
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
IgG4-related lung disease: A case report and literature review
Hongmei Ren1*; Zhiqing Han1; Jinping Wang1; Siming Meng1; Xiaoming Zuo2; Cuixia Zheng1
1Department of Respiratory Critical Medicine, Yangpu Hospital of Tongji University, 450 Tengyue Rd., Shanghai, 200090 China.
2Department of Pathology, Yangpu Hospital of Tongji University, China.
*Corresponding Author : Hongmei Ren
Department of Cardiology, Daping Hospital, Army Medical University, Chongqing, China.
Email: rhm321@163.com.
Received : Aug 01, 2022
Accepted : Aug 22, 2022
Published : Aug 29, 2022
Archived : www.jcimcr.org
Copyright : © Ren H (2022).
Abstract
IgG4-Related Lung Disease (IgG4-RLD) is an unusual disease, having various clinical manifestations. Patients may have no respiratory symptoms and no abnormalities shown on chest images. Therefore, the diagnosis is challenging. Here we present an uncommon case of IgG4-RLD with multi-loci nodeson the center of the hilar and review the relevant literature.
Keywords: IgG4-related diseases; Lung.
Abbreviations: Abbreviations: CT: Computed Tomography; HPF: High Power Field; Igg4-RD: Igg4-Related disease; Igg4-RLD: Igg4-Related Lung Disease; AIP: Autoimmune Pancreas.
Citation: Ren H, Han Z, Wang J, Meng S, Zuo X, et al. IgG4-related lung disease: A case report and literature review. J Clin Images Med Case Rep. 2022; 3(8): 2019.
Introduction
Igg4-Related Disease (IgG4-RD) is a newly recognized autoimmune-mediated fibro inflammatory disease that may affect multiple organs and lead to tumefactive, tissue destructive lesions and organ failure. It is characterized by a dense lymphoplasmacytic infiltrate rich in IgG4-positive plasma cells, storiform fibrosis, and often but not always, elevated serum IgG4 concentrations [1,2]. Involvement of nearly every anatomic site has been reported. The most commonly involved organs are pancreas, bile duct, main salivary gland (submandibular gland and parotid gland), lacrimal gland, retroperitoneal and lymph node [3,4]. Immunoglobulin G4 related disease was first reported in the late 1990s. Yoshida K et al [5] reported that a large number of IgG4 positive plasma cells infiltrated in a patient with Autoimmune Pancreas (AIP). In 2003, it was reported for the first time that a large number of IgG4-positive plasma cells infiltrated in the lung lesions of AIP patients. It is suggested that AIP is a new autoimmune disease related to IgG4 with multiple system involvement, which may lead to lung involvement. In 2009, Zen et al [6] called IgG4-RD involved in lung “IgG4-related lung disease (IgG4-RLD)”. Due to the late recognition of IgG4-RLD and lack of clinical experience, it is easy to cause misdiagnosis and mistreatment. Here we report a pathologically confirmed case of IgG4-RLD with multi-loci nodes were centered on the hilar, and review the relevant literature to improve the cognition of the disease.
Case presentation
This is a 71-year-old male patient with chest pain and shortness of breath. He coughed for one month, with aggravated symptom for one week. One month before his admission, the patient fell down and complained chest pain, shortness of breath, as well as cough with a small amount of white phlegm. The chest pain was paroxysmal dull pain in the lower chest, which was heavier on the right side than on the left side, and had no correlation with the change of breath and posture. With progressive decrease of poor appetite and fatigue, he came to the respiratory clinic of our hospital. The plain scan of CT showed that there was multi-loci nodes on the upper right lobe and middle right lobe, the upper left lobe, and the lower left lobe. These shadows were centered on the hilar, with unclear boundary. Local bronchial lumen stenosis, miliary nodular shadows in both lungs, and enlarged hilar were also observed (Figure 1). He had a history of lacunar cerebral infarction for 10 months, and he took long-term aspirin orally. His respiratory rate was 22 breaths/min, and he suffered slightly short of breath. Besides, there was no positive signs in the lung, and no obvious abnormality in the rest. Auxiliary examination demon strated 72.61 mg/L of Serum CRP (C-Reactive Protein,115 g/L of Hb (Hemoglobin), 59 mm/1h of ESR (erythrocyte sedimentation rate), 31.9 g/L of serum albumin, 3.05 mmol/L of serum potassium, and 0.05N g/mL of serum procalcitonin. His urine and fecal routine, electrolytes of liver and kidney function, fungal D-glucan, thyroid function were normal. The blood tumor markers, including carcinoembryonic antigen, sugar antigen CAl9-9, squamous cell carcinoma antigen, neuron specific enolase and cytokeratin-19-fragment, were normal. His antinuclear antibody and Antineutrophil Cytoplasmic Antibody (ANCA) were negative, and his creatine kinase