
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case of thoracoscopic-assisted tracheal tumor resection and tracheal reconstruction
Zehui Shi1,2; Zuhao Zhang2; Xiao Jiang3; Xuejiao Li1,2; Ziwei Guo1,2; Qiyong Wu1*
1The Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University, Changzhou, China.
2Dalian Medical University, Dalian, China.
3Department of Endocrine and Metabolism, The Second Affi liated Hospital of Dalian Medical University, Dalian, China.
*Corresponding Author : Qiyong Wu
Department of Thoracic and Cardiac Surgery, The Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University, Changzhou 213004, China.
Email: wqyxycxy@aliyun.com
ORCID ID: 0000-0002-6281-5622
Received : Aug 01, 2022
Accepted : Aug 24, 2022
Published : Aug 31, 2022
Archived : www.jcimcr.org
Copyright : © Wu Q (2022).
Abstract
Primary tracheal tumor is a disease with low morbidity and poor prognosis. Surgical resection is the main treatment. It is difficult to treat tracheal tumors, while involving tracheal reconstruction operations are more complicated. We report a case of tracheal tumor patient. The large tumor was located above the tracheal carina and the opening of the left main bronchus. The lumen of the left main bronchus was significantly narrowed. The patient was received thoracoscopic-assisted tracheal tumor resection and tracheal reconstruction under general anesthesia. The patient recovered healthy after operation without serious complications. Thoracoscopic-assisted tracheal tumor resection provides a flexible surgical option for the treatment of this disease.
Keywords: Tracheal tumor resection; Tracheal stenosis; Tracheal reconstruction; Thoracoscopy-assisted.
Citation: Shi Z, Zhang Z, Jiang X, Li X, Wu Q, et al. A case of thoracoscopic-assisted tracheal tumor resection and tracheal reconstruction. J Clin Images Med Case Rep. 2022; 3(8): 2023.
Background
Primary tracheal tumors are rare disorders which accounting for 0.2% of respiratory tumors, about 0.1-0.2/100,000 people, [1,2]. Squamous cell carcinoma and adenoid cystic carcinoma are the main pathological types. Most of the tracheal tumors are malignant, with insidious progression and lack of specific clinical manifestations in the early stage. Hemoptysis, irritating cough are the common clinical manifestations [3]. Tracheal stenosis, significant dyspnea, even life-threatening will be caused with development of the tumor [4]. Surgical resection and tracheal reconstruction are the main treatment for tracheal tumors. Other treatment, such as chemoradiotherapy and bronchoscopy techniques, provide palliative care but are incurable. Patients are at risk of tumor recurrence or distant metastases after chemoradiotherapy and bronchoscopy techniques [3]. Most tracheal tumors are diagnosed late, and whether or not to operate depends on the anatomical structure of the trachea and the location of the tumor. At present, the 5-year survival rate of tracheal tumors is only 27% [5]. Traditional tracheal surgery is based on the right thoracotomy or median thoracotomy. In recent years, with the development of laparoscopic technology, thoracoscopy has been choice for tracheal tumor resection and tracheal reconstruction [6]. We used thoracoscopic-assisted techniques with less surgical trauma and clearer surgical field, combined with the surgical plan of transthoracic tracheal intubation, which fully ensured the intraoperative life safety of the patient and perfectly realized the patient’s tracheal tumor removal and tracheal reconstruction.
