
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Severe pulmonary mucorales superinfection in three influenzapatients with and without influenza-associated aspergillosis
Frederike Waldeck1,2*; Pedro David Wendel Garcia3; Filippo Boroli4; Noémie Suh4; Katia Boggian2; Valentina Silvia Nastasel5; Daniel Kirschenbaum6; Govind Oliver Sridharan7; Marco Maggiorini3; Gian Reto Kleger8; Werner C Albrich2
1Division of Infectious Diseases and Microbiology, University hospital Schleswig Holstein, Campus Lübeck, Germany.
2Division of Infectious Diseases and Hospital Epidemiology, Cantonal Hospital St. Gallen, St. Gallen, Switzerland.
3Institute of Intensive Care Medicine, University Hospital Zurich, Zurich, Switzerland.
4Division of Intensive Care, Geneva University Hospitals, Geneva, Switzerland.
5Department of Pathology and Molecular Pathology, University Hospital Zurich, Zurich, Switzerland.
6Institute of Neuropathology, University Hospital Zurich, Zurich, Switzerland.
7Division of Intensive Care, Fribourg Hospital, Fribourg, Switzerland.
8Division of Intensive Care, Cantonal Hospital St. Gallen, St. Gallen, Switzerland.
*Corresponding Author : Frederike Waldeck
Division of Infectious Diseases and Microbiology, University hospital Schleswig-Holstein, Campus Lübeck, Ratzeburger Allee 160, 23538 Lübeck, Germany.
Email: Frederike.waldeck@uksh.de
ORCID: 0000-0002-1692-5521
Received : Jul 28, 2022
Accepted : Aug 19, 2022
Published : Aug 26, 2022
Archived : www.jcimcr.org
Copyright : © Waleck F (2022).
Abstract
Mucormycosisis an opportunistic fungal disease which affects immunocompromised hosts including patients with haematologic malignancies and poorly controlled diabetes mellitus. Mucorales grow invasively and are associated with high mortality even if promptly diagnosed. Viral infection like influenza can cause severe pneumonia and is associated with pulmonary aspergillosis. Here we report three separate cases of Mucorales super infection in critically-ill patients with influenza infection, one of them histologically confirmed. Two patients also had influenza-associated pulmonary aspergillosis. Two patients had fatal clinical outcome despite intensive care. The simultaneous detection of these two rare mold infections in patients with severe influenza is highly remarkable and calls for increased awareness.
Keywords: Influenza; Influenza-associated aspergillosis; Mucormycosis; Intensive-care; Invasive mycosis.
Abbreviations: ARDS: Acute Respiratory Distress Syndrome; BAL: Bronchoalveolar Lavage; ECMO: Extracorporeal Membrane Oxygenation, EORTC: European Organization for Research and Treatment of Cancer, IAPA: Influenza-Associated Pulmonary Aspergillosis; ICU: Intensive Care Unit; PCR: Polymerase Chain Reaction, RRT: Renal Replacement Therapy.
Citation: Waldeck F, Garcia PDW, Boroli F, Suh N, Boggian K, et al. Severe pulmonary mucorales superinfection in three influenza patients with and without influenza-associated aspergillosis. J Clin Images Med Case Rep. 2022; 3(8): 2016.
Introduction
Influenza represents an independent risk factor for invasive aspergillosis [1] with substantial morbidity and mortality (33-67%) [2]. Recent corticosteroid use but not classical risk factors for pulmonary aspergillosis predispose to Influenza-Associated Pulmonary Aspergillosis (IAPA) [1,2]. Mucormycosis is another less common mold infection responsible for 4% of mycosis cases in autopsy studies. It affects patients with a range of predisposing immunosuppressive conditions particularly hematologic malignancies, hematopoietic or solid organ transplantation, corticosteroid use, trauma, burns and poorly controlled diabetes mellitus [3,4]. Diagnosis of mucormycosis is difficult and requires histopathological confirmation of tissue invasion as galactomannan and beta-D-glucan are negative. Despite antifungal therapy and aggressive surgical debridement mortality reaches up to 50% [3,4].
As part of a retrospective study of patients with influenza treated in the Intensive Care Unit (ICU) including 157 patients with severe influenza infection in Switzerland during the 2017/18 and 2019/2020 influenza seasons [5]. We identified three (1.9%) Mucorales superinfections. Two patients also had invasive pulmonary aspergillosis.