was normal. Rheumatoid factor was 110 IU/ml (reference value < 15 IU/ml); Immunoglobulin G was 14.3 g/L (reference value 7-16 g/L); Immunoglobulin G4 was 3.4 g/L (reference value 0.03-2.01 g/L); Immunoglobulin A was 2.13 g/L (reference value 0.7-4 g/L); Immunoglobulin M was 1.05 g/l (reference value 0.4-2.3 g/L). Total complement was 55.0 u/ml (reference value 23-46 U/ml). Arterial blood gas analysis showed: 7.45 of pH value, 5.18 kpa of PaCO2 and 9.2 kpa of PaO2 (without oxygen inhalation). No obvious abnormality was found in the enhanced CT scan of the upper abdomen. Further electron (fluorescence) bronchoscopy showed that the bronchial mucosa of the upper left lobe, the upper right lobe, the middle right lobe and the lower left lobe were hypertrophic. The lumen was narrow, and the apical of the upper right lobe was occluded (Figure 2). Pathological examination of the bronchial mucosa on the apical segment of the upper right lobe showed chronic inflammation of the mucosa. The biopsy of the right upper lung was performed. The histopathology showed nodular and stori form fibrosis, hyperplasia in the interstitial tissue of the lung. Also, a dense lymphoplasmacytic infiltration was observed. The number of IgG4- positive plasma cells was more than 10 per HPF (Figure 3). According to the diagnostic criteria of IgG4-related respiratory system involvement proposed by the Japanese Respiratory Society in the 54th IgG4-RLD Symposium in 2014 [7], the diagnosis of IgG4-RLD was clear. 30 mg of Prednisone was given per day orally, and the symptoms improved. Then, he was discharged from the hospital. After one month, the dosage was 25 mg QD orally. After 2 months of reexamination, the case’s symptoms were relieved. The reexamination of chest CT showed that the multi-loci nodes of the lung was obviously absorbed compared with that before (Figure 4). The IgG4 level in serum was 1.93 g/L, which was reduced to normal. At present, the condition is stable and the follow-up treatment is continuing.



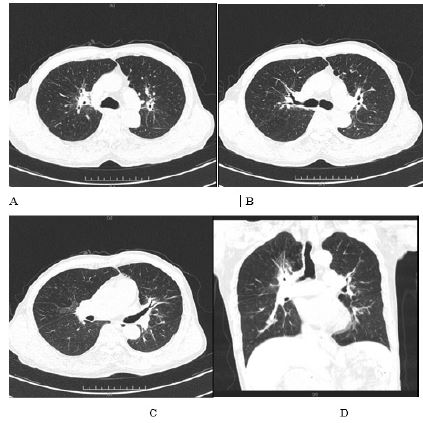
Table 1: General Clinical Data of IgG4-RLD Reviewed.
| Researcher | Number of cases | Average age (years) | Gender (male/female) | Number of Cases with Respiratory symptoms |
|---|---|---|---|---|
| Yoh Zen et al [6] 2009 | 21 | 69 | 17 /4 | 10, where: Cough (10) Hemoptysis (10) |
| Shoko Matsui et al [8] 2013 | 18 | 62 | 14/4 | 5 |
| Xuefeng sun et al [9] 2016 | 17 | 44.8 | 6/11 | Cough (11) dyspnea (5) chest pain (4) |
| Dai Inoue et al [10] 2012 | 13 | 62 | 9/4 | 10, where: Cough (7) hemoptysis (2) exertional dyspnea (2) chest pain (1) |
| Ming Wu et al [11] 2018 | 13 | 51.1 | 8/5 | 10, where Cough (9) expectoration (6) hemoptysis (6) chest distress (2) asthma (2) |
| Guojing Han et al [12] 2017 | 8 | 59 | 4/4 | 2, where Shortness of breath (2), cough (2), expectoration (2) after exercise |
| Xiaoting LV et al. [13] 2018 | 7 | 56 | 4/3 | 6, where: Dyspnea (6) cough (2) |
| Yan Li et al [14] 2018 | 6 | 55 | 5/1 | 6, where: Cough(5) expectoration (4) asthma (3) shortness of breath after activity (1) chest pain (1) chest distress (1) hemoptysis (1) |
| Joseph C K et al [15] 2016 | 6 | 55.2 | 5/1 | 4, where Cough (2) hemoptysis (1) dyspnea (1) |
| HuiZhang et al [16] 2012 | 4 | 47.8 | 1/3 | 4, where: Dry cough (3)shortness of breath (3) chest tightness (1) |
| Phillip Hui et al [17] 2013 | 3 | 52 | 1/2 | 3, where: Cough (3) dyspnea (2) expectoration (2) |
| Erik baltaxe et al [18] 2016 | 3 | 41 | 2/1 | 2, where: Cough (1) dyspnea (1) expectoration (1) pleural pain (1) |
| Kyoko Y et al [19] 2008 | 3 | 72 | 3/0 | Exertive dyspnea (2) |
| Xuefeng S, Min P et al [20] 2014 | 3 | 42.5 | 1/2 | 3 example Cough (3) expectoration (1) intermittent hemoptysis (1) chest pain (1) |
| Mingxia Ren et al [21] 2019 | 2 | 67 | 2/0 | Cough and expectoration (1) |
| Masahiro K et al [22] 2015 | 2 | 61.5 | 1/1 | Phlegm Blood (1) |
| Xinghua Shan et al [23] 2015 | 2 | 45.5 | 2/0 | Cough (2) expectoration(2) Phlegm Blood(1) chest pain (1)chest distress (1) |
| Case report [24-81] | 58 | 60 | 44/15 | 45, where:Cough(21)expectoration(9) dyspnea (7) dry cough (7)laborious dyspnea (6) shortness of breath after activity(5) Phlegm Blood(4) hemoptysis (2) asthma (2)chest pain(3) back pain (1) |
Discussion
IgG4-RLD is a rare disease. We searched Pub Med, CNKI and Wanfang database with the options of All Field “IgG4 related disease” AND All Field “lung”, AND All Field “IgG4 related disease” AND All Field “respiratory”. From 1990 to May 2020, 75 complete lgG4-related respiratory disease literatures, with 56 in English and 19 in Chinese, were retrieved. All of these papers were confirmed by histopathology, with 189 cases in total. Most of them were case reports, 17 of which involved more than 2 cases, including 1 that involved 21 cases (Table 1).
