
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Radiocarpal collapse after a radiocarpal fracture
dislocation despite surgical treatment
Maximilian Quentin Wenzel1; Valeska Hofmann3; Amelie Deluca2*; Florian Wichlas1
1Department of Orthopedics and Traumatology, Salzburg University Hospital, Paracelsus Medical University, 5020 Salzburg, Austria.
2Institute of Tendon and Bone Regeneration, Spinal Cord Injury & Tissue Regeneration Center Salzburg, 5020 Salzburg, Austria.
3Complex Oncology Center, Department of Medical oncology; Russe, Bulgaria
*Corresponding Author : Amelie Deluca
Institute of Tendon and Bone Regeneration Paracelsus Medical University, Strubergasse 21, 5020 Salzburg, Austria.
Phone: 0043-664-4490016;
Email: amelie.deluca@pmu.ac.at
Received : Aug 02, 2022
Accepted : Aug 26, 2022
Published : Sep 02, 2022
Archived : www.jcimcr.org
Copyright : © Deluca A (2022).
Abstract
We present a case of a radiocarpal fracture dislocation. The injury of the distal radioulnar joint was initially underestimated and only fixed with screws and a K-wire without addressing the radiocarpal instability. In the further course, the patient developed a painful radiocarpal dislocation and an impaired Range Of Motion (ROM) of the affected wrist. During rescue surgery the carpus was reduced and centralized into the radial fossa. One year later, the patient was mainly pain free and the ROM improved. Nevertheless, the radiographs showed signs of posttraumatic osteoarthritis already.
These complex injuries are rare, often mistaken for distal radius fractures, and highly unstable. Indirect signs for instability need to be recognized, such as carpal bony tears and subluxations.
The goal of treatment is to stabilize the reduced joint by a sufficient osteosynthesis of bony structures and a ligament reconstruction if warranted.
Nevertheless, the outcome is poor with a high rate of posttraumatic osteoarthritis.
Citation: Wenzel MQ, Hofmann V, Deluca A, Wichlas F. Radiocarpal collapse after a radiocarpal fracture dislocation despite surgical treatment. J Clin Images Med Case Rep. 2022; 3(9): 2029.
Background
The radiocarpal fracture dislocation is a rare traumatological event, mainly caused by high energy trauma. The mechanism is a shearing or rotational movement, sometimes combined with a radiocarpal dislocation and a rupture of the radiocarpal ligaments. It is a severe injury and needs recognition as such to achieve the best functional outcome. In most cases, the treatment consists of anatomical reduction and internal fixation together with a ligament repair [1-5].
We present a case of an insufficiently treated radiocarpal fracture dislocation and its salvage procedure.
Case description
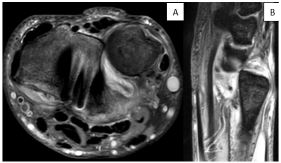
The patient was a 42-year-old male storekeeper and injured in a motorcycle accident. Besides a pelvic fracture (classified AO C1) and a fracture of the left distal radius (AO 23 B1), he sustained a distal radius fracture of the right side. The radiographs showed a distal radius fracture, classified AO 2R3B3.3, with palmar and dorsal osseous ligament tears of the carpus (Figure 1). The carpus was centralized, showed no signs of dislocation and the Distal Radio-Ulnar Joint (DRUJ) seemed unaffected. The CT scan showed a small palmar rim fragment and palmar as well as dorsal osseous ligament tears of the carpus, the DRUJ was reduced.

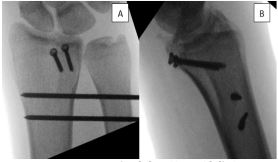
Sixteen days after the initial trauma, the fracture was treated by open reduction and internal fixation with two lag screws for the palmar rim fragment. Intraoperatively, an instability of the DRUJ was diagnosed and temporarily stabilizedulno-radially with two K-wires (1.6 mm) for 6 weeks (Figure 2). The postoperative treatment consisted of immobilization of the wrist and elbow in an above elbow cast for 6 weeks.
The first postoperative X-ray already showed a palmar dislocation of the carpus despite the screw fixation but remained untreated (Figure 3).

The diagnosis and operative revision strategies were discussed with the patient. A total wrist fusion as potential alternative was rejected and the patient decided to undergo another rescue surgery, which was performed 4 months after the first surgery.