Case 1
A 59 year old white farmer was admitted to an Austrian primary care hospital with worsening dyspnoea for one week, cough with purulent sputum, headache and fevers. He had been previously treated as an outpatient for suspected exacerbation of chronic obstructive pulmonary disease with antibiotics and corticosteroids. On admission he had mild hypoxemia, mildly elevated inflammation markers and a minimal right upper lobe infiltrate. Corticosteroids were initiated and on day four piperacillin/tazobactam was added for new infiltrates in both upper lobes and fever. On day six he was intubated now fulfilling criteria for Acute Respiratory Distress Syndrome (ARDS). Inflammatory markers spiked and multi-organ (respiratory, cardiovascular, renal, hepatic) failure developed. Bronchoalveolar lavage (BAL) revealed influenza B on PCR and fungal elements on microscopy. Voriconazole and oseltamivir were started. He was transferred to a tertiary care center where veno-arterial Extra Corporeal Membrane Oxygenation (ECMO) was initiated due to refractory hypoxemia complicated by in-hospital hypoxic cardiac arrest. Acute myocardial infarction and severe cardiogenic shock developed. Despite maximal supportive measures he died on day eight. Growth of Aspergillus fumigatus and Lichtheimia corymbifera was reported only post-mortem from the initial BAL. No bacterial pathogen was identified by culture, multiplex PCR or urinary antigensfor Legionella and pneumococcus. No biopsy during bronchoscopy for histological examination or autopsy was performed.
Case 2
A 58 year old white male was admitted to a primary care hospital with fever, cough with purulent sputum, myalgia and diarrhea for four days. He smoked and drank alcohol daily. On admission, he had mild hypoxemia, increased inflammatory markers, acute renal failure and bibasal consolidations. Ceftriaxone and clarithromycin were started for community-acquired pneumonia. Sputum culture was negative. Despite a positive PCR for influenza A from oropharyngeal swab antiviral treatment was initially withheld. Severe ARDS, anuria and septic shock developed by day two. Invasive mechanical ventilation, Renal Replacement Therapy (RRT) and vasoactive support were initiated and therapy was escalated to cefepime and levofloxacin and low-dose corticosteroids for septic shock.
Because of refractory hypoxemia he required veno-venous ECMO implantation and was transferred to a tertiary hospital on day five. BAL cultures grew Aspergillus spp. and PCR remained positive for Influenza A. High-dose oseltamivir (150 mg every 12 h) and voriconazole were started. Due to persistent influenza virus detection and no respiratory improvement, intravenous zanamivir replaced oseltamivir and imipenem previous antibiotics on day 12. Cultures of BAL on day 14 revealed growth of Rhizomucor pusillus and voriconazole was replaced by liposomal amphotericin B. Intravenous corticosteroids were started on day 20 as rescue therapy for non-resolving ARDS. No bacterial pathogen was detected, and antibiotics were discontinued on day 24. Posaconazole was added on day 32 because of persistently positive galactomannan and detection of Aspergillus spp. in several BALs and bronchial biopsies.
Respiratory and renal functions eventually improved, ECMO and RRT were removed on day 29. Due to persistent invasive aspergillosis and undetectable plasma posaconazole levels, voriconazole was reintroduced on day 51, while continuing liposomal amphotericin B. On day 65, progression of invasive aspergillosis documented by a new pulmonary biopsy motivated a switch from voriconazole to caspofunginplus nebulised amphotericin B according to antifungal susceptibility testing. This treatment was maintained until discharge on day 130 without respiratory and renal supportive therapy.