75 papers reviewed in this study were published from 2007 to 2020. The authors of the papers include researchers from China, Japan, the United States, South Korea, the United Kingdom, Germany, Italy, Australia, Greece, Argentina and other countries. Most of the papers published are from Japan, whose scientists contributed 25 papers. However, still the prevalence and incidence rate of IgG4-RD is not clear. According to Japanese scholars, the incidence of this disease throughout Japan is 0.28–1.08/100,000 [82]. 14% - 35% of patients with IgG4-RD will have intrathoracic invasion [83], [84]. IgG4-RD is mainly found in adults, most of them are men. Of the 189 cases, 133 were male and 56 were female, aged 23-79 years old, with an average age of 55.7 years old (Table 1).
The clinical manifestations of IgG4-RLD were various. The literature review of this study shows that among 126 of 189 patients with respiratory symptoms, such as cough, expectoration, dyspnea, chest pain, hemoptysis, shortness of breath after activity, etc., 24 patients were initially showing extrapulmonary symptoms, and 13 patients with asymptomatic physical examination were confirmed by chest imaging and pathology that the lung was involved (Table 1). In terms of clinical manifestations, these symptoms lack specificity, and were difficult to distinguish from other respiratory diseases. Besides, they were prone to misdiagnosis and missed diagnosis.
The increase of lgG4 concentration in serum is an important feature of laboratory examination. Nevertheless, the increase of serum IgG4 level is not specific. It can be seen in 5% of normal people, or in 10% patients with malignant tumors of the biliopancreatic system or other infectious diseases and inflammatory diseases [85]. The sensitivity and specificity of the diagnosis of IgG4-RD through serum lgG4 level were 63% and 94% respectively [86,87]. 3-30% of patients had normal serum IgG4 level [88].
The chest imaging manifestations of IgG4-RLD are various. More than half of the cases reviewed in the study literature showed nodular /mass shadow in 105 cases (55.5%). And In this study, we found that enlargement of hilar/mediastinal lymph nodes, infiltration shadow of lung, interstitial change of alveoli, thickening of bronchial wall /vascular bundle, thickening of interlobular septum, and thickening and/or infiltration of pleura can all appear in this disease. In the cases reviewed in this study, 5 cases of chest imaging showed cavities, 2 cases showed cystic lesions, and 1 indicated emphysema. The imaging manifestations can exist alone or in combination with several types. The above situation shows that although the image manifestations of IgG4-RLD have certain characteristics, it lacks obvious specificity. Nodular shadow and mass shadow should be differentiated from lung cancer. Interstitial change of alveoli, enlargement of hilar/mediastinal lymph nodes, and thickening of bronchial wall/vascular bundle should be differentiated from diffuse lung diseases such as lymphoproliferative diseases, sarcoidosis and nonspecific interstitial pneumonia.
