
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case series of different courses of methotrexate-associated lymphoproliferative disease with pulmonary involvement
Satoshi Tanaka1*; Hiroki Sugioka1; Riiko Kitou1; Kiyohide Komuta1; Satoshi Tanizaki1; Tomohiro Kanai1; Keiko Matsuoka2; Jun Ishiko3; Junji Uchida1; Kiyonobu Ueno1
1Department of Respiratory Medicine, Osaka General Medical Center, Osaka, Japan.
2Department of Pathology, Osaka General Medical Center, Osaka, Japan.
3Department of Hematology and Oncology, Osaka General Medical Center, Osaka, Japan.
*Corresponding Author : Satoshi Tanaka
Osaka General Medical Center, 3-1-56 Bandai-higashi, Sumiyoshi, Osaka 558-8558, Japan.
Email: satoshi112427@yahoo.co.jp
Received : Jul 27, 2022
Accepted : Aug 18, 2022
Published : Aug 25, 2022
Archived : www.jcimcr.org
Copyright : © Satoshi T (2022).
Abstract
Lymphoproliferative Disorder (LPD) is a complication of Methotrexate (MTX) therapy. Several cases of Methotrexate-Associated Lymphoproliferative Disorder (MTX-LPD) have been reported. However, pulmonary lesions in MTX-LPD are rare. Image findings of MTX-LPD show various patterns. Pneumocystis pneumonia and interstitial pneumonia, which have complex courses, have been reported in MTX-treated patients with lung diseases other than MTX-LPD. Furthermore, the treatment course of MTX-LPD differs from those of other lung diseases and could vary across patients. Here in, we discuss the importance of an accurate MTX-LPD diagnosis through detailed examination and treatment priority depending on the severity of underlying diseases and complications.
Keywords: Rheumatoid arthritis; Methotrexate; Lymphoproliferative disorder; Pulmonary lesion.
Abbreviations: LPD: Lymphoproliferative Disorder; MTX: Methotrexate; PCP: Pneumocystis Pneumonia; IP: Interstitial Pneumonia; RA: Rheumatoid Arthritis; OII-LPD: Other Iatrogenic Immunodeficiency-Associated Lymphoproliferative Disorders; WBC: White Blood Cell; Hb: Hemoglobin; LDH: Lactate Dehydrogenase; CRP: C-Reactive Protein; Β-D-G: 1,3-Β-D-Glucan; KL-6: Krebs Von Den Lungen 6; Sil-2 R: Serum-Soluble Interleukin-2 Receptor; HR-CT: High-Resolution Computed Tomography; TBLB: Transbronchial Lung Biopsy; BAL: Bronchoalveolar Lavage; HLH: Hemophagocytic Lymphohistiocytosis; RECIST: Response Evaluation Criteria In Solid Tumors.
Citation: Tanaka S, Sugioka H, Kitou R, Komuta K, Tanizaki S, et al. A case series of different courses of methotrexate-associated lymphoproliferative disease with pulmonary involvement. J Clin Images Med Case Rep. 2022; 3(8): 2014.
Introduction
Methotrexate (MTX) is an anchor drug in rheumatoid arthritis treatment.
Lymphoproliferative Disorder (LPD) is a complication of low-dose MTX (frequency < 0.1%). There are more reports in Asia (especially Japan) than in Europe and the USA, the reason for which is unknown [1,2]. The World Health Organization classifies MTX-associated LPD (MTX-LPD) under “Other Iatrogenic Immunodeficiency-Associated Lymphoproliferative Disorders (OII-LPDs), with MTX-LPD accounting for most OII-LPDs. In 40%-50% of cases, MTX-LPD develops at extranodal sites (the skin, oral cavity, salivary glands, digestive tract, liver, spleen, and spine) and pulmonary lesions are rare [3]. The pulmonary complications of MTX include infections and Interstitial Pneumonia (IP), besides LPD. The first intervention in MTX-LPD treatment is MTX discontinuation, and in most cases, the disease spontaneously regresses after MTX has been stopped. When MTX-LPD does not regress spontaneously, chemotherapy or radiotherapy is needed, depending on the malignant lymphoma type. Here, we report three cases of MTX-LPD of pulmonary involvement with differing courses.