Case 3
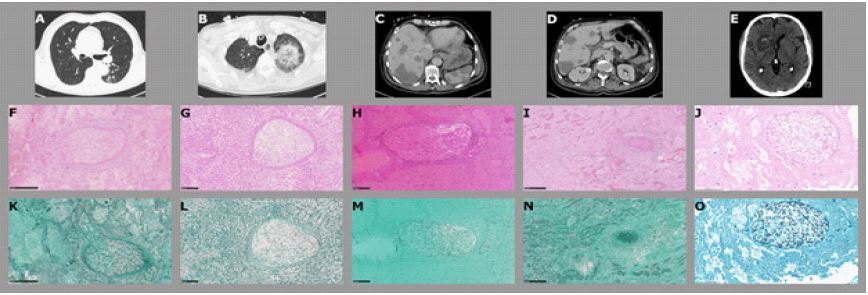
A 72 year old male with newly diagnosed Myelodysplastic Syndrome (MDS) was admitted to a tertiary care hospital with persisting fever and dry coughs. On admission, slightly elevated CRP and neutropenia but no infiltrates on chest x-ray were present. Cefepime was initiated empirically and oseltamivir added after detection of influenza A (PCR) from nasopharyngeal swab. On day 8 and after clinical improvement he received induction chemotherapy with daunorubicin and cytarabine. On day 19 he deteriorated with fever, increasing inflammatory biomarkers and new pulmonary infiltrates (Figure 1A). Therapy was escalated to meropenem, voriconazole and, when blood cultures grew Staphylococcus haemolyticus, vancomycin. He was protectively intubated when left hemiparesis and slurred speech developedon day 22. CT-scan revealed multiple hypodense lesions in brain, liver, kidneys, spleen and lungs (Figure 1B-1E). Due to the morphology of the lesions and new epithelial livid maculae on trunk and extremities voriconazole was replaced by liposomal amphotericin B and posaconazole. Blood cultures, panfungal PCRs of blood, tracheal secretions and BAL did not detect any infectious pathogens. On day 25 skin biopsies revealed focal epidermal necrosis with intravascular fungal thrombosis. On the same day, he developed fulminant right-sided heart failure and suffered cardiac arrest. Reanimation was unsuccessful.Autopsy revealed a severe angio-invasive mucormycosis with massive cerebral, hepatic, renal and splenic involvement, as well as bilateral fungal pneumonia with abscesses and panlobular necrosis (Figure 1F-1O).
Discussion
We report three rare cases of Mucorales respiratory superinfection in patients with influenza, two of them also with IAPA, one histologically confirmed. The simultaneous identification of these two rare mold infections in patients with severe influenza infection is highly remarkable.
Influenza-associated mucormycosis is extremely rare as is coinfection with Aspergillus and Mucorales independent of influenza. Angio-invasive mucormycosis was first described histopathologically in a fatal influenza A H1N1 virus infection in 2009/2010 without clinical details [6]. In a recent case report and review of literature eight cases of influenza-associated mucormycosis have been described with a mortality of 37.5% [7]. One case of proven disseminated mucormycosis and IAPA was recently described [8].
Healthy patients with influenza do not fulfil revised EORTC host criteria for invasive fungal disease. Therefore new criteria for IAPA have been proposed [1,9] which are fulfilled by two of our cases. Case 3 had histologically proven mucormycosis. As with IAPA the diagnosis of mucormycosis in influenza infection is equally problematic since host criteria are not fulfilled. Due to lack of histopathologic samples in two patients we cannot ultimately exclude that detection of Mucorales in BAL represented colonisation. In a review of 66 cases with Mucorales spp. detection in lung, skin/soft tissue and sinus, 55% were clinically asymptomatic likely representing colonisation. Patients with invasive fungal disease had worse outcome than those colonised [10]. The rarity of Mucorales in our two hospitals, the severe clinical course and the extensive patchy pulmonary infiltrates support mold infection rather than colonisation.
Patients with pulmonary mucormycosis are typically severely immunocompromised but few cases of pulmonary mucormycosis in immunocompetent patients with underlying pulmonary disease -as in case 1-have been reported. A case series of 851 cases with mucormycosis included 18.3% without predisposing disease [4] but corticosteroid use was present in every third patient. Two of our cases did not have underlying immunosuppression but received corticosteroids. The third case had newly diagnosed MDS, chemotherapy and steroids. In-vitro and murine studies indicate that neuraminidase inhibition in combination with corticosteroids decreases immune response by impairing cytokine production in response to Aspergillus spp [11], leading to increased susceptibility to mold infection in influenza. Corticosteroids are associated with an increased risk of IAPA [1], increased influenza-mortality and also predispose to mucormycosis [4] and aspergillosis. Corticosteroids have been proposed by Ahmadikia et al. as a risk factor for mucormycosis in viral infection [7] and might have been a major risk factor for the development of invasive mucormycosis in cases 1 and 2 of our series. We hypothesize that influenza not only predisposes to aspergillosis but might predispose to mucormycosis because of extensive tissue damage and impaired local host defence [9,12]. Further studies are needed to study the pathogenesis and the burden of mucormycosis in influenza infection.