Histopathological examination is the key to the diagnosis of the disease, and tissue biopsy is very important to exclude malignant diseases [88], tuberculosis, interstitial pneumonia, organic pneumonia, Castleman disease and other diseases. 189 patients had definite histopathology. The pathological specimens of 161 cases were obtained by pulmonary resection, VATS, lung biopsy, percutaneous lung biopsy and bronchoscopy lung/mucosa biopsy. Two cases were diagnosed by pleural biopsy and 19 cases by extrapulmonary organ biopsy. Although there was no lung tissue biopsy data, the lung images decreased or even disappeared following treatment, so IgG4-RLD was confirmed. Histopathological features: In 184 biopsies, lymphocytic plasmacytosis was seen, and in 132 biopsies, IgG4 positive plasmacytosis was found 10-159 (number/ HP). IgG4/IgG plasma cell value in 156 tissues was between 23% and 88%. There were obliterative phlebitis in 49 tissues, obliterative arteritis in 23 tissues, storiformfibrosis in 82 tissues and irregular fibrosis in 38 tissues. In addition, a small number of IgG4 positive cells can also be seen in many inflammatory infiltrates. Therefore, in absolute quantity, the number of IgG4 positive plasma cells determined in the literature is between 10-50/HPF. In relative quantity, if the ratio of IgG4 positive plasma cells to IgG plasma cells is greater than 50%, it is more helpful to diagnose IgG4-RD. Particularly, in the late stage of the disease, when only a small amount of plasma cells exist in the tissue and fibrosis becomes the main component, the ratio of IgG4 to IgG will play a key role in the diagnosis [89].
IgG4-RLD has a good response to glucocorticoid therapy. More than 50% of 189 patients reviewed in this study were treated with glucocorticoid alone, with an effective rate of 87.6%. Commonly used glucocorticoids include prednisone, prednisolone or methylprednisolone, with an initial dosage of 0.5-1 mg /kg/day for prednisone, 0.5-0.6 mg/kg/day for prednisolone or 0.4-80 mg/kg/day for methylprednisolone. 9.3% of patients recurred after glucocorticoid reduction, and the symptoms improved after glucocorticoid addition or combined with immunosuppressive agent. The immunosuppressive agents used in the review of this study include methotrexate, mycophenolatemofetil, azathioprine, cyclophosphamide and cyclosporine. The effective rate of operation was 56%. 14 cases were untreated, and 2 cases were self-healing (self-healing rate was 14.3%), which indicated that the disease had some self-healing. In particular, a case of inhaled fluticasone propionate (500 μ g) with salmeterol (50 μ g) was treated twice a day was effective. Two cases of glucocorticoid combined with rituximab were reported in the literature review. They were effective, but the disease was easy to relapse. When drugs were reduced, the disdisease was easy to recur. At present, the optimal maintenance dose and time of IgG4-RLD have not been determined. After the treatment, the patients who stop the drug and relapse can be treated with glucocorticoid again. Immunosuppressive agent should be used in the period of maintaining remission. The prognosis of this disease is not clear. In 189 patients reviewed in this study, only 3 died, and 1 died after VATS.
In summary, IgG4-RLD is a rare respiratory disease. It has non-typical clinical manifestations and various chest images. The disease can exist alone, and is often associated with other systemic diseases. Plus, it is difficult to distinguish it from common respiratory diseases such as lung cancer, tuberculosis, etc. The diagnosis of the disease depends on clinical, chest images, serum IgG4 level and comprehensive pathological analysis. It has a good response to glucocorticoid treatment. Some cases are prone to recur in the process of hormone reduction, so it should be followed up for a long time after treatment. The prognosis is not clear. Therefore, further prospective and multicentric clinical studies are needed.
Conclusion
Our case implied three clinical evidences: First, multi-loci nodes on the middle of the hilar could be the presentation of IgG4-related respiratory disease. Second, IgG4-related respiratory disease with hypertrophic mucosa. Finally, IgG4-related respiratory disease can be very sensitive to prednisone. Lung lesions were absorbed further, and serium concentration of IgG4 was decreased after prednisone treatment and symptoms significantly improved in our case. In brief, we reported the first case of IgG4-RLD presenting with multi-loci nodes were centered on the hilar combined with hypertrophic mucosa, the lumen was narrow and even occluded. The findings will further our understanding of the characteristics of IgG4-RLD.
Declarations
Ethics approval and consent to participate: Our study has received approval from the ethics committee of Yangpu Hospital of Tongji University.
Consent for publication: Written informed consent for publication of clinical details and/or clinicalimages was obtained from the patient. A copy of the consent form is available for review by the editor of this paper.
Availability of data and materials: The datasets related to this article are available from the corresponding author on reasonable request.
Competing interests: The authors claimed that they had no competing interests.
Funding: Not applicable.
Authors’ contributions: HR contributed to the conception and design, all data collection, and analysis and interpretation of data and played a major role in the writing of the article.
ZH, JW and SM provided raw data of the patient.
XZ gave suggestions on documenting the pathological findings in this report, and CZ made key revision on the manuscript for important intellectual content.
All authors have read and given consent to the final manuscript, and have ensured the integrity of their respective intellectual parts.
Acknowledgements: Not applicable.
References
- Stone JH, Zen Y, Deshpande V. IgG4-related disease [J]. N. Engl. J. Med. 2012; 366: 539-551.
- Khosroshahi A, Wallace ZS, Crowe JL, et al. International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease [J]. Arthritis Rheumatol. 2015; 67: 1688-1699.
- Kamisawa T, Funata N, Hayashi Y, et al. A new clinicopathological entity of IgG4-related autoimmune disease [J]. J Gastroenterol. 2003; 38: 982-984.
