture after the TCCC rupture does present significant differences in dorsal and volar in the three positions of the specimens, less in dorsal pronation. These results agree with those obtained by Omokawa nd other authors [21-24]. The effect of the BOD break with respect to the intact specimen seems clear that it destabilizes both in the neutral position and in supination, while the results in pronation suggest that a study with a larger number of specimens could help to elucidate the influence of the break. of the BOD membrane in that position. The dorsal displacement in pronation does not present statistically significant differences, but presents a P very close to the limit of significance. There are significant differences in volar displacement (P = 0.05). In DOB and TFCC repairs, we observe that successive phases of surgical reconstruction do not result in statistically significant differences in dorsal or volar displacements compared to the intact specimen, in any of the three positions. Therefore, we can say that the surgical repair we have performed is effective in stabilizing the radioulnar joint. The repair of the TFC complex in combination with DOB rupture (or the absence there of), reveals statistically significant differences concerning the complete destabilization in the dorsal displacement in supination, while in the rest of the configurations it does not present them. Gymnastic requirements that must be assimilated in the development of coordination, joint mobility, postural adaptation, and dynamism of the motor control, expression skills, and elegance of the technical gesture [25,26]. Furthermore , the artistic gymnastics are sports that put athletes at risk of musculoskeletal disorders such as wrist pain and many injuries , all mainly caused by overuse and repeating the same gestures several times for every type of training [27,28]. Wrist pain and shoulder pain had a statistically significant association with the age of the athletes type of sport and duration of them [29]. Normally the external wrist band brace improved DRUJ stability in both normal and TFCC-torn wrists and reduced the DRUJ instability caused by TFCC tear to a near-normal level. The brace can also be considered for use on a normal wrist for protection against DRUJ injury caused by excessive translation [21]. Finally, the repair of the DOB membrane associated with the reinsertion of the TFCC manages to stabilize in the dorsal and volar all positions, although it does not present important differences with the isolated repair of DOB, and with the results obtained it can be thought that a study with a greater number of cadaveric pieces would achieve statistical significance in all planes. Comparing the proposed technique with others described in the literature, we see that it may be a valid and adequate option. In addition, the reconstruction depends on a Pulvertaft suture, which can be more prone to failure. The tunnels have a similar direction but they do not use a guide as in our case, which allows us to face the tunnels and make the passage of the plasty easier in a minimally invasive technique such as the one we present. Furthermore, at the radial level they drill 5 mm with the greater risk that this entails, and we believe that stabilization dependent on a knot on the autograft itself may have less resistance than fixation with two biotenodesis screws. This can be accomplished thanks to the length of the plasty, which, as demonstrated in the study by Fahandezh-Saddi is usually between 15 and 18 cm in length, which is sufficient for this reconstruction. However, this composition has not been biomechanically evaluated [30].
Non- surgical management forms the first-line treatment for all TFC tears can be done in sports, but if the symptoms persist despite 2 to 6 months surgical treatment should be recommended. Arthroscopic debridement is the recommended treatment for central tears; arthroscopic repair is the recommended treatment for radial, ulnar and peripheral tears. Despite such data, the optimal surgical technique to manage TFC tears is yet to be established [31].
Conclusion
The proposed reconstruction technique, which consists of the percutaneous realization of two 3.5 mm tunnels with a guide and with the hemi tendon of the extensor carpi radialis longus, offers better stabilization than the reinsertion of the CFCT, to the point that associating the repair this or not, it hardly has an impact on stabilization. This surgical technique obtains a firm and stable fixation and equalizes the stability of the intact joint and clearly improves the results of the rupture situation, even over the isolated repair of the CFCT, therefore this reconstruction plasty seems an adequate therapeutic tool reproducible and satisfactory in improving the stability of the distal radioulnar joint.