In absence of biomarkers for mucormycosis and the requirement of fungal cultures for diagnosis, it is conceivable that prior cases of superinfection with Mucorales in patients with influenza and with IAPA might have been missed. Voriconazole is standard treatment of IAPA but not efficacious against Mucorales. Due to the high mortality of IAPA [1,2] additional etiologic testing might not be performed even in those failing voriconazole, further suggesting that Mucorales coinfection might be overlooked. Given the need for radical combined treatment a low index of suspicion of mucormycosis is critical to improve the otherwise dismal prognosis.
Conclusion
In summary, we report three patients with influenza-associated mucormycosis with and without IAPA. We consider these very important findings due to the severity of the clinical presentation. Given potential underreporting of this severe superinfection and implications for treatment, there should be greater awareness and a low threshold for obtaining respiratory specimens for fungal culture from critically ill patients with influenza in order to confirm our observations.
Declarations
Conflict of interest: None.
Funding: This work was supported by the Swiss research network on fungal diseases (FUNIGNOS, research granted on 5.12.2019) and the research funding of the cantonal hospital of St. Gallen (project number 19/23 2019).
References
- Schauwvlieghe AFAD, Rijnders BJA, Philps N, et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. The Lancet Respiratory Medicine. 2018; 6: 782–792. https://doi.org/10.1016/S2213-2600(18)30274-1.
- Crum Cianflone NF. Invasive Aspergillosis Associated With Severe Influenza Infections. Open Forum Infectious Diseases 2016; 3: of w171. https://doi.org/10.1093/ofid/ofw171.
- Roden MM, Zaoutis TE, Buchanan WL, et al. Epidemiology and Outcome of Zygomycosis: A Review of 929 Reported Cases. Clinical Infectious Diseases 2005; 41: 634–653. https://doi.org/10.1086/432579.
- Jeong W, Keighley C, Wolfe R, et al. The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clinical Microbiology and Infection 2019; 25: 26–34. https://doi.org/10.1016/j.cmi.2018.07.011.
- Waldeck F, Boroli F, Suh N, et al. Influenza-associated aspergillosis in critically-ill patients—a retrospective bicentric cohort study. Eur J Clin Microbiol Infect Dis 2020. https://doi.org/10.1007/s10096-020-03923-7.
- Bal A, Suri V, Mishra B, et al. Pathology and virology findings in cases of fatal influenza A H1N1 virus infection in 2009-2010: Pathology and virology findings of H1N1 infection. Histopathology. 2012; 60: 326–335. https://doi.org/10.1111/j.1365-2559.2011.04081.x.
- Ahmadikia K, Hashemi SJ, Khodavaisy S, et al. The double-edged sword of systemic corticosteroid therapy in viral pneumonia: A case report and comparative review of influenza-associated mucormycosis versus COVID-19 associated mucormycosis. Mycoses. 2021; 64: 798-808. doi:10.1111/myc.13256
- Aqsa A, Droubi S, Glaser A. Aspergillus and Rhizopus Fungal Coinfection in a Patient with Multiple Myeloma. Cureus 2020. https://doi.org/10.7759/cureus.8050.
- Verweij PE, Rijnders BJA, Brüggemann RJM, et al. Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: An expert opinion. Intensive Care Med 2020; 46: 1524–1535. https://doi.org/10.1007/s00134-020-06091-6.
- Langford S, Trubiano JA, Saxon S, Spelman D, Morrissey CO, et al. Mucormycete infection or colonisation: experience of an Australian tertiary referral centre. Mycoses 2016; 59: 291–295. https://doi.org/10.1111/myc.12467.
- Van de Veerdonk FL, Dewi I, Cunha C, van der Beek L. Inhibition of host neuraminidase increases susceptibility to invasive pulmonary aspergillosis, OFID; 2018.
- McCullers JA. The co-pathogenesis of influenza viruses with bacteria in the lung. Nature Reviews Microbiology 2014; 12: 252–262. https://doi.org/10.1038/nrmicro3231.