- Cheuk W, Chan JK. IgG4-related sclerosing disease: A critical appraisal of an evolving clinicopathologic entity [J]. Adv. Anat. Pathol. 2010; 17: 303-332.
- Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K, et al. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis [J]. Dig Dis Sci. 1995; 40: 1561-1568.
- Zen Y, Inoue D, Kitao A, et al. IgG4-related lung and pleural disease: a clinicopathologic study of 21 cases [J]. Am J Surg Pathol. 2009; 33: 1886-1893.
- Matsui S, Yamamoto H, Minamoto S, Waseda Y, Mishima M, et al. Proposed diagnostic criteria for IgG4-related respiratory disease [J]. Respir Investig. 2016; 54: 130-132.
- Matsui S, Hebisawa A, Sakai F, et al. Immunoglobulin G4-related lung disease: clinicoradiological and pathological features [J]. Respirology. 2013; 18: 480-487.
- Sun X, Liu H, Feng R, et al. Biopsy-proven IgG4-related lung disease [J]. BMC Pulm Med. 2016; 16: 20.
- Inoue D, Zen Y, Abo H, et al. Immunoglobulin G4-related lung disease: CT findings with pathologic correlations [J]. Radiology. 2009; 251: 260-270.
- Wu Ming, Wang Lu, Ji Yuan, et al. Analysis of clinical features of IgG4-related lung disease [J]. Chinese Journal of Medicine, 2018; 098: 3442-3446.
- Han Guo Jing, Hu Hong, Mao Dan, Bai Xue, She Danyang, Zhao Shifeng, Wen Zailu, Gao Jie. Analysis of clinical features of eight cases of IgG4-related lung disease[J].Chinese Journal of Tuberculosis and Respiratory Medicine. 2017; 40: 193-198.
- Lv X, Gao F, Liu Q, et al. Clinical and pathological characteristics of IgG4-related interstitial lung disease [J]. ExpTher Med. 2018; 15: 1465-1473.
- Li Yan. 6 cases of IgG4-related lung disease and literature review[J]. Journal of Clinical Pulmonology. 2018; 23: 1881-1884.
- Keenan JC, Miller E, Jessurun J, Allen T, Kim HJ. IgG4-related lung disease: A case series of 6 patients and review of the literature [J]. Sarcoidosis Vasc Diffuse Lung Dis. 2016; 32: 360-367.
- Zhang Hui, Shi Juhong, Feng Rui’e, Tian Xinlun, Xu Zuojun, Xu Wenbing, Liu Hongrui, Liu Tonghua. Clinicopathological analysis of four cases of IgG4-related nonspecific interstitial pneumonia[J].Chinese Journal of Tuberculosis and Respiratory Medicine. 2012; 35: 747-751.
- Hui P, Mattman A, Wilcox PG, Wright JL, Sin DD. Immunoglobulin G4-related lung disease: A disease with many different faces [J]. Can Respir J. 2013; 20: 335-338.
- Baltaxe E, Shulimzon T, Lieberman S, Rozenman J, Perelman M, et al. IgG4-Related Lung Disease - Three Untreated Cases with a Benign Outcome [J]. Arch Bronconeumol. 2016; 52: e1-e3.
- Yamashita K, Haga H, Kobashi Y, Miyagawa-Hayashino A, Yoshizawa A, Manabe T. Lung involvement in IgG4-related lymphoplasmacytic vasculitis and interstitial fibrosis: Report of 3 cases and review of the literature [J]. Am J Surg Pathol. 2008; 32: 1620-1626.
- Sun X, Peng M, Hou X, Feng R, Xu Z, et al. Refractory IgG4-related lung disease with constitutional symptoms and severe inflammation [J]. Am J Respir Crit Care Med. 2014; 189: 374-375.
- Ren Mingxia, Huang Yan, Fang Yi, Liu Yi. Three cases of IgG4-related lung disease and literature review[J]. Chinese Community Physician. 2019; 35: 18-19.
- Kitada M, Matuda Y, Hayashi S, et al. IgG4-related lung disease showing high standardized uptake values on FDG-PET: Report of two cases [J]. J Cardiothorac Surg. 2013; 8: 160.
- Shan Xinghua, Nie Xiaomeng, Yong Xiao, Wang Ying, Chen Liang, He Miaoxia, Yao Xiaopeng, Li Qiang, Huang Yi. Two cases of IgG4-related lung disease and literature review[J].Chinese Journal of Internal Medicine. 2015; 54: 684-690.
- Idoyaga P, Fielli M, González A, Ferreyra Mufarregue LR, Fernández Casares M, Crevena G. Enfermedadpulmonarintersticialpor IgG4 [IgG4-related interstitial lung disease][J]. Medicina (B Aires). 2018; 78: 449-452.
- Patel M, Kumar B, Diep ML, Nandurkar D. IgG4 Related Lung Disease [J]. Can Respir J. 2016; 2016: 1409281.
