
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Posterior midline transpedicular approach for third rib neoplasm
*Corresponding Author : Jayakrishnan S
Consultant Cardiothoracic and Vascular Surgeon, Apollo Adlux Hospital, Angamaly, Kerala, India.
Email: jayakrishnans2011@gmail.com
Received : Jul 28, 2022
Accepted : Aug 26, 2022
Published : Sep 02, 2022
Archived : www.jcimcr.org
Copyright : © Jayakrishnan S (2022).
Abstract
Aneurysmal bone cysts are primarily benign neoplastic lesions, often occurring in childhood and adolescent age group. A 27 year old male with neoplastic lesion arising from the posterior end of right third rib, underwent resection without thoracotomy or use of thoracoscopy. In this technique we used posterior midline transpedicular approach and resected with the help of neuronavigation system. Use of neuro navigation system helps to achieve tumour free margin and very usefull in neoplasms closer to the spine. This is a minimally invasive approach for neoplasm arising from the rib without thoracoscopy or thoracotomy.
Citation: Jayakrishnan S. Posterior midline transpedicular approach for third rib neoplasm. J Clin Images Med Case Rep. 2022; 3(9): 2027.
Introduction
Neoplasms of the rib are heterogeneous group, consisting of aggressive and benign entities with large number of overlapping features [1]. Aneurysmal Bone Cysts (ABC) are rare lesions seen typically in adolescent age group. Although primarily benign, up to thirty percent of aneurysmal bone cysts may be secondary to other neoplasms like germ cell tumour, osteosarcomas, fibrous dysplasia or osteoid osteomas especially in adults [1]. So the resection of ABCs are mandatory in adults when they are symptomatic. Symptoms vary from pain and swelling adjacent to the affected bone as well as dyspnoea and pathological fractures. They are commonly observed in the posterior arch of the ribs. This report describes an innovative posterior midline approach for an aneurysmal bone cyst, from third rib, closer to the spine.
Case history
A 27 year old male engineer, with back pain, was evaluated and found to have Lytic lesion in the posterior end of the third rib with cortical break and pleural based soft tissue thickening. A differential diagnosis of metastasis, peripheral lung tumour or tuberculosis was considered. PET CT revealed FDG non avid solitary, permeative, and expansible lytic lesion. There was an adjacent soft tissue component, involving posterior aspect of right 3rd rib suggestive of eosinophilic granuloma /Ewings sarcoma. (Figure 1A,1B). Evidence of primary or secondary malignancy elsewhere was not found in the whole body survey. Considering the CT, PET findings and symptomatic nature of the disease, surgical excision of the lesion was planned. The tumour was excised through posterior midline trans pedicular approach with the aid of neuro navigation. This involved preoperative fusion of CT and PET images and surface marking using Striker Neuronavigation system (Figure 1C). After draping the patient, the entry point and trajectory was marked. Subperiosteal dissection of both lamina and pedicle of third thoracic vertebra after entering through posterior midline incision . The right transverse process and attachment of 3rd rib head was identified and reconfirmed with neuronavigation. It also aids to locate the tumor and tumor free margin. Using a Gigly saw, supramarginal excision of the tumor on both the sides was performed without any chord or neruve injury (Figure 2A,2B). By adopting this novel approach, a large postero-lateral incision with its morbidities, thoracoscopy and single lung ventilation was avoided. The neuro navigation aided in resecting the rib, with a tumour free margin at both anterior and posterior ends as well as allowing tumour free pleural margin .The histopathological study revealed aneurysmal bone cyst (Figure 2C) with free margins on all sides. Hence no further chemo/radiation were required. This report describes novel minimalistic posterior midline approach for posterior rib neoplasm.
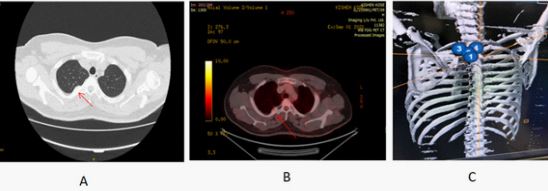
B - PET CT Showing the lytic lesion.
C - Neuronavigation image during the pre-operative surface marking.
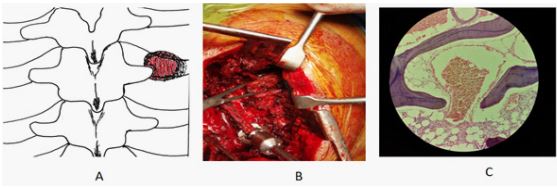
B - Intra-operative photograph showing the tumour.