Case report
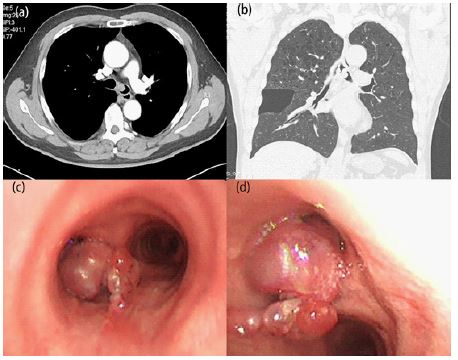
A 58-year-old male were admitted to the Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University, for “episodic dry cough for 2 months”. He had no accompanying symptoms such as sputum, hemoptysis, and dyspnea during coughing. After taking oral “roxithromycin and azithromycin” by himself, there was no recovery. He has a history of smoking and “coronary atherosclerosis”, and underwent “coronary stenting” in our hospital 6 years ago. After admission, a chest computed tomography scan showed a mass located in the tracheal carina and left main bronchus, with a size of about 1.5 cm × 2 cm, and the formation of bullae in the middle lobe of the right lung (Figure 1a,b). Fiberoptic bronchoscopy revealed a prominent tumor in the tracheal carina and left main bronchus, almost completely obstructing the left main bronchus (Figure 1c,d). The lumen is severely narrowed and the distal end cannot be accessed. Bronchoalveolar lavage, brushing, and bronchoscopic biopsy suggested tracheal malignancy. Pulmonary function, electrocardiogram, and echocardiography were checked before operation, and contraindications to surgery were excluded. After obtaining the patient’s informed consent, it was decided to perform thoracoscopic-assisted tracheal tumor resection and tracheoplasty.
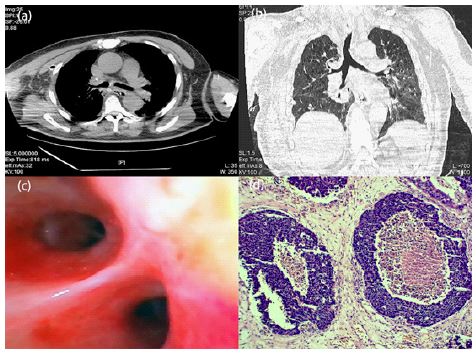
After admission, the patient was connected to a monitor with HR 100 beats/min, BP 140/90 mmHg, RR 16 beats/min, and oxygen was administered by face mask with SpO2 98% to 99%. After induction of anesthesia, the patient was placed in the right lateral position, and an incision of approximately 10 cm was made in the 4th intercostal space in the right anterior axillary line and 1.5 cm in the 7th intercostal space in the midaxillary line. The thoracoscope was inserted and the thoracic cavity was explored. A mass of about 2 cm in size was seen above the tracheal ridge and the opening of the left main bronchus. The mass protruded into the lumen and showed infiltrative growth, and the lumen of the left main trachea was obviously narrowed. The lumen of the left main trachea was obviously narrowed. The paratracheal and infraluminal lymph nodes were slightly enlarged and did not invade other surrounding organs. We opened the mediastinal pleura with an electric hook, and then freed and ligated the odd vein. After fully exposing the intact main trachea, rongeurs, left and right main bronchi, and clearing the surrounding lymph nodes, we disconnected the patient from the ventilator and used the electric hook and ultrasonic knife to cut the right main bronchus 0.5 cm from the opening of the right main bronchus, and the left main bronchus 1.5 cm from the opening of the left main bronchus. The tracheal tumor specimen was sent for pathological examination. At this time, mechanical ventilation could not maintain normal oxygenation, so we placed a tracheal tube in the left main bronchus through the thoracotomy field to maintain ventilation for the patient. After the rapid pathology results showed no cancerous tissue at the cut edge, tracheoplasty and tracheobronchial anastomosis were performed. At the time of anastomosis, bronchoscopic exploration and measurement of the proximal and distal disconnected trachea were performed. Since the length exceeded the length of the tracheal tube and normal ventilation could not be maintained, it was decided to insert a tube changer. The two tracheal tubes were extended and modified and replaced with 7.0 mm tubes. The transthoracic tracheal tube was removed and the anterior end of the modified tracheal tube was sent to the distal left main bronchial incision