
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Renal cell carcinoma with tumour thrombus extending in duplicated inferior vena cava: A rarity with management conundrum
Gurvansh Singh Sachdev; Arun Chawla*; Anshuman Singh; Vivekanand Hiremath
Department of Urology and Renal Transplant, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, Karnataka, India.
*Corresponding Author : Arun Chawla
Head of Department, Department of Urology and Renal Transplant, Kasturba Medical College, Academy of Higher Education, Manipal, Karnataka, India.
Email: gurvanshsachdev@yahoo.in
Received : Aug 05, 2022
Accepted : Aug 29, 2022
Published : Sep 05, 2022
Archived : www.jcimcr.org
Copyright : © Chawla A (2022).
Abstract
DIVC may play a role as a confounding factor in imaging diagnostic tests and also may represent a hazard for inadvertent injury and bleeding during surgery.
Careful interpretation Radiological investigations help to define such anomalies and avoid significant morbidity during surgical exploration.
We present a case of renal cell carcinoma involving Right kidney with tumor thrombus extending into both venae cava. Triphasic Contrast-Enhanced Computerized Tomography (CECT) scan of abdomen with three-dimensional reconstruction showed duplicated left sided IVC, Heterogeneously enhancing intraluminal soft tissue density filling defect was seen along the entire length of right renal vein, also crossing the midline to the left sided duplicated IVC -s/o tumour thrombus. Patient underwent right radical nephrectomy with tumour thrombectomy. Cavotomy was done at the junction of right renal vein and right IVC.
Entire thrombus was delivered intact. Histopathological examination showed papillary renal cell carcinoma (type II) stage pT3bN1Mx. IVC thrombus showed clusters of malignant cells of same morphology as tumor entangled in thrombus. The patient is doing well at 3 months of follow-up.
Keywords: DIVC; RCC; Tumor thrombus; Thrombectomy.
Abbreviations: DIVC: Duplicated Inferior Vena Cava; RCC: Renal Cell Carcinoma; CECT: Contrast Enhanced Computerized Tomography.
Citation: Sachdev GS, Chawla A, Singh A, Hiremath V. Renal cell carcinoma with tumour thrombus extending in duplicated inferior vena cava: A rarity with management conundrum. J Clin Images Med Case Rep. 2022; 3(9): 2031.
Introduction
Congenital anomalies of inferior vena cava are extremely rare, reflecting the complexity of the embryological development of these structures. Duplication of IVC (DIVC) occurs in 0.7% of population. DIVC may play a role as a confounding factor in imaging diagnostic tests and also may represent a hazard for inadvertent injury and bleeding during surgery.
We describe a patient with right RCC with DIVC and presence of tumour thrombus involving right renal vein and both IVCs, treated by right radical nephrectomy with vena caval thrombectomy.
Case presentation
A 74 year old diabetic man was admitted with complaints of right flank pain since two months and history of passage of blood clots in urine. Physical examination, haematological and biochemical parameters were unremarkable.
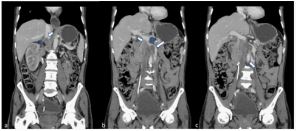
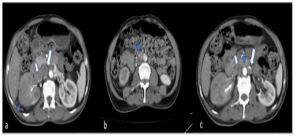
Ultrasonography of abdomen showed a bulky kidney with irregular solid mass of size 4 x 3 cm in right kidney. Triphasic Contrast-Enhanced Computerized Tomography (CECT) scan of abdomen with three-dimensional reconstruction revealed heterogeneously enhancing soft tissue density lesion predominantly in the right lower pole extending into the renal pelvis, extending into the calyces and the proximal ureter. Duplicated left sided IVC was seen as a continuation of left common iliac vein, crossing anterior to the aorta just above the level of left renal vein to join the right sided IVC. Heterogeneously enhancing intraluminal soft tissue density filling defect was seen along the entire length of right renal vein, extending into the supra and infrarenal portion of right IVC (for a length of (14.0 cm) and also crossing the midline to the left sided duplicated IVC (for a length of (4.0 cm) - s/o tumour thrombus. Left renal vein was free from tumour thrombus (Figure 1 and Figure 2).