Declarations
Author contributions: Conceptualization, Alberto Giménez-Ros, Francisco Martínez-Martínez; data curation Vicente J. León-Muñoz, Fernando Santonja-Medina; formal analysis José Luis Calvo-Guirado, Alberto Giménez-Ros; funding acquisition, Alberto Giménez-Ros, Francisco Martínez-Martínez; investigation Alberto Giménez-Ros, Vicente J. León-Muñoz; methodology, Fernando Santonja-Medina, José Luis Calvo-Guirado; project administration Alberto Giménez-Rosresources Francisco Martínez-Martínez; software, Fernando Santonja-Medina, Francisco Martínez-Martínez, supervision Alberto Giménez-Ros, Francisco Martínez-Martínez; validation, Fernando Santonja-Medina, Francisco Martínez-Martínez; visualization Alberto Giménez-Ros, José Luis Calvo-Guirado; writing—original draft preparation, Alberto Giménez-Ros, Francisco Martínez-Martínez; writing—review and editing . Alberto Giménez-Ros, José Luis Calvo-Guirado
Funding: This research received no external funding.
Acknowledgments: To the Institute of Biomechanics of Valencia, where the study was developed and provided the material for its development.
Conflicts of interest: The authors declare no conflict of interest.
References
- Bergfeld JA, Weiker GG, Andrish JT, et al. Soft playing splint for protection of significant hand and wrist injuries in sports. Am J Sports Med 1982; 10: 293–296.
- DeHaven KE, Lintner DM. Athletic injuries: Comparison by age, sport, and gender. Am J Sports Med. 1986; 14: 218–224.
- Ko JH, Wiedrich TA. Triangular fibrocartilage complex injuries in the elite athlete. Hand Clin. 2012; 28: 307-321.
- Harvey NM, Culp RW. Baseball commentary “traumatic TFCC tear”. Hand Clin. 2012; 28: 323-324.
- Baratz ME. Central TFCC tears in baseball players. Hand Clin. 2012; 28: 339.
- Wiedrich TA. The treatment of TFCC injuries in football players. Hand Clin. 2012; 28: 327-328.
- Ferrara L, Cohen AA. Mechanical study on tennis racquets to investigate design factors that contribute to reduced stress and improved vibrational dampening. Procedia Eng. 2013; 60: 397–402.
- Welcome DE, Dong RG, Xu XS, Warren C, McDowell TW, et al. An examination of the vibration transmissibility of the hand-arm system in three orthogonal directions. Int. J. Ind. Ergon. 2015; 45: 21–34.
- Kakar S, Carlsen BT, Moran SL, Berger RA. The management of chronic distal radioulnar instability. Hand Clin. 2010: 26: 517–428.
- Schachinger F, Farr S. Arthroscopic Treatment Results of Triangular Fibrocartilage Complex Tears in Adolescents: A Systematic Review. J. Clin. Med. 2021; 10: 2363.
- Noda K, Goto A, Murase T, Sugamoto K, Yoshikawa H, et al. Interosseous Membrane of the Forearm: An Anatomical Study of Ligament Attachment Locations. J Hand Surg. 2009; 34: 415–422.
- Kitamura T, Moritomo H, Arimitsu S, Berglund LJ, Zhao KD, et al. The biomechanical effect of the distal interosseous membrane on distal radioulnar joint stability: A preliminary anatomic study. J Hand Surg. 2011; 36: 1626–1630.
- Moritomo H. The distal interosseous membrane: Current concepts in wrist anatomy and biomechanics. J Hand Surg. 2012; 37: 1501–1507.
- Moritomo H. The Distal Oblique Bundle of the Distal Interosseous Membrane of the Forearm. J Wrist Surg. 2013; 2: 93–94.
- Marinello PG, Peers S, Bafus BT, Evans PJ. Modified brachioradialis wrap for stabilizing the distal radioulnar joint: Case report. Hand N Y N. 2015; 10: 802–806.
- Riggenbach MD, Wright TW, Dell PC. Reconstruction of the Distal Oblique Bundle of the Interosseous Membrane: A Technique to Restore Distal Radioulnar Joint Stability. J Hand Surg. 2015; 40: 2279–2282.
- Brink PRG, Hannemann PFW. Distal Oblique Bundle Reinforcement for Treatment of DRUJ Instability. J Wrist Surg. 2015; 4: 221–228.
- de Vries EN, Walenkamp MMJ, Mulders MAM, Dijkman CD, Strackee SD, et al. Minimally invasive stabilization of the distal radioulnar joint: A cadaveric study. J Hand Surg Eur Vol. 2017; 42: 363–369.
- Aita MA, Mallozi RC, Ozaki W, Ikeuti DH, Consoni DAP, et al. Ligamentous reconstruction of the interosseous membrane of the forearm in the treatment of instability of the distal radioulnar joint. Rev Bras Ortop. 2018; 53: 184–191.