margin as a support for the anastomosis of the left main bronchus with the main trachea, and the posterior wall membrane was closed with continuous 3-0 prolene sutures and the anterior wall cartilage ring was closed with intermittent 3-0 buckwheat sutures. As the patient had alveoli, we removed the right alveoli using a cutter closure, and at the same time released the inferior pulmonary ligament, opened the pericardium to release the right hilum, opened the lateral wall of the main trachea above the main trachea-left main bronchus anastomosis, and end-lateral anastomosis of the right main bronchus stump with the main trachea, with continuous sutures of 3-0 prolene suture in the lower half and interrupted sutures of 3-0 buckwheat suture in the upper half. Sputum was aspirated during the whole procedure to avoid blood and secretions from entering the lung tissue. After the tracheal suture was closed, the wound was adequately hemostatic, the chest cavity was flushed, and the bulging lung was examined without active bleeding or anastomotic leakage. Bronchoscopy was performed to confirm tracheal patency, closed chest drainage was placed, and the chest was closed at various levels. To relieve post-tracheoplasty tension, sutured mandibular traction was used to keep the patient in a cervical flexion position. The operative time was 4 h. Intraoperative bleeding was about 100 ml, and the patient was transferred to the intensive care unit after surgery and recovered well. On the 8th postoperative day, the drainage was removed and mechanical ventilation was stopped, oxygen saturation was maintained at 98-100%, and the patient was transferred to a general ward with a low head for 2 weeks. Postoperative CT showed a patent trachea, and the patient was discharged 20 days after surgery. Pathological results showed large cell neuroendocrine carcinoma, no tumor tissue was found in any of the tracheal marginal sites, and no tumor metastasis was seen in lymph nodes. Immunohistochemistry: CKp (+), Syn (+), CgA (+), Ki-67 (+, 60%), TTF-1 (+), CK7 (+), NapsinA (-), P63 (-), P40 (-), CK5/6 (-). Combined with the patient’s postoperative pathology, the patient was advised to undergo a combination of postoperative treatment, including radiotherapy, and regular review.

Discussion
Primary tracheal tumors are less common, mostly secondary to direct invasion or bloodstream dissemination, with squamous cell carcinoma and adenoid cystic carcinoma as the main pathological types [3]. Large cell neuroendocrine carcinoma, as the third most common pathological subtype after squamous cell carcinoma and adenoid cystic carcinoma, has better prognosis [7]. The onset of tracheal tumors is insidious and lacks specific clinical manifestations, and most patients first seek medical attention with symptoms such as cough, wheezing and dyspnea, but they are easily misdiagnosed as asthma or bronchitis, leading to delayed diagnosis and affecting treatment [3]. Due to the special anatomical structure of the trachea, symptoms only appear when the obstruction of the tracheal lumen exceeds 50%, and can lead to tracheal stenosis and significant dyspnea when it exceeds 75%, which can be life-threatening when airway obstruction is severe [4]. Therefore, when many patients are diagnosed, it is already difficult to ensure complete surgical removal of the lesion, or even lose the opportunity of surgery [5]. Currently, surgery is the main treatment for tracheal tumors, and other treatment methods include bronchoscopy, chemotherapy and radiation therapy. Tracheal transplantation and tracheal bioengineering are also developing rapidly and may become a viable option in the future as well [3].