Patient was taken up for right radical nephrectomy, with tumour thrombectomy through a transperitoneal Chevron incision with extension in midline upto xiphisternum in supine position. Hilar dissection done and right IVC was bared. Right IVC was seen communicating with left IVC anterior to the aorta with the isthmus at the communication at just superior to the level of left renal vein. Tumour thrombus was seen extending from right renal vein into the suprarenal and infrarenal portion of right IVC and periosteal region of left IVC. Few enlarged retrocaval, precaval and aortocaval lymph nodes were also noted. Right renal artery and ureter were ligated and entire kidney mobilized outside Gerota’s fascia, leaving the kidney attached only by the right renal vein. Leftcolon was mobilized and left IVC was bared. Left renal vein was noted to be free from tumour thrombus. Infrarenal Right and left IVCs, left renal vein, and suprarenal IVC just below liver proximal to tumour were clamped in that order. Cavotomy was done at the junction of right renal vein and right IVC. Entire thrombus was delivered intact following which IVC was closed using Prolene 5-0 suture (Figure 3 and Figure 4).
Abdominal closure was done in two layers after placement of a single pelvic drain. Estimated blood loss was 550 ml with one unit of PRBC transfusion done intra operatively. Postoperative period was uneventful with drain removal on third postoperative day. Patient was allowed per orally on second postoperative day and discharged on fourth postoperative day. Histopathological examination showed papillary renal cell carcinoma (type II) stage pT3bN1Mx. Hilar and retroperitoneal lymph nodes were positive for metastasis. IVC thrombus showed clusters of malignant cells of same morphology as tumorentangled in thrombus. The patient is doing well at 3 months of follow-up.
Discussion
The IVC is formed between weeks 6 and 10 of gestation. There are several theories accounting for the duplication. It has been estimated that duplication occurs in 0.2–3.0% of the general population. The infrarenal portion of the IVC is formed from two embryonic veins, the supracardinal veins. The right supracardinal vein persists and develops as IVC while the left supracardinal vein regresses. Persistence of both supracardinal veins results in duplication of IVC [1,2].
Three different variants of duplication of inferior vena cava are known i.e Type I or Major duplication: Two bilaterally symmetrical trunks with a preaortic trunk of the same calibre. Type II or minor duplication with two bilaterally symmetrical trunks, but it is smaller than the preaortic trunk. In Type III or asymmetric duplication there is small left IVC, larger right IVC and even larger preaortic trunk [3]. Our patient was noted to have type I duplication.
Chuang categorised the abnormalities of the postrenal segment of the IVC into four categories: Type A is a persistent right posterior cardinal vein (retrocaval ureter), type B is a persistent right supracardinal vein (normal IVC), type C is a persistent left supracardinal vein (left IVC), and type BC is a persistent right and left supracardinal veins (double IVC) [4].
Locally advanced RCC can have a myriad of presentation from haematuria to fatigue, weight loss to lower extremity oedema, ascites and pulmonary embolism [5]. CT plays an important role in delineating the primary renal pathology and the extent of thrombus invasion into IVC. Because thrombus study requires enhancement phase, a multidetector CT has improved the sensitivity and specificity of CT in detecting RCC by improving accuracy of staging and enhancing surgical planning [6,7].
MRI is however the gold standard for demonstrating level and extent of tumour invasion in IVC with a sensitivity close to 100%. Recent studies have however highlighted equal efficacy of both MRI and multidetector CT for evaluation of tumour thrombus [8]. In our case, CECT revealed double vena cava sign with tumor thrombus in both vena cava extending into suprarenal IVC.
Although IVC duplication is usually asymptomatic, it might have significant clinical implications. As an uncommon anomaly, the duplication of IVC can be misdiagnosed as a pathological lesion such as ureteric dilatation or lymphadenopathy on CT images. The left side of a double IVC might be interpreted erroneously as enlarged retroperitoneal lymph nodes [2,9,10,11]. Which might induce preoperative over staging by radiographic imaging in RCC.
The recognition of IVC anomalies becomes important when radiological, interventional, or surgical procedures involve these structures. Diagnosis of DIVC is important when an IVC filter is to be placed for thromboembolic disease [12]. Reports have showed the importance of recognizing a double IVC when performing renal vein sampling or adrenal venography because blood flow carried by the left vena cava will dilute the left renal vein sample [4].