Case series
Case 1
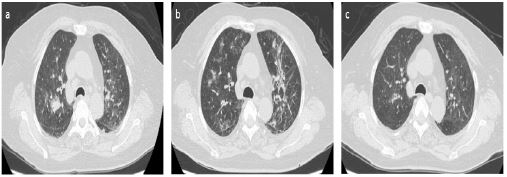
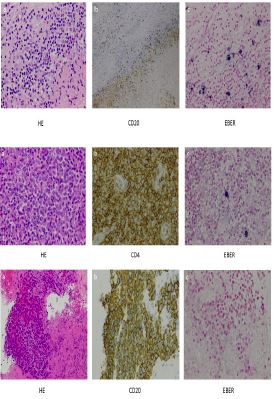
A 76-year-old woman presented with a 1-day history of general malaise and high fever. She had RA and was taking MTX regularly (4 mg/week, 12 years). Laboratory tests revealed White Blood Cell (WBC) and platelet counts of 6600 (/μL) and 7.7 (×10⁴/μL), respectively, and hemoglobin (Hb), Lactate Dehydrogenase (LDH), C-Reactive Protein (CRP), Serum 1,3-Β-D-Glucan (β-D-G), Krebs von den Lungen 6 (KL-6), Serum-Soluble Interleukin-2 Receptor (sIL-2 R) levels of 7.9 g/dL, 625 (IU/L), 10.00 (mg/dL), < 11.0 pg/mL, 361 U/mL, 6140 U/mL, respectively. High-Resolution Computed Tomography (HR-CT) showed cervical, supraclavicular and mediastinal lymphadenopathies, multiple nodules, and ground-glass opacities in both lungs (Figure 1Aa). Histological examination of a biopsied sample of the right submandibularlymph node revealed extensive necrosis. Immunohistology showed CD20 and CD79a expression (Figure 2A). The systemic lymph nodes that were swollen shrank after MTX discontinuation, and sIL-2 R decreased. However, the bilateral ground-glass opacities deteriorated (Figure 1Ab). Bronchoscopy (Transbronchial Lung Biopsy [TBLB] and Bronchoalveolar Lavage [BAL]) was performed. TBLB revealed no significant findings; however, lymphocytes were predominant and CD4 /CD8 ratio was 0.4. On the other hand, BAL fluid was positive for Pneumocystis jirovecii DNA, and the β-D-Glevel was elevated (30.4 pg/mL). Therefore, the patient was diagnosed with Pneumocystis Pneumonia (PCP). Her respiratory condition was good, and she was followed up without antibiotics therapy. Her lung shadow improved (Figure 1Ac), and the β-D-Glevel decreased gradually.


Case 2
A 72-year-old man presented with a 1-week history of general malaise and high fever. He had RA and was taking MTX regularly (16 mg/week, 2 years). Laboratory findings revealed WBC and platelet counts of 31900 (/μL) and 4.4 (×10⁴/μL), respectively; Prothrombin Time-International Normalized Ration (PT-INR) of 1.4; and Hb, LDH, CRP, blood urea nitrogen, creatinine, D-dimer, β-D-G, KL-6, and sIL-2 R levels of 9.7 g/dL, 586 (IU/L), 13.19 (mg/dL), 44 (mg/dL), 2.11 (mg/dL), 41.3 (μg/mL), < 11.0 pg/mL, 242 U/mL, and 58100, U/mL respectively. HR-CT showed cervical, supraclavicular, mediastinal, axillary, and inguinal lymphadenopathies; multiple granular shadows; infiltration shadows; bilateral bronchial wall thickening, predominantly distributed in the lower lung fields; hepatomegaly; and splenomegaly (Figure 1Ba). Hemophagocytic lymphohistiocytosis and disseminated intravascular coagulation were suspected. First, MTX was discontinued, and the patient was started on antibiotics and leucovorin calcium rescue. His inflammatory response and cytopenia (Hb and platelet count) improved; however, multiple lymphadenopathies did not shrink. Lymph node biopsy was performed on the right inguinal lymph node. Histologic tests showed the normal lymph node structure was destroyed. Immunohistology showed CD3, CD4, CD5 and CD7 expression (Figure 2B). He was diagnosed with Peripheral T-cell lymphoma, not otherwise specified. Therefore, systemic chemotherapy with pirarubicin (Tetrahydropyranyladriamycin [THP]), cyclophosphamide, vincristine, and prednisolone (THP-COP regimen) was initiated, and six cycles were administered in all. Partial response in the form of shrinking of systemic lymphadenopathy was noted after six cycles (Response Evaluation Criteria in Solid Tumors: RECIST version 1.1) (Figure 1Bb).