Classical trachelectomy is performed through a right-sided open-chest approach or median sternal split, and thoracoscopic-assisted tracheal tumor resection has not been studied much [6]. The first thoracoscopic video-assisted tracheal mass resection and tracheal reconstruction in a spontaneously breathing non-intubated patient was reported by Li et al. in 2016 [8]. Although the procedure is very innovative, the indications for anesthesia and the requirements for anesthesiologists and operators are also extremely demanding. Therefore, we chose to perform tracheal surgery on the patient with the assistance of thoracoscopy. We took incisions at the 4th intercostal space in the right anterior axillary line and the 7th intercostal space in the mid-axillary line in the right chest, breaking the conventional open tracheal surgery and minimizing the surgical trauma to the patient. At the same time, the surgical field is fully exposed and the surgical area is clearly visible, which is conducive to fine surgical operation in a narrow surgical space and improves the accuracy of tracheal anastomosis. Intraoperatively, we need to apply tracheal intubation, thoracoscopic intubation, mechanical ventilation and other devices to fully ensure the safety of the patient up, to be able to properly manage surgery-related complications, and to reduce the risks associated with anesthesia and surgery. We confirmed the feasibility of thoracoscopic-assisted tracheal tumor resection and tracheoplasty. This surgical approach places a higher technical demand on the operator, but the patient is the greatest beneficiary. The thoracoscopic-assisted surgery time is significantly shorter and the surgical approach is more minimally invasive. In addition to this, it reduces postoperative pain and speeds up the recovery time for patients [9]. The patient’s tumor was completely resected with no peripheral and distant metastases by our surgical approach, but considering the patient’s pathological and immunohistochemical findings, combined with reports about tracheal neuroendocrine carcinoma with distant lung metastases even after treatment [10], we strongly recommend the patient to receive comprehensive treatment such as postoperative adjuvant radiotherapy and regular follow-up review to obtain better long-term survival rate.
With the development of thoracoscopic techniques, more and more tracheal tumors will be treated by minimally invasive surgery. Thoracoscopic-assisted tracheal tumor resection provides a flexible surgical option for the treatment of this disease. More patients will benefit from it in the future.
Declarations
Statement of conflict of interest: The authors declare that they have no competing interests.
Consent for publication: Not applicable.
Acknowledgement: Thanks for the approval of the Affiliated Changzhou No. 2 People’s Hospital of Nanjing Medical University and Dalian Medical University.
Data availability: The metabolomic datasets generated during the current study are available from the corresponding author on request.
Author contributions: Conceived and reported the case: Zehui Shi; Constructed figure and table: Xuejiao Li; Wrote and translated: Xiao Jiang. Article correction: Ziwei Guo and Zuhao Zhang.
References
- Junker K. Pathology of tracheal tumors. Thorac Surg Clin. 2014; 24: 7-11.
- Honings J, van Dijck JA, Verhagen AF, van der Heijden HF, Marres HA, et al. Incidence and treatment of tracheal cancer: A nationwide study in the Netherlands. Ann Surg Oncol. 2007; 14: 968-976.
- Diaz Mendoza J, Debiane L, Peralta AR, Simoff M. Tracheal tumors. Curr Opin Pulm Med. 2019; 25: 336-343.
- Allen MS. Malignant tracheal tumors. Mayo Clin Proc. 1993; 68: 680-684.
- Urdaneta AI, Yu JB, Wilson LD. Population based cancer registry analysis of primary tracheal carcinoma. Am J Clin Oncol. 2011; 34: 32-37.
- Li ZH, Dong B, Wu CL, Li SH, Wu B, et al. Case Report: ECMO-Assisted Uniportal Thoracoscopic Tracheal Tumor Resection and Tracheoplasty: A New Breakthrough Method. Front Surg. 2022; 9: 859432.
- Urdaneta AI, Yu JB, Wilson LD. Population based cancer registry analysis of primary tracheal carcinoma. Am J Clin Oncol. 2011; 34: 32-37.
- Li S, Liu J, He J, Dong Q, Liang L, et al. Video-assisted transthoracic surgery resection of a tracheal mass and reconstruction of trachea under non-intubated anesthesia with spontaneous breathing. J Thorac Dis. 2016; 8: 575-585.
- Rocco G. One-port (uniportal) video-assisted thoracic surgical resections - a clear advance. J Thorac Cardiovasc Surg. 2012; 144: S27-S31.
- Brochu V, Tamber GS, Rayes RF, Fiset B, Caglar D, et al. High-Grade Neuroendocrine Carcinoma within a Tracheal Polyp: A Case Report. JTO Clin Res Rep. 2021; 2: 100169.