Early ligation of renal artery is an important step in management of such patients. In a study of 82 patients, Ciancio et al proposed early ligation of renal artery as compared with preoperative embolisation of renal tumours and found it significantly reduced bleeding by collapsing many of the collaterals. They also proposed early control of renal artery by ligating it behind the RV [13].
Recognition of DIVC before or during radical nephrectomy can prevent injury to the anomalous vasculature and resulting exsanguinating hemorrhage. It is also important that control of both IVCs be obtained before cavotomy. In the rare instance that tumor thrombus extends into the anomalous vessels, thrombus extraction from both the IVCs has to be ensured, as was done in our case. If the tumor thrombus is seen invading left IVC, the left IVC can be excised. However, resection of the left IVC despite the absence of an interiliac vein does not reduce the venous drainage from the left femoral vein probably because of abundant pelvic venous channels [14]. Lymphatic drainage tends to follow the vessels. Thus, patients with abnormal venous anatomy may have unusual patterns of lymphatic drainage and lymph node metastases. Therefore, lymph node dissection in a patient with a venous anomaly should be altered accordingly whenever indicated [10].
Conclusion
The recognition of congenital IVC anomalies has major clinical implications. In addition to preventing diagnostic errors, careful interpretation of cross-sectional imaging can help to avoid complications arising from venous anomalies unexpectedly encountered during surgery.
References
- Philips E. Embryology, normal anatomy and anomalies. In: Ferris EJ, Hippona FA, Kahn PC, Philips E, Shapiro JH (eds) Venography of the inferior vena cava and its branches. Williams and Wilkins, Baltimore. 1969; 1–32.
- Bass JE, Redwine MD, Kramer LA, Huynh PT, Harris JH, et al. Spectrum of congenital anomalies complicating retroperitoneal surgery. Radiographics. 2000; 20: 639–652.
- Starly B. A rare vascular anomaly - Type III asymmetric duplicated inferior vena cava; Case 12098: European society of radiology. 2014
- Chuang VP, Mena CE, Hoskins PA. Congenital anomalies of the inferior vena cava: Review of embryogenesis and presentation of a simplified classification. Br J Radiol. 1974; 47: 206-213.
- Parekh DJ, Cookson MS, Chapman W, et al. Renal cell carcinoma with renal vein and inferior vena caval involvement: Clinicopathological features, surgical techniques and outcomes. J Urol. 2005; 173: 1897–1902.
- Constantinides C, Recker F, Bruehlmann W, et al. Accuracy of magnetic resonance imaging compared to computerized tomography and renal selective angiography in preoperatively staging renal cell carcinoma. Urol Int. 1991; 47: 181–185.
- Lawrentschuk N, Gani J, Riordan R, et al. Multidetector computed tomography vs magnetic resonance imaging for defining the upper limit of tumour thrombus in renal cell carcinoma: a study and review. BJU Int 2005; 96: 291–295.
- Agarwal S, et al. BMJ Case Rep. 2018;
- Cohen SI, Hochsztein P, Cambio J, Sussett J. Duplicated inferior vena cava misinterpreted by computerized tomography as metastatic retroperitoneal testicular tumor. J Urol. 1982; 128: 389–391.
- Klimberg I, Wajsman Z. Duplicated inferior vena cava simulating retroperitoneal lymphadenopathy in a patient with embryonal cell carcinoma of the testicle. J Urol. 1986; 136: 678–679.
- Evans JC, Earis J, Curtis J. Thrombosed double inferior vena cava mimicking paraaortic lymphadenopathy. Br J Radiol. 2001; 74: 192–194.
- Hhabuchi T, Okagaki T, Arai K, et al. Renal cell carcinoma extending into left side of double inferior vena cava. Urology. 1993; 41: 181-184.
- Ciancio G, Vaidya A, Soloway M. Early ligation of the renal artery using the posterior approach: A basic surgical concept reinforced during resection of large hypervascular renal cell carcinoma with or without inferior vena cava thrombus. BJU Int. 2003; 92: 488–489.
- Reinus WR, Gutierrez FR. Duplication of the inferior vena cava in thromboembolic disease. Chest 1986; 90: 916-918.