C - Microphotograph showing the features of aneurysmal bone cyst.
Discussion
Primary Aneurysmal bone cysts are independent neoplasms. Despite the evidence of possible malignant transformation in the form of oncogenic activation of USP6 gene in ABC [1,2], the tumor is generally thought to have no malignant potential but requires resection if they are symptomatic [1]. The rib neoplasms are usually approached through thoracotomy or using Video Assisted Thoracoscopic Surgical (VATS) techniques. Our non thoracotomy approach by a, single midline incision for these tumors of posterior ribs, can be used routinely for complete and safe resection with tumor free margins. The surgical exposure allows for laminectomy, facetectomy, costo transversectomy, with rib resection and complete tumor excision [3]. We have successfully used the posterior midline approach in this patient.
This technique avoids complications of regular thoracotomy which includes bleeding, infection, pneumothorax, pleural effusion, shoulder dysfunction and muscular pain which can cause splinting and decreased inspiratory efforts. Furthur there is reduced compliance to physiotherapy, and causes post-thoracotomy pain syndrome [4,5]. Chronic pain after thoracotomy affects up to 57% of patients at 3 months and 47% at 6 months [6]. Video-Assisted Thoracoscopic Surgery (VATS) may be used for rib resection to reduce pain of intercostal nerve damage by limiting the number and size of intercostal ports used. However, the incidence of chronic pain appears to be similar to open thoracotomy [7]. This non thoracotomy technique preserves paraspinal muscle viability, bulk and innervation, and reduces overall morbidity while ensuring safe spinal and paraspinal dissection under neuronavigation. Neuronavigation enables accurate surgery, and may ultimately reduce complications and improve outcome. It allows painless, image-guided surgery, and can be used in all procedures where paraspinal dissection is involved and resection margins needs to be precisely defined [8]. This approach reduces the muscle cuts and splits, reducing inflammation and ensures safety of the neural structures including dorsal primary rami. Also it reduces the incision length as it allows more than adequate exposure through a precise and limited muscle elevation over concerned rib while avoiding long length of muscle mobilization [5]. Also, the surgical approach is the same as for laminectomy, and therefore, access to the rib head neoplasm is easy, fast and safe. In this era of minimally invasive surgery, overall blood loss and muscle-related morbidities such as pain and scarring are significantly reduced.
References
- Howard Y Park, Sara K Yang, William L Sheppard, Vishal Hegde, Stephen D Zoller, et al. Current management of aneurismal bone cyst Curr Rev Musculoskelet Med. 2016; 9: 435–444. Published online 2016 Oct 24.
- Ye Y, Pringle LM, Lau AW, et al. TRE17/USP6 oncogene translocated in aneurysmal bone cyst induces matrix metalloproteinase production via activation of NF-kappaB. Oncogene. 2010; 29: 3619–3629.
- Payer M, Radovanovic I, Jost G. Resection of thoracic dumbbell neurinomas: Single postero-lateral approachor combined posterior and transthoracic approach? J Clin Neurosci. 2006; 13: 690–693.
- Sakakura N, Mizuno T, Arimura T, Kuroda H, Sakao Y, et al. Design variations in vertical muscle-sparing thoracotomy. J Thorac Dis. 2018; 10: 5115-5119.
- Reid JC, Jamieson A, Bond J, Versi BM, Nagar A, et al. A pilot study of the incidence of post-thoracotomy pulmonary complications and the effectiveness of pre-thoracotomy physiotherapy patient education. Physiother Can. 2010 Winter; 62: 66-74.
- Bayman EO, Brennan TJ. Incidence and severity of chronic pain at 3 and 6 months after thoracotomy: meta-analysis. J Pain 2014; 15: 887–897.
- Searle RD, Simpson MP, Simpson KH, Milton R, Bennett MI, et al. Can chronic neuropathic pain following thoracic surgery be predicted during the postoperative period? Interact Cardiovasc Thorac Surg. 2009; 9: 999–1002.
- Hayhurst C, Byrne P, Eldridge PR, Malluci CL. Application of electromagnetic technology to neuronavigation: A revolution in image-guided neurosurgery. Technical note. J Neurosurg. 2009; 111: 1179–1184.