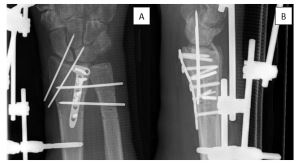
In this operation, a corrective osteotomy of the palmar fragment was performed, using a locking 2.4 mm plate (Synthes LCP 2,4 mm Titanium T-Plate) for fixation. The DRUJ was reduced openly and stabilized ulno-radially with 2 K-wires (1.6 mm), the Triangular Fibrocartilage Complex (TFCC) was fixed with vicrylsutures. A temporary radiocarpal fixation was decided upon intraoperatively and performed using 2 K-wires (1.6 mm) for 6 weeks. Additionally, an external fixator was applied for 6 weeks from the radial shaft to the second metacarpal bone.
An additional surgical revision was necessary 5 days later, because one screw was intra articular in the DRUJ and had to be removed (Figure 5).
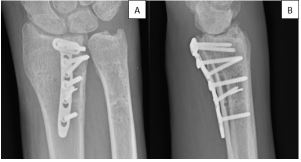
One year after the rescue surgery, the patient presented with a range of motion of pronation/supination with 60-0-50 degrees and dorsal extension/palmarflexion with 40-0-20 degrees (Figures 6,7). The patient complained about the limited ROM but only reported about pain when lifting heavy weights. Nevertheless, the severity of his other injuries made it impossible for him to fulfill his previous job.

Discussion
Radiocarpal fracture dislocations are rare injuries and account for 0.2% of all wrist injuries [6]. Radiocarpal dislocations occur mainly in combination with distal radius fractures combined with disruptions of the radiocarpal ligaments as well as a fracture of the ulnar styloid. These severe injuries need to be distinguished from simple reversed Barton AO 23 B3 fractures [1,4].
Besides standard diagnostics, a CT scan is mandatory to detect all bony tears and carpal instabilities preoperatively.
Not necessarily all radiocarpal dislocations have to be dislocated at the time of arrival [5]. Indirect sings for this injury, such as subluxation in the radiocarpal joint, minor fractures of the distal rim of the radius (dorsal or palmar), and bony avulsions of radiocarpal ligaments lead to the diagnosis. Due to its instability, radiocarpal dislocations need surgical treatment in terms of open reduction, internal fixation, and ligament repair [7-9].
As this type of injury has been recognized, different classifications for radiocarpal fractured is locations have been proposed. The first was published in 1985 by Moneim and distinguishes between Type I (dislocation of only the radiocarpal joint), and type II (additional intercarpal dislocation). However, this classification is rarely used [10]. Another one has been proposed by Dumontier [2]. It distinguishes between minor radius fractures (group 1), involving less than one-third of the width of the scaphoid fossa, and greater fragments (group 2), involving more than one-third of the width.
Dumontier points out, that the outcome of patients with group-1-injuries, as in our case, is usually poor, whereas group-2-fractures have a better outcome [2]. This undermines the severity of the presented case and the importance of the palmarrim fragment. Small fragments are often a sign of high radiocarpal instability. In our opinion, their anatomic fixation is the mainstay for a stable radiocarpal joint.
A few mistakes have been made in the treatment of our patient. The patient´s wrist instability was not recognized although indirect signs were clearly present, probably because the radiocarpal joint was not dislocated. The fracture was treated by simple screw fixation of the palmar fragment. Although an instability of the DRUJ was disclosed intraoperatively, it was addressed without any suspicion for further injuriesof the radiocarpal joint. The screw fixation was probably insufficient, and the palmar fragment dislocated secondarily.
The palmar distal radius rim fragment seems to be a key fragment for the palmar stability of the wrist, as it has already been reportedin a small series of five cases which all presented with palmar radiocarpaldislocations [11]. In our case, the increasing radiocarpal instability was primarily detected within the postoperative X-ray’s and rescue surgery was planned. The goal of this complex surgery, 4 months after initial surgery, was to centralize and stabilize the carpus in the radiusat any cost, which meant to use radiocarpal K-wires and an external fixator, additionally to the plate.