- Li Yan, Huang Mei, Cai Hourong, Sun Qi, Miao Liyun, Meng Fanqing, Xiao Yonglong. A case of IgG4-related lung disease and review of literature[J].Journal of Clinical Pulmonology. 2016; 1: 20-24.
- Wibmer T, Kropf-Sanchen C, Rüdiger S, et al. Isolated IgG4-related interstitial lung disease: unusual histological and radiological features of a pathologically proven case [J]. Multidiscip Respir Med. 2013; 8: 22.
- Wang J, Zeng Y, Gu Y, Li S, et al. IgG4-related lung disease manifested as pneumonia in puerperium: A case report [J]. Int J Clin Exp Pathol. 2015; 8: 3312-3315.
- Ahn JH, Hong SI, Cho DH, Chae EJ, Song JS, et al. A Case of IgG4-Related Lung Disease Presenting as Interstitial Lung Disease [J]. Tuberc Respir Dis (Seoul). 2014; 77: 85-89.
- Choi JH, Sim JK, Oh JY, et al. A Case of IgG4-Related Disease Presenting as Massive Pleural Effusion and Thrombophlebitis [J]. Tuberc Respir Dis (Seoul). 2014; 76: 179-183.
- Choi IH, Jang SH, Lee S, Han J, Kim TS, et al. A Case Report of IgG4-Related Disease Clinically Mimicking Pleural Mesothelioma [J]. Tuberc Respir Dis (Seoul). 2014; 76: 42-45.
- Kang MK, Cho Y, Han M, et al. IgG4-Related Lung Disease without Elevation of Serum IgG4 Level: A Case Report [J]. Tuberc Respir Dis (Seoul). 2016; 79: 184-187.
- Bae K, Jung H, Jeon KN, Hyun Song D, Kim SH, et al. Coexistence of nontuberculous mycobacterium and IgG4-related disease in a solitary pulmonary nodule: A case report [J]. Medicine (Baltimore). 2019; 98: e18179.
- Wang Jinlin, Wang Lulin, Fang Ying, Zeng Yunxiang, Li Shiyue, Gu Yingying. A case of IgG4-related lung disease with simple lung involvement[J].Chinese Journal of Tuberculosis and Respiratory. 2014; 37: 709-711.
- Hazzard C, Wolf AS, Beasley MB, Flores RM. Benign imitation of malignancy: Avoiding resection in immunoglobulin g4-related lung disease [J]. Ann Thorac Surg. 2014; 98: 1465-1467.
- Schneider F, Veraldi KL, Levesque MC, Colby TV, S Yi E. IgG4-Related Lung Disease Associated with Usual Interstitial Pneumonia [J]. Open Rheumatol J. 2016; 10: 33-38.
- Jagpal A, Crowe DR, de Andrade JA, Del Pilar Acosta Lara M, Navarro-Millan I. More than meets the eye: IgG4-related disease presenting as isolated interstitial lung disease [J]. Rheumatology (Oxford). 2017; 56: 1630-1631.
- Rumalla K, Smith KA, Arnold PM. Immunoglobulin G4-related epidural inflammatory pseudotumor presenting with pulmonary complications and spinal cord compression: case report [J]. J Neurosurg Spine. 2017; 26: 688-693.
- Naramala S, Biswas S, Adapa S, et al. Pleomorphic Pulmonary Manifestations of IgG4-Related Disease [J]. Case Rep Rheumatol. 2019; 2019: 7572869.
- Xue J, Wang XM, Li Y, et al. Highlighting the importance of early diagnosis in progressive multi-organ involvement of IgG4-related disease: A case report and review of literature [J]. World J Clin Cases. 2018; 6: 707-715.
- Kobayashi H, Shimokawaji T, Kanoh S, Motoyoshi K, Aida S, et al. IgG4-positive pulmonary disease [J]. J Thorac Imaging. 2007; 22: 360-362.
- Tanabe N, Kato M, Yonemoto C, Koshimo Y, Goto S, et al. A Case of IgG4-related Inflammatory Pseudotumor of the Lung] [J]. Nihon Kokyuki Gakkai Zasshi. 2008; 46: 894-898.
- Takato H, Yasui M, Ichikawa Y, et al. Nonspecific interstitial pneumonia with abundant IgG4-positive cells infiltration, which was thought as pulmonary involvement of IgG4-related autoimmune disease [J]. Intern Med. 2008; 47: 291-294.
- Ikari J, Kojima M, Tomita K, et al. A case of IgG4-related lung disease associated with multicentricCastleman’s disease and lung cancer [J]. Intern Med. 2010; 49: 1287-1291.
- Fujiu K, Sakuma H, Miyamoto H, Yamaguchi B. Immunoglobulin G4-related inflammatory pseudotumor of the lung [J]. Gen Thorac Cardiovasc Surg. 2010; 58: 144-148.
