Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Elevated serum Carbohydrate Antigen (CA) 19-9 level in a patient with uncontrolled diabetes mellitus
*Corresponding Author : Zeinab Hassan Toufaili
Family Medicine Consultant, Primary Health Care Corporation, Qatar.
Phone: 97433623493;
Email: drzeinabtoufaili@gmail.com
Received : Jul 28, 2022
Accepted : Aug 22, 2022
Published : Aug 29, 2022
Archived : www.jcimcr.org
Copyright : © Toufaili ZH (2022).
Abstract
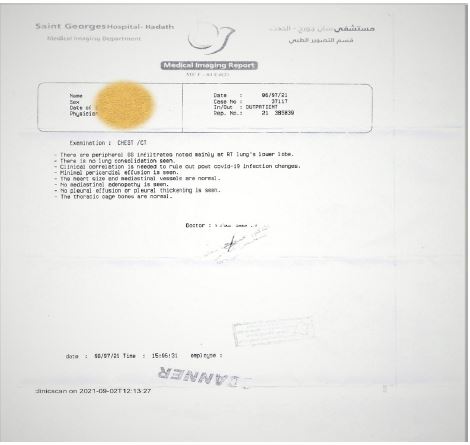
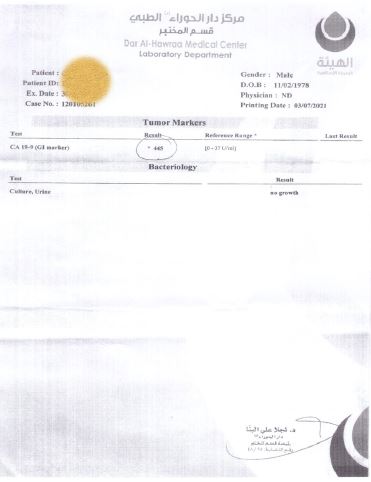
Around 40-year old male with previously controlled diabetes mellitus type II, presented for right upper quadrant abdominal pain. Workup showed elevation in HbA1c 15% and CA 19-9 of 445 U/ml (reference range < 37). CT abdomen with IV contrast was negative for pancreatic tumor. CT chest showed peripheral ground glass infiltrates noted mainly at the right lung’s lower base. Patient took treatment for community acquired pneumonia.
Four months later his HbA1c dropped back to 7.4% and CA 19-9 was at a normal range. He continued his same old medical treatment and was doing well on it.
This case suggests that physicians should avoid requesting CA 19-9 initially in the investigation for loss of glycemic control to avoid fear of cancer and unnecessary follow-up studies especially that uncontrolled diabetes is multifactorial and is aggravated by the presence of infections that can show atypical presentations in such patients.
Keywords: Diabetes mellitus type 2; General practice / family medicine; Pneumonia; Pancreatic cancer; Screening (oncology).
Citation: Toufaili ZH. Elevated serum Carbohydrate Antigen (CA) 19-9 level in a patient with uncontrolled diabetes mellitus. J Clin Images Med Case Rep. 2022; 3(8): 2018.
Introduction
Primary health care workers encounter a variety of medical conditions including acute illnesses while taking care of patients with chronic diseases.
We present a case of previously controlled diabetes mellitus with sudden elevation of HbA1c and abdominal pain that raised the suspicion of a possible pancreatic cancer.
CA 19-9 is a useful marker for gastrointestinal cancers especially biliary tract and pancreatic cancers. However, it may also increase in benign pancreatobiliary, hepatic and pulmonary diseases, thyroiditis, diabetes mellitus, and autoimmune diseases [1,2]. The American Society of Clinical Oncology (ASCO) claimed the specificity and sensitivity of CA 19-9 alone is inadequate for a reliable diagnosis in pancreatic cancer [3,4]. Therefore, precise history taking and physical examination should be performed along with step-wise approach to laboratory investigation is advised before testing for tumor markers.
In particular, CA 19-9 elevation in diabetic patients may lead to more fear of pancreas cancer as several previous epidemiological studies have shown that diabetic patients are susceptible to pancreatic cancer [2,5-7].
Case presentation
A male patient in his early forties known to have well controlled diabetes mellitus presented to a private polyclinic in Lebanon for renewal of his chronic medications. He recently checked his HbA1c level which turned out to be 15%, he also reported polyuria and polydipsia as well as abdominal pain. The pain was described as dull and disturbing in nature, he had good appetite but felt tired.