The initial X-ray examination already showed small dorsal and palmarshear fragments, indicating ruptures of the radiocarpal ligaments with potential instability. Besides, a subtitle subluxation in the radiocarpal joint can be observed (Figure 1). A thorough preoperative physical examination, eventually under image intensifier, could have led to the diagnosis and discovered the severe instability of the carpus. In this case, maybe an initial plate fixation using a distal rim plate, or a hook plate could have guaranteed the stability of the palmar rim fragment [12]. Nevertheless, if instability persists, ligamental- and capsular-tears need to be addressed. In radiocarpal fracture dislocations, ligamental lesions usually occur palmarly and dorsally [13]. Given the severity of this injury, a palmar and dorsal approach can be necessary for ligamental and capsular repair.If sutures are likely to be insufficient, it has been suggested to use anchors instead [14].
As in our case one year after rescue surgery (Figure 6), the development of early osteoarthritis are very common as described in most cases [2,6,15]. Based on the serious sequelae of this injury, a wrist fusion is an alternative to our rescue attempt. Nevertheless, as this injury occurs mainly in young patients, we preferred a joint-preserving surgery. This underlines the need for early recognition and stable fixation of the injury.
Conclusion
Conclusively, radiocarpal fracture dislocations are rare and underestimated injuries. The instability of the radiocarpal joint and DRUJ needs to be distinguished from simple reversed AO 23 B3 Barton fractures. The complex instability must be detected and treated surgically by osteosynthesis and joint stabilizing measures, such as sutures, transfixing K-wires or even external fixation. The palmar rim fragment fixation is the key for a stable radiocarpal joint. Nevertheless, the results are commonly poor with a high rate of developing posttraumatic osteoarthritis. A radiocarpal arthrodesis can therefore be an alternative.
Declarations
Conflicts of interest: The authors have no relevant financial or non-financial interests to disclose.
The authors have no conflicts of interest to declare that are relevant to the content of this article.
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in the subject matter or materials discussed in this manuscript.
The authors have no financial or proprietary interests in any material discussed in this article.
Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
This article does not contain any studies with animals performed by any of the authors.
Informed consent: Informed consent was obtained from all individual participants included in the study.
References
- Bhashyam AR, et al., Dorsal Barton fracture is a variation of dorsal radiocarpal dislocation: a clinical study. J Hand Surg Eur. 2019; 44: 1065-1071.
- Dumontier C, et al. Radiocarpal dislocations: Classification and proposal for treatment. A review of twenty-seven cases. J Bone Joint Surg Am. 2001; 83: 212-218.
- Harness NG, et al. Loss of fixation of the volar lunate facet fragment in fractures of the distal part of the radius. J Bone Joint Surg Am. 2004; 86: 1900-1908.
- Ilyas AM and CS Mudgal, Radiocarpal fracture-dislocations. J Am Acad Orthop Surg, 2008; 16: 647-655.
- Souer JS, et al, Case reports: Volar marginal articular fractures with loss of articular apposition. Hand (NY). 2010; 5: 195-199.
- Spiry C, et al. Radiocarpal dislocations and fracture-dislocations: Injury types and long-term outcomes. Orthop Traumatol Surg Res. 2018; 104: 261-266.
- Bilos ZJ, Pankovich AM, Yelda S. Fracture-dislocation of the radiocarpal joint. J Bone Joint Surg Am. 1977; 59: 198-203.
- Jardin E, et al. Open volar radiocarpal dislocation with extensive dorsal ligament and extensor tendon damage: A case report and review of literature. Hand Surg Rehabil. 2016; 35: 127-34.
- Howard RF, DP Slawski, LA Gilula. Isolated palmar radiocarpal dislocation and ulnar translocation: A case report and review of the literature. J Hand Surg Am. 1997; 22: 78-82.
- Moneim MS, JT Bolger, GE Omer. Radiocarpal dislocation-classification and rationale for management. Clin Orthop Relat Res. 1985: 199-209.
- Apergis E, et al. Beware of the ulno-palmar distal radial fragment. J Hand Surg Br. 2002; 27: 139-145.
- Hintringer W, et al. Biomechanical considerations on a CT-based treatment-oriented classification in radius fractures. Arch Orthop Trauma Surg. 2020; 140: 595-609.
- Le Nen D, et al. [Luxation-fractures of the radiocarpal joint. Clinical study of 6 cases and general review]. Ann Chir Main Memb Super. 1991; 10: 5-12.
- Hofmeister EP, et al. Surgical reconstruction of a late-presenting volar radiocarpal dislocation: A case report. Am J Orthop (Belle Mead NJ). 2008; 37: 96-99.
- Schoenecker PL, et al. Radiocarpal fracture-dislocation. Clin Orthop Relat Res. 1985; 237-244.