
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
An unusual presentation of a neuroblastoma
Francesco Pacchiano1; Paolo Pizzicato2*; Luisa Castelli2; Patrizia Lombardo2; Carmela Brillantino2; Pasquale Guerriero2; Maria Cristina Smaldone2; Antonio Rossi3; Rocco Minelli4; Giuseppe Paviglianiti5; Valentina Cariello1; Michele Capozza6; Massimo Eraldo Abate6; Eugenio Rossi2
1Seconda Universitàdeglistudidi Napoli Luigi Vanvitelli “Naples, Italy.
2U.O.S.D. Diagnostica per Immagini A.O.R.N. Santobono-Pausilipon, Pausilipon Hospital, Naples, Italy.
3Università Campus Biomedico Roma.
4Department Life and Health “V. Tiberio”, University of Molise, Francesco De Sanctisst 1,86100,Campobasso, Italy.
5UOC Radiologia Pediatrica ARNASCivico-Di Cristina-Benfratelli, Palermo.
6UOC Oncologia Pediatrica A.O.R.N. Santobono-Pausilipon, Pausilipon Hospital, Naples, Italy.
*Corresponding Author : Paolo Pizzicato
U.O.S.D. Diagnostica per Immagini A.O.R.N. Santobono-Pausilipon, Pausilipon Hospital, Naples Italy.
Email: paolopizzicato@gmail.com
Received : Aug 01, 2022
Accepted : Aug 23, 2022
Published : Aug 30, 2022
Archived : www.jcimcr.org
Copyright : © Pizzicato P (2022).
Abstract
Neuroblastoma (NB) and Wilms tumor (WT) are very common tumors of the pediatric patient and can be sometimes difficult to make a differential diagnosis based only on the imaging findings. We present the case of a little patient who presented to our department with an abdominal mass in the left abdominal region, where the lesion presented elements at imaging which led to the diagnosis of a WT in a context of negativity of the urinary catecholamines. The lesion was treated with chemotherapy, although given the lack of response of the mass, was then conducted a biopsy that led to the diagnosis of NB of the surrenal gland.
Keywords: Wilms Tumor (WT); Neuroblastoma (NB); SIOP.
Citation: Pacchiano F, Pizzicato P, Castelli L, Lombardo P, Brillantino C, et al. An unusual presentation of a neuroblastoma. J Clin Images Med Case Rep. 2022; 3(8): 2020.
Introduction
CNB is a malignant tumor that originates from neural crest cells, is the most common tumor in children under the age of 1 year [1]. Patients with localized disease are often asymptomatic or may present with abdominal distension and pain [2]. This type of tumors appears heterogeneous, not well delimited, which can extend beyond the midline [3], with calcifications in between 80% and 90% of cases [4].
Case report
A 3-year-old female patient presented to our emergency department with fever, abdominal distension and constipation. Physical examination identified a palpable mass in the left abdominal region. Routine laboratory tests revealed anemia was present: (RBC = 3.76 106 / μl, Hb = 8.30 g/dl; MCV= 71.00 fl (vn: 75.00-95.00)); LDH= 1660 U/L, PCR= 19.41 mg/L, Iron 27 μg/dl (vn: 30-120), ESR = 65 mm (vn: 1-15). Homovanillic Acid (HVA), Vanillylmandelic Acid (VMA) and 5-OHindolacetic acid were within normal limits negative [23.2 mg/L (nv 0.00-22.00); 6.5 mg/L (nv 0.00-11.00) and 8.8 mg /L (nv: 1.2-16.2), respectively].
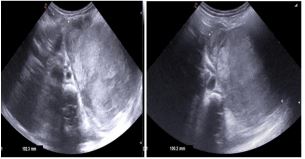
To evaluate the abdominal mass, an ultrasound examination of the abdomen was performed (Figure 1a,1b). It revealed an extensive solid polylobulate formation, diffusely in homogeneous. At the MRI of the abdomen with contrast medium than performed (Figure 2a,2b) the mass was isointense in the T1 and globally hyperintense in the T2; there were hyperintense areas in both T1 and T2, suggestive for post-hemorrhagic areas. The mass seemed to origin from the kidney. The “claw-sign” was present (Figure 2c).