Case 3
A 77-year-old man presented with a 1-month history of back pain and dyspnea on effort. He had RA and was regularly taking MTX (10 mg/week, 19 years). Laboratory tests revealed LDH, CRP, β-D-G, KL-6, neuron specific enolase, and sIL-2 Rlevels of 428 (IU/L), 3.02 (mg/dL), < 11.0 pg/mL, 454 U/mL, 62.2 ng/mL, and 1360 U/mL, respectively. HR-CT showed supraclavicular, mediastinal, axillary and peritoneal lymphadenopathies; a tumor shadow in the left lower lobar bronchus; atelectasis of the left lower lobe; left pleural effusion; and splenomegaly (Figure 1Ca). Lung cancer was suspected, and bronchoscopy was performed. Bronchoscopy revealed tumor exposure in the left main bronchus (Figure 1Ccd), however he could not be diagnosed even after two bronchoscopies. Histological tests performed after the third bronchoscopy revealed a lymphoid cell cluster with necrotic tissue. Immunohistology showed CD20 expression (Figure 2C). MTX was discontinued; however, multiple lymphadenopathies and tumor did not shrink. Thus, systemic chemotherapy with rituximab and a THP-COP regimen was started; in all, six cycles were administered. Complete response in the form of systemic lymphadenopathy shriniking was achieved after six cycles (RECIST version 1.1) (Figure 1Cb).
Discussion
MTX-LPD was first reported as lymphoma in an MTX-treated RA patient [4]. RA alone increases the risk of developing LPD by 2- to 4-fold [5]. Antirheumatic drugs further increase this risk (MTX, 1.7-fold; infliximab, 2.6- fold; etanercept, 3.8- fold) [6]. Per its clinical course, MTX-LPD is classified into three groups: regressive LPD without relapse/regrowth, regressive LPD with relapse/regrowth event, and persistent LPD [7]. Case 1 fall under the regressive LPD without relapse/regrowth group, however Case 2 and Case 3 fall under persistent LPD. The ration of the three groups was similar. Approximately 50% of cases show spontaneous regression with only MTX discontinuation [8]. CT of pulmonary lesions in MTX-LPD has shown various patterns; however, no specific shadows have been reported [9]. MTX-LPD can cause various complications; therefore, it may not have characteristic shadows. The histologic patterns of MTX-LPD are heterogeneous; however, diffuse large B-cell lymphomais the most common histologic type (58%), followed by classical Hodgkin’s lymphoma (15.3%) [3]. Some cases (25%, particularly the regressive group) could not be classified into a particular histologic type, because in these cases, MTX had already been discontinued and MTX-LPD was regressing at the time of biopsy [10]. Although it may be clinically difficult, a biopsy should be performed before MTX discontinuation, if possible. MTX-associated pulmonary complications include infections and IP, besides LPD. The percentages of patients with LPD, infection, and IP were 42%, 25%, and 33%, respectively, among MTX-treated RA patients [2]. In Case 1, MTX-LPD and PCP developed simultaneously. In this case, PCP was detected very early and improved only by follow-up. No detailed mechanism has been found, however changes in the immune status due to underlying diseases or administration of immunosuppressive drugs might affect the inflammatory process of PCP [11]. In Case 1, immune status seems to have changed rapidly after discontinuation of MTX.