- Low SL, Clippinger BB, Landfair GL, Criner Woozley K. A Biomechanical Evaluation of the DRUJ After Distal Oblique Bundle Reconstruction. J Hand Surg. 2020; 45: 452. e1-452.e8.
- Shin SH, Park T, Hong E, Kwak DS, Chung YG, et al. Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study. Healthcare. 2022; 10: 828. https://doi.org/10.3390/ healthcare10050828.
- Rizzo ML. Statistical Computing with R, Second Edition. Vienna, Austria: CRC Press; 2019; 387.
- Fellows I. Deducer: A Data Analysis GUI for R. J Stat Softw. 2012; 49: 1–15.
- Omokawa S, Iida A, Kawamura K, Nakanishi Y, Shimizu T, Kira T, et al. A Biomechanical Perspective on Distal Radioulnar Joint Instability. J Wrist Surg. 2017; 6: 88–96.
- Benjamin HJ, Engel SC, Chudzik D. Wrist Pain in Gymnasts: A Review of Common Overuse Wrist Pathology in the Gymnastics Athlete. Curr. Sports Med. Rep. 2017; 16: 322–329.
- Mangone M, Paoloni M, Procopio S, Venditto T, Zucchi B, et al. Sagittal spinal alignment in patients with ankylosing spondylitis by rasterstereographic back shape analysis: An observational retrospective study. Eur. J. Phys. Rehabil. Med. 2020; 56.
- DiFiori JP. Overuse injury and the young athlete: The case of chronic wrist pain in gymnasts. Curr. Sports Med. Rep. 2006; 5: 165–167.
- Wyatt HE, Gittoes MJR, Irwin G. Sport-specific musculoskeletal growth and postural control in female artistic gymnasts: A 12 month cohort study. Sports Biomech. 2020; 19: 258–270.
- Farì G, Fischetti F, Zonno A, Marra F, Maglie A, et al. Musculoskeletal Pain in Gymnasts: A Retrospective Analysis on a Cohort of Professional Athletes. Int. J. Environ. Res. Public Health. 2021; 18: 5460. https://doi.org/10.3390/ ijerph18105460
- Shin SH, Park T, Hong E, Kwak DS, Chung YG, et al. Stabilization of the Distal Radioulnar Joint with or without Triangular Fibrocartilage Complex Tear by an External Wrist Band Brace: A Cadaveric Study. Healthcare. 2022; 10: 828. https://doi.org/10.3390/ healthcare10050828
- Riggenbach MD, Wright TW, Dell PC. Reconstruction of the Distal Oblique Bundle of the Interosseous Membrane: A Technique to Restore Distal Radioulnar Joint Stability. J Hand Surg. 2015; 40: 2279–2282.
- Brink PRG, Hannemann PFW. Distal Oblique Bundle Reinforcement for Treatment of DRUJ Instability. J Wrist Surg. 2015; 4: 221–228.
- de Vries EN, Walenkamp MMJ, Mulders MAM, Dijkman CD, Strackee SD, et al. Minimally invasive stabilization of the distal radioulnar joint: a cadaveric study. J Hand Surg Eur Vol. 2017; 42: 363–369.
- Aita MA, Mallozi RC, Ozaki W, Ikeuti DH, Consoni DAP, et al. Ligamentous reconstruction of the interosseous membrane of the forearm in the treatment of instability of the distal radioulnar joint. Rev Bras Ortop. 2018; 53: 184–191.
- Low SL, Clippinger BB, Landfair GL, Criner Woozley K. A Biomechanical Evaluation of the DRUJ after Distal Oblique Bundle Reconstruction. J Hand Surg. 2020; 45: 452. e1-452.e8.
- Fahandezh Saddi Diaz H. Estudio anatómico del abductor accesorio de la mano y su correlación clinico-ecográfica. Estudio en cadáver [Tesis Doctoral]. [Madrid: Departamento de cirujia]: Universidad Complutense de Madrid; 2015.
- Robertson G, Ang KK, Maffulli N, Simpson CK, Rust PA, et al. Return to sport following surgical management of triangular fibrocartilage tears: a systematic review. Br Med Bull. 2019; 130: 89-103.