- Toyoshima M, Chida K, Kono M, et al. IgG4-related lung disease in a worker occupationally exposed to asbestos [J]. Intern Med. 2010; 49: 1175-1178.
- Umeda M, Fujikawa K, Origuchi T, et al. A case of IgG4-related pulmonary disease with rapid improvement [J]. Mod Rheumatol. 2012; 22: 919-923.
- Tanaka K, Nagata K, Tomii K, Imai Y. A case of isolated IgG4-related interstitial pneumonia: a new consideration for the cause of idiopathic nonspecific interstitial pneumonia [J]. Chest. 2012; 142: 228-230.
- Sugino K, Gocho K, Ishida F, et al. Acquired hemophilia A associated with IgG4-related lung disease in a patient with autoimmune pancreatitis [J]. Intern Med. 2012; 51: 3151-3154.
- Inoue T, Hayama M, Kobayashi S, et al. Lung cancer complicated with IgG4-related disease of the lung [J]. Ann Thorac Cardiovasc Surg. 2014; 20: 474-477.
- Suzuki H, Watanabe M, Ara T, et al. Immunoglobulin G4-related lung disease accompanied by organizing pneumonia [J]. Intern Med. 2013; 52: 2105-2111.
- Jinnur PK, Yi ES, Ryu JH, Iyer VN. Cavitating Lung Disease: A Novel Presentation of IgG4-Related Disease [J]. Am J Case Rep. 2015; 16: 478-482.
- Noguchi S, Yatera K, Jinbo M, et al. IgG4-related Lung Disease Associated with Autoimmune Hemolytic Anemia: A Case Report and a Literature Review[J]. Intern Med. 2016; 55: 2469-2474.
- Tashiro H, Takahashi K, Nakamura T, Komiya K, Kimura S, et al. Coexistence of lung cancer and immunoglobulin G4-related lung disease in a nodule: a case report [J]. J Med Case Rep. 2016; 10: 113.
- Yamakawa H, Suido Y, Sadoyama S, et al. Desquamative Interstitial Pneumonia Complicated with IgG4-related Lung Disease [J]. Intern Med. 2017; 56: 1553-1556.
- Kotetsu Y, Ikegame S, Takebe-Akazawa K, Koga T, Okabayashi K, Takata S. A case of IgG4-related lung disease complicated by asymptomatic chronic Epstein-Barr virus infection [J]. ClinRespir J. 2017; 11: 1012-1017.
- Mikumo H, Hamada N, Harada E, et al. A case of immunoglobulin G4-related respiratory disease with multiple lung cysts: A case report [J]. Respir Med Case Rep. 2017; 21: 89-92.
- Okubo T, Oyamada Y, Kawada M, Kawarada Y, Kitashiro S, Okushiba S. Immunoglobulin G4-related disease presenting as a pulmonary nodule with an irregular margin [J]. Respirol Case Rep. 2016; 5: e00208.
- Kono M, Nakamura Y, Oyama Y, et al. IgG4-related disease presenting with combined pulmonary fibrosis and emphysema (CPFE) [J]. Respir Med Case Rep. 2018; 25: 257-260.
- Arakawa N, Yamasawa H, Takemura T, Okada S, Taki T, Ishikawa S. Interstitial pneumonia with autoimmune features that met the proposed diagnostic criteria for IgG4-related respiratory disease [J]. Respirol Case Rep. 2019; 8: e00512.
- Sakashita K, Takamori M, Murata K, Wada A, Fujita A, Enatsu K. [A Case of IgG4-positive Inflammatory Pseudotumor Which Rapidly Resolved] [J]. Nihon Kokyuki Gakkai Zasshi. 2011; 49: 172-177.
- Ono Y, Toyokawa G, Tagawa T, Ijichi K, Oda Y, et al. IgG4-Related Lung Disease Exhibiting the Invasion into the Diaphragm: A Case Report [published online ahead of print, 2020 Feb 27] [J]. Ann Thorac Cardiovasc Surg. 2020; 10.5761/atcs.cr.19-00244.
- Liu A, Zhang Q, Liu B, Xu N, Li A, et al. A case of immunoglobulin G4-related lung disease with bilateral diffuse infiltration: A case report [J]. Medicine (Baltimore). 2017; 96: e9211.
- Liu Yong, Sun Yongchang, Feng Rui’e, Liu Xiaofang, Liu Guangjie, Liu Honggang. A case of IgG4-related lung disease and literature review[J].Chinese Journal of Tuberculosis and Respiratory. 2012; 35: 752-757.
- Wang Shaoting, Sun Xuefeng. A case of IgG4-related disease confirmed by multiple sites of pathology[J]. Union Medical Journal. 2017; 8: 274-277.
- Skopouli FN, Panayotopoulos P, Moutsopoulos HM. IgG4-Related Nodular Lung Lesion [J]. Arthritis Rheumatol. 2017; 69: 438.
- Lococo F, Di Stefano T, Rapicetta C, et al. Thoracic Hyper-IgG4-Related Disease Mimicking Malignant Pleural Mesothelioma [J]. Lung. 2019; 197: 387-390.