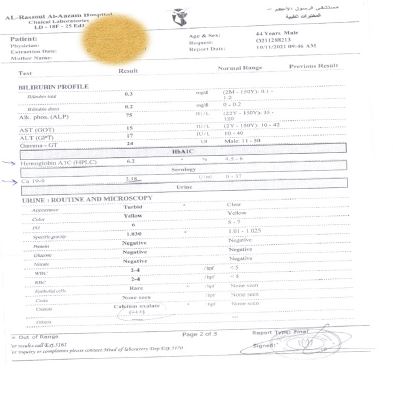
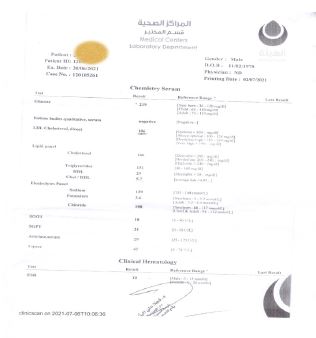
Laboratory workup done showed no electrolyte disturbances and no ketones were detected in serum or in urine. He had serum WBC count of 9.63/ ul with 46.7 % neutrophils and 36.4% lymphocytes, normal TSH level, liver function test, but high CA 19-9 reaching 445 (normal reference range 0-37 U/ml). Malignancy was suspected and CT scan of chest, abdomen and pelvis was done with IV contrast.
Results came back negative for pancreatic tumor, with normal liver size and density and no intra or extra- hepatic ducts dilatation. However peripheral ground glass infiltrates were noted mainly at the right lung’s lower lobe.
The patient was then treated for community acquired pneumonia and was doing well after that.
Follow up visit was scheduled in four months. Repeat of labs showed HbA1c of 6.2% and Ca 19-9 of 2.18 (Table 1).
The patient was reassured and educated to continue his same old medical treatment.
Table 1: Comparison between laboratory values at time of presentation and after treatment.
| Blood test normal range | June 2021 | Nov 2021 |
|---|---|---|
| HbA1c (4.5-6%) | 15 | 6.2 |
| Ca 19-9 (0-37 U/ml) | 445 | 2.18 |
| WBC (4-11 k/ul) | 9.63 | 11.6 |
| Neutrophil (37-75%) | 46.7 | 58.4 |
| Lymphocytes (10-50%) | 36.4 | 26.3 |
| ALT (10-40 IU/L) | 31 | 17 |
Discussion
CA 19-9 is a tumor-associated antigen that was first described in the early 1980s. It has been the most widely used tumor marker in pancreatic cancer [8,9].
For a tumor marker to be ideal, it has to be specific to a given tumor type and highly sensitive to avoid false positive diagnosis [10,11]. However, this does not apply to CA 19-9 due to its inadequate sensitivity [12,13] and false negative results in the Lewis blood type negative population [4,14].
CA 19-9 is synthesized in the normal pancreatic parenchyma and biliary tract. It is also produced from the epithelial cells of the gastric, colonic, and uterine mucosa, as well as the salivary glands [2].
The major limitation for using CA 19-9 as a tumor marker for pancreatic cancer is that it may be markedly elevated in patients with other malignancies such as colorectal, liver, breast, and lung cancers, as well as nonmalignant diseases such as obstructive jaundice, pancreatitis, cirrhosis, and lung disorders [12,13,15-18].
Yokoyama et al [19] confirmed elevated levels of CA 19-9 in bronchial epithelium-derived serum and bronchoalveolar lavage fluid by immune histochemical analysis. CA 19-9 is selectively expressed in regenerating epithelial cells in patients with idiopathic interstitial pneumonia and Diffuse Pan-Bronchiolitis (DPB), regardless of the etiology [20].
Also most of the bronchial mucus obtained during general anesthesia from patients without pulmonary diseases contains high levels of CA 19-9 [21]. Meaning that even destruction of normal lung tissue could lead to elevation in serum CA 19-9 levels [20].
In a retrospective review of medical reports of 192 patients who had elevation in CA 19-9 in the absence of malignancy done by Kim et al [2]. The estimated causes were found in 147 patients (76.6%) and were classified as hepatic in origin in 63 patients (42.8%), pulmonary in 32 (21.7%), gynecologic in 38 (25.8%), endocrine in 13 (8.8%), and related to spleen disease in 1.
It was also noticed that in chronic lung disease, the CA 19-9 level remained consistently elevated with a slight increase or decrease, but never normalized.However, in acute pulmonary diseases such as pneumonia or lung abscess, the CA 19-9 level normalized or decreased after treatment.
Also, It has already been shown that CA 19-9 and HbA1c values are mutually correlated with each other and that CA 19-9 increases in proportion to blood sugar levels [9,22].