There are many reports of MTX-LPD being associated with a high prevalence of Epstein-Barr Virus (EBV) infection, and EBV reactivation contributes to MTX-LPD development. MTX-LPD with EBV positivity is more spontaneously remissive compared to that with EBV negativity [12]. Among our cases, EBV positivity was the highest in case 1, as determined by EBV-encoded small RNA in situ hybridization staining. In case 1, multiple lymphadenopathies shrank after only MTX discontinuation; on the other hand, chemotherapy was required in case 2 and 3.
Conclusion
In conclusion, we described three cases of MTX-LPD with pulmonary involvement, and the disease course was different in each case. MTX-LPD with pulmonary lesions can show various shadows on imaging and cause complications. Therefore, careful attention is required for diagnosis and treatment in cases of suspected MTX-LPD with pulmonary lesions.
Disclosure statement
Author contribution statement: All authors participated in the treatment of this case, and the first author drafted the manuscript. All authors read and approved the final manuscript.
Conflict of interest: The authors declare no conflicts of interest.
Founding statement: This study has no funding.
Acknowledgements: We are grateful to Dr. Makoto Takeuchi for assistance with immunostaining linked to EBV-encoded small RNA in situ hybridization.
References
- Kaneko Y. Methotrexate-associated lymphoproliferative disorder. Nihon Rinsho Meneki. Gakkai Kaishi. 2017; 40: 174-178.
- Thaniyan A, Ayman FFA, Mirghani HO, Al-Sayed BA, Merghani TH, et al. Histopathological features of methotrexate induced pulmonary lesions in rheumatoid arthritis patients: A systematic review of case reports. Open Access Maced J Med Sci. 2017; 5: 266-270.
- Swerdlow SH, Campo E, Harris NL, et al. WHO Classification Tumors of Haematopoietic and Lymphoid Tissues. Immunodeficiency-Associated Lymphoproliferative Disorders. revised fourth edition, IARC publications. 2017; 443-464.
- Ellman MH, Hurwitz H, Thomas C, Kozloff M. Lymphoma developing in a patient with rheumatoid arthritis taking low dose weekly methotrexate. J Rheumatol. 1991; 18: 1741-1743.
- Anderson LA, Gadalla S, Morton LM, Landgren O, Pfeiffer R, Warren JL, et al. Population-based study of autoimmune conditions and the risk of specific lymphoid malignancies. Int J Cancer. 2009; 125: 398-405.
- Wolfe F, Michaud K. Lymphoma in rheumatoid arthritis: the effect of methotrexate and anti-tumor necrosis factor therapy in 18572 patients. Arthritis Rheum. 2004; 50: 1740-17451.
- Tokuhira M, Watanabe R, Nemoto T, Sagawa M, Tomikawa T, et al. Clinicopathological analyses in patients with other iatrogenic immunodeficiency associated lymphoproliferative diseases and rheumatoid arthritis. Leuk Lymphoma. 2012; 53: 616-623.
- Takanashi S, Aisa Y, Ito C, Arakaki H, Osada Y, Amano Y, et al. Clinical characteristics of methotrexate-associated lymphoproliferative disorders: Relationship between absolute lymphocyte count recovery and spontaneous regression. Rheumatol Int. 2017; 37: 1629-1633.
- Arakawa H, Yamasaki M, Kurihara Y, et al. Methotrexate-induced pulmonary injury: Serial CT findings. J Thorac Imaging. 2003; 18: 231.
- Makihara S, Kariya S, Noujima-Harada M, Ohara N, Naito T, et al. Methotrexate-associated lymphoproliferative disorder with multiple pulmonary nodules and bilateral cervical lymphadenopathy. Auris Nasus Larynx. 2019; 46: 927-933.
- Tanaka Y, Saraya T, Kurai D, Ishi H, Takizawa H, et al. Spontaneous resolution of Pnemocystis jirovecii pneumonia on high-resolution computed tomography in a patient with renal cell carcinoma. Am J Case Rep. 2014; 15: 496-500.
- Ichikawa A, Arakawa F, Kiyasu J, Sato K, Miyoshi H, Niino D, et al. Methotrexate/ iatrogenic lymphoproliferative disorders in rheumatoid arthritis: Histology, Epstein-Barr virus, and clonality are important predictors of disease progression and regression. Eur J Haematol. 2013; 91: 20-28.