- Lin Huan, Niu Chunlai, Dong Yuchao, Zhang Wei, He Miaoxia, Qin Hao, Zhou Dan. A case of IgG4-related lung disease complicated with squamous cell carcinoma and literature review[J].International Journal of Respiratory. 2019; 39: 1379-1384.
- Tan H, Li H, Hu Y, Niu R, Pan P, Hu C. A case of solely lung-involved IgG4-related disease mimicking tuberculosis [J]. Heart Lung. 2015; 44: 161-164.
- Zhang XQ, Chen GP, Wu SC, et al. Solely lung-involved IgG4-related disease: A case report and review of the literature [J].Sarcoidosis Vasc Diffuse Lung Dis. 2016; 33: 398-406.
- Chen CF, Chu KA, Tseng YC, Wu CC, Lai RS. IgG4-related lung disease presenting as interstitial lung disease with bronchiolitis: A case report [J]. Medicine (Baltimore). 2017; 96: e9140.
- Wang X, Wan J, Zhao L, Da J, Cao B, Zhai Z. IgG4-related disease with tracheobronchial miliary nodules and asthma: a case report and review of the literature [J]. BMC Pulm Med. 2019; 19: 191.
- Zhang Yu, Huang Shaoxiang, Xu Jianchun, Zhang Lidong. A case of IgG4-related disease with pulmonary involvement and literature review[J]. Chongqing Medicine. 2016; 45: 4604-4606.
- Xie Liangjun, Zhang Feng, Li Jianfang, Qin Luping, Zhang Tingjie, Cheng Muhua. Analysis of two cases of pulmonary cavity lesions with hypermetabolism on PET/CT[J]. New Medicine. 2017; 48: 666-668.
- Kang Guannan, Dang Ping, Hou Lili, Ma Qingyan, Song Tao, Geng Shujun. Analysis of the causes of misdiagnosis of IgG4-related pulmonary disease as pulmonary tuberculosis[J].Clinical misdiagnosis and mistreatment. 2017; 30: 40-42.
- Cai Xiaojia, Shi Gaofeng, Xu Qian, Liu Yao. A case of IgG4-related lung disease[J]. Journal of Practical Radiology. 2018; 34: 485-486.
- Gómez Hernández MT, Rodríguez Alvarado I, Novoa N, Jiménez López MF. Immunoglobulin G4-Related Lung Disease as an Incidental Finding After Surgical Resection of Lung Cancer [J]. Arch Bronconeumol. 2019; 55: 276-278.
- Qiu Chenhui, Ye Jian. A case of IgG4-related disease complicated with diffuse alveolar hemorrhage[J].Zhejiang Practical Medicine. 2019; 24: 383-385.
- Ji Qun, Fang Tuanyu, Quan Huibiao, Wang Fei. A case of type 2 diabetes mellitus complicated with IgG4-related lung disease[J].Chinese Journal of Diabetes. 2019; 27: 229-233.
- Hu Jingjing, Guan Caihong. A case of IgG4-related lung disease and literature review[J]. Zhejiang Journal of Integrated Traditional Chinese and Western Medicine. 2019; 29: 753-755.
- Wang Tingli, Gou Shenju, Qiu Hongyu. A case of membranous nephropathy combined with immunoglobulin G4-related lung disease and previous esophageal cancer [J]. West China Medicine. 2019.
- Uchida K, Masamune A, Shimosegawa T, Okazaki K. Prevalence of IgG4-Related Disease in Japan Based on Nationwide Survey in 2009 [J]. Int J Rheumatol. 2012; 2012: 358371.
- Fei Y, Shi J, Lin W, et al. Intrathoracic Involvements of Immunoglobulin G4-Related Sclerosing Disease[J]. Medicine (Baltimore). 2015; 94: e2150.
- Zen Y, Nakanuma Y. IgG4-related disease: A cross-sectional study of 114 cases [J]. Am J SurgPathol. 2010; 34: 1812-1819.
- Ebbo M, Grados A, Bernit E, et al. Pathologies Associated with Serum IgG4 Elevation [J]. Int J Rheumatol. 2012; 2012: 602809.
- Raj R. IgG4-related lung disease [J]. Am J Respir Crit Care Med. 2013; 188: 527-529.
- Hao M, Liu M, Fan G, Yang X, Li J. Diagnostic Value of Serum IgG4 for IgG4-Related Disease: A PRISMA-compliant Systematic Review and Meta-analysis [J]. Medicine (Baltimore). 2016; 95: e3785.
- Khosroshahi A, Wallace ZS, Crowe JL, et al. International Consensus Guidance Statement on the Management and Treatment of IgG4-Related Disease [J]. Arthritis Rheumatol. 2015; 67: 1688-1699.
- Cai Boqiang. Pulmonary manifestations of connective tissue disease[M]. Beijing, People’s Health Publishing House. 2014.