The reason for CA 19-9 elevation in benign diseases was explained by several mechanisms. First of all, inflammation and proliferation of non-tumorous tissue such as in pancreatitis, cholangitis, bronchiectasis, idiopathic pulmonary fibrosis, ovarian cyst, and endometriosis, can elevate CA 19-9. Second, blockage of CA 19-9 excretion in certain diseases as obstructive jaundice and bronchitis may lead to elevation in its serum level. Finally, when metabolic malfunction is present such as in hepatitis, diabetes mellitus, and chronic glomerulonephritis, elevation in serum CA19-9 may occur [2,23].
Our patient was found to have elevation in HbA1c and infiltrates on CT chest, which suggests based on the data above and the negative abdominal CT scan for pancreatic tumor that the reason for elevated CA19-9 was either the acute lung inflammation or the metabolic malfunction in the context of uncontrolled diabetes mellitus which may even be the result of the infection itself or all factors combined together. The return of CA 19-9 back to normal three months after successful treatment of pneumonia and adequate control of diabetes mellitus was reassuring and confirmed the speculated cause.
Several previous epidemiological studies have shown that diabetic patients are susceptible to pancreatic cancer [5-7]. Therefore CA 19-9 elevation in diabetic patients should be carefully analyzed [2,24].
We suggest that careful history taking and physical examination should be performed before running into laboratory workup. And in the presence of an infection, physicians should refrain from ordering CA 19-9 as elevated levels may be found in the absence of malignancies as discussed above. In particular, CA 19-9 elevation in diabetic patients may lead to more fear of pancreatic cancer and the need to go through unnecessary investigation with all its psychological and financial burden to the patient.
In our case, after obtaining a negative CT scan of the abdomen, we could not be reassured as the CA19-9 level was very high so the patient was offered the choice to do gastroscopies for further investigation which he opted to postpone especially that he started to feel better after the antibiotic course. Follow up labs, four months later, were all back to normal and the patient was finally reassured.
An algorithm of systematic approach to CA19-9 elevation without evidence of malignancy was suggested by Kim et al [2]. They recommended for diabetic patients with CA 19-9 elevation, an imaging study should be performed to rule out pancreatic cancer. If no abnormality is observed on imaging, then HbA1c should be checked first because uncontrolled diabetes mellitus may be the cause. If the HbA1c is elevated, the blood glucose should be strictly controlled with follow-up measurements of CA19-9 and HbA1c together. If CA 19-9 decreases after intensive blood sugar control, then CA 19-9 elevation was due to hyperglycemia [2,25].
The diagnosis can be confirmed clearly if changes in CA 19-9 match the course of the suspected benign disease during a follow-up period of 1-3 months. If CA 19-9 is normalized after treatment of the causative disease, additional follow-up is not necessary.
We find the mentioned approach reasonable given all the known data on CA 19-9, in addition physicians should be careful on when to check this tumor marker especially in the context of hyperglycemia and infection.
Take home messages
• Sudden loss of glycemic control is multifactorial, infection is one of the most common causing factors.
• CA 19-9 is a tumor marker that may be elevated in benign conditions.
• Physicians should refrain from requesting CA 19-9 level in the context of hyperglycemia and infection until control of the acute illness.
• In particular, in patients with diabetes mellitus, elevated CA 19-9 level lead to more fear of pancreatic cancer.
• Careful history taking and physical examination along with stepwise approach to laboratory investigations is recommended to avoid psychological and financial stress on the patient.
Declarations
Acknowledgements: Special thanks to Mr. J K for his trust and consent to share his medical hardship.
Conflicts of interests: The author declares having no competing interests.
References
- Ventrucci M, Pozzato P, Cipolla A, Uomo G. Persistent elevation of serum CA 19-9 with no evidence of malignant disease. Dig Liver Dis. 2009; 41: 357–363.
- Kim S, Park BK, Seo JH, Choi J, Choi JW, et al. Carbohydrate antigen 19-9 elevation without evidence of malignant or pancreatobiliary diseases. Sci Rep. 2020; 10: 1–9.
- Locker GY, Hamilton S, Harris J, Jessup JM, Kemeny N, et al. ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol. 2006; 24: 5313–5327.
- Wu E, Zhou S, Bhat K, Ma Q. CA 19-9 and pancreatic cancer. Clin Adv Hematol Oncol. 2013; 11: 53–55.
- Maisonneuve P, Lowenfels AB. Risk factors for pancreatic cancer: A summary review of meta-analytical studies. Int J Epidemiol. 2015; 44: 186–198.