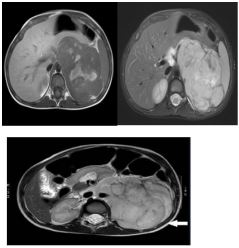


No other lesions were found. This imaging findings were typical of WT so that chemotherapy was started directly, according to the UMBRELLA protocol. When our patient made the second MRI of follow-up of the abdomen (Figure 3a,3b) the mass was slightly increased in size although the therapy. Given this lack of response, in the suspicion of a NB, a biopsy of the mass was performed, that confirmed the diagnoses. In addition, a Scintigraphy with Metaiodobenzilguanidin (MIBG) (Figure 4a,4b) was performed which showed iperaccumulations around the lesion with sparing of the central area.
Discussion
Calcifications are uncommon in WT, only in 9% of the cases [5], while the so-called “Claw-sign”, which refers to the sharp angles that parenchyma forms around the mass is typically associated with WT [3]. The age of onset is an important element to consider in the differential diagnosis between WT and NB [6], and our patient was in the peak incidence of WT. In addition, the urinary cathecolamines, which are positive in about 90% of neuroblastoma cases [7], were negative. In our patient the severe inhomogeneity, the intralesional hemorrhages, the absence ofcalcifications and the fact that the mass appeared to be of renal parenchyma led to thediagnosis of Wilms tumor. This hypothesis was also supported by the negativity of urinarycatecholamines at the time of diagnosis.
According to the International Society of Pediatric Oncology (SIOP), pre-operative chemotherapy with subsequent radical nephrectomy [8] is the clinical strategy in the management of WT. The protocol also recommends that for WT, the diagnosis should be made on the behalf of the imaging findings and biopsy is not generally necessary [9]; medical treatment is usually started directly with consequent follow-up. Our little patient therefore begun the cytoreductive therapy. After evaluating the lack of response of the mass, since the increased volume evaluated in the follow-up MRI, it was decided to carry out atru-cut biopsy of the mass. The histological examination demonstrated a Neuroblastoma poor stroma (poorly differentiated). NB tends to infiltrate the bone marrow and to evaluate the presence of marrow invasion, it is performed bilateral marrow aspirates. On the other hand, the Scintigraphy with Metaiodobenzilguanidin (MIBG) is used to evaluate the presence of bone metastasis for the staging.
Conclusion
In conclusion, the differential diagnoses between WT and NB, that together represent about the 50% of abdominal masses in pediatric age, it is not always possible with imaging, as in this case. The mass presented all the radiological characteristics of a WT, which led to the initial misdiagnosis.
References
- Heck Julia E, et al. The epidemiology of neuroblastoma: A review. Paediatric and perinatal epidemiology. 2009; 23: 125-143.
- Park Julie R, Angelika Eggert, Huib Caron. Neuroblastoma: Biology, prognosis, and treatment. Pediatric Clinics of North America. 2008; 55: 97-120.
- Dumba M, Jawad N, Mc Hugh K. Neuroblastoma and nephroblastoma: a radiological review. Cancerimaging. 2015; 15.
- XuY, Wang J, Peng Y, Zeng J. CTcharacteristics of primary retroperitonealneoplasms in children. Eur J Rad. 2010; 75: 321–328.
- Brisse HJ, Smets AM, Kaste SC, et al. Imaging in unilateral Wilmstumour. Pediatr Radio. 2008; l38: 18–29.
- Chung E, Graeber A, Conran R. Renal Tumors of Childhood: Radiologic-Pathologic Correlation Part 1. The 1st Decade: From the Radiologic Pathology Archives. Radiographics. 2016; 36: 499-522.
- Strenger, Volker, et al. Diagnostic and prognostic impact of urinary catecholamines in neuroblast omapatients. Pediatric blood & cancer. 2007; 48: 504-509.
- Pater L, Melchior P, Rübe C, Cooper BT, McAleer MF, Kalapurakal JA, Paulino AC. Wilms tumor. Pediatric Blood & Cancer. 2021; 68: e28257.
- Vujanić Gordan M, et al. The role of biopsy in the diagnosis of renal tumors of childhood: Results of the UKCCSG Wilms tumor study 3. Medical and pediatriconcology. 2003; 40: 18-22.