- Batabyal P, Vander Hoorn S, Christophi C, Nikfarjam M. AssociaAssociation of diabetes mellitus and pancreatic adenocarcinoma: A meta-analysis of 88 studies. Ann Surg Oncol. 2014; 21: 2453–2462.
- Li D, Tang H, Hassan MM, Holly EA, Bracci PM, et al. Diabetes and risk of pancreatic cancer: A pooled analysis of three large case-control studies. Cancer Causes Control. 2011; 22: 189–197.
- Koprowski H, Steplewski Z, Mitchell K, Herlyn M, Herlyn D, et al. Colorectal carcinoma antigens detected by hybridoma antibodies. Somatic Cell Genet. 1979; 5: 957–971.
- Uygur Bayramiçli O, Debak R, Orbay E, Dolapçioǧlu C, Sargin M, et al. Type 2 diabetes mellitus and CA 19-9 levels. World J Gastroenterol. 2007; 13: 5357–5359.
- Pepe MS, Etzioni R, Feng Z, Potter JD, Thompson M Lou, et al. Phases of biomarker development for early detection of cancer. J Natl Cancer Inst. 2001; 93: 1054–1061.
- Feng Z. Classification versus association models: Should the same methods apply? Scand J Clin Lab Invest. 2010; 70: 53–58.
- Duffy MJ, Sturgeon C, Lamerz R, Haglund C, Holubec VL, et al. Tumor markers in pancreatic cancer: A European Group on Tumor Markers (EGTM) status report. Ann Oncol [Internet]. 2009; 21: 441–447. Available from: https://doi.org/10.1093/annonc/mdp332
- Goonetilleke KS, Siriwardena AK. Systematic review of carbohydrate antigen (CA 19-9) as a biochemical marker in the diagnosis of pancreatic cancer. Eur J Surg Oncol. 2007; 33: 266–270.
- Kannagi R. Carbohydrate antigen sialyl Lewis a - Its pathophysiological significance and induction mechanism in cancer progression. Chang Gung Med J. 2007; 30: 189–209.
- Ritts RE, del Villano BC, Go VLW, Herberman RB, Klug TL, et al. Initial clinical evaluation of an immunoradiometric assay for CA 19‐9 using the nci serum bank. Int J Cancer. 1984; 33: 339–345.
- Frebourg T, Bercoff E, Manchon N, Senant J, Basuyau JP, et al. The evaluation of CA 19‐9 antigen level in the early detection of pancreatic cancer: A prospective study of 866 patients. Cancer. 1988; 62: 2287–2290.
- Pavai S, Yap SF. The Clinical Significance of Elevated Levels of Serum CA 19-9. Med J Malaysia. 2003; 58: 667–672.
- Duffy MJ. CA 19-9 as a marker for gastrointestinal cancers: A review. Ann Clin Biochem. 1998; 35: 364–370.
- Yokoyama T, Ikedou Y, Kido F, Tanoue S, Tashiro K, et al. A study of sialylated carbohydrate antigen in patients with benign bronchopulmonary disease. Nihon Kokyuki Gakkai Zasshi. 1998; 36: 851-856.
- Shin JY, Yoo SJ, Park BM, Jung SS, Kim JO, et al. Extremely increased serum carbohydrate antigen 19-9 levels caused by new or resistant infections to previous antibiotics in chronic lung diseases. Tuberc Respir Dis (Seoul). 2013; 75: 125–127.
- Matsuoka Y, Endo K, Kawamura Y, Yochida T, Saga T, et al. Normal Bronchial Mucus Contains High Levels of Cancer-Associated Antigens, CA 125, CA 19-9, and Carcinoembryonic Antigen. Cancer. 1990; 651: 506–510.
- Kim SH, Baek CO, Lee KA, Park TS, Baek HS, et al. Clinical implication of elevated CA 19-9 level and the relationship with glucose control state in patients with type 2 diabetes. Endocrine. 2014; 46: 249–255.
- Ito S, Gejyo F. Elevation of Serum CA19-9 Levels in Benign Diseases. Intern Med. 1999; 38: 840–841.
- Liao WC, Tu YK, Wu MS, Lin JT, Wang HP, et al. Blood glucose concentration and risk of pancreatic cancer: Systematic review and dose-response meta-analysis. BMJ [Internet]. 2015; 349: 1–11. Available from: http://dx.doi.org/doi:10.1136/bmj.g7371
- Murai J, Soga S, Saito H, Otsuki M, Kitada T, et al. Study on the mechanism causing elevation of serum CA19-9 levels in diabetic patients. Endocr J. 2013; 60: 885–891.