
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
In infectious endocarditis, a lesion can hide another one
Monique Boukobza1*; EmilaIlic Habensus2; Jean Pierre Laissy3
1Department of Radiology, Bichat Hospital, 46 rue Henri Huchard, 75018, Paris, Assistance Publique-Hôpitaux de Paris, France.
2Clinical Investigation Center, Assistance Publique-Hôpitaux de Paris, Bichat Claude-Bernard, Hospital, 46 rue Henri Huchard, 75018, Paris, France.
3Department of Radiology, Bichat Hospital, Assistance Publique-Hôpitaux de Paris, Paris, France ; INSERM U1148, Paris, France; Paris University, France.
*Corresponding Author : Monique Boukobza
Department of Radiology, Assistance Publique-Hôpitaux de Paris, Bichat Hospital, 46 rue Henri Huchard, 75018, Paris, France.
Tel: +33 6 24 65 29 32, Fax: +33 1 40 25 83 05;
Email: m.boukobza@orange.fr.
Received : Aug 06, 2022
Accepted : Aug 29, 2022
Published : Sep 05, 2022
Archived : www.jcimcr.org
Copyright : © Monique B (2022).
Abstract
A 24-year-old immune-competent man, with no significant past medical history, presented a Streptococcus viridans Infective Endocarditis (IE). Work-up for IE showed on post-contrast brain CT-scan a ring- enhancing lesion suggesting a cerebral abscess, with a contiguous nodular enhancing lesion. Given this radiological aspect, and because immediate cardiac surgery was indicated, a cerebral angiography was performed, which exhibited an Intracranial Aneurysm (IA) of a distal branch of the left middle cerebral artery. The association of an IIA and a brain abscess is even rare in IE-patients and IIAs can be completely silent.
The interest of the current case is in its unusual radiological presentation. Faced to unusual cerebral imaging findings in IE context, an IIA must be considered and a vascular imaging must be performed urgently, initially by non-invasive methods.
Keywords: Infective endocarditis; Infectious intracranial aneurysm; Brain abscess; Ring-enhancing rain lesion; Emergency; Cerebral angiography; Brain-CT.
Abbreviations: IE: Infectious Endocarditis; IA: Intracranial Aneurysm; IIA: Intracranial Infectious Aneurysm; BA: Brain Abscess.
Citation: Boukobza M, Habensus E, Laissy JP. In infectious endocarditis, a lesion can hide another one. J Clin Images Med Case Rep. 2022; 3(9): 2032.
Introduction
Neurological complications of Infective Endocarditis (IE) occur in 20-40% of cases, can be classified into the following categories: Encephalopathy, ischemic stroke, cerebral hemorrhage, intracranial infectious aneurysms, meningitis and brain abscess.
We report a rare presentation of 2 brain complications in the same IE-patient, whose appearance on brain-CT adds an extra diagnostic challenge
Case presentation
A 24-year-old immune-competent man, with no significant past medical history, presented to the emergency department with a 2-day history of headache and fever. At admission, the patient was febrile at 38.5°C. His blood pressure was 108/66 mm Hg. Physical examination and chest radiography was unremarkable. Blood tests showed leukocytosis (15.6 × 109/L) and blood cultures were positive for Streptococcus viridans.
Transthoracic and transesophageal echocardiography revealed 13 mm mobile vegetation on a bicuspid aortic valve. IE of dental origin was diagnosed and antibiotic treatment was started on. Post-contrast brain CT-scan showed a ring- enhancing lesion suggesting a cerebral abscess, with a contiguous nodular enhancing lesion (Figure 1a, arrow). Given this radiological aspect, and because immediate cardiac surgery was indicated, a cerebral angiography was performed (Figure 1b).
Cerebral angiography exhibited an infectious Intracranial Aneurysm (IIA) of a distal branch (M4) of the left middle cerebral artery (Figures 2a, 2b), which was successfully treated by glue embolization. The day after the patient underwent mechanic aortic valve replacement and mitral valve plasty. Brain and cardiac outcome was favourable.
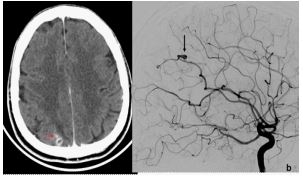
Figure 1b: Catheter cerebral angiography (lateral view, b, c, arrow; orthogonal view, d) shows an aneurysm.

Discussion
Systemic septic emboli from vegetations complicate between 22 and 50% of cases of IE. Previous studies have shown that valve vegetation size (≥10 mm), location (mitral vs aortic) and mobility are associated with higher risk of embolic events [1]. The brain is the most frequent site of embolism in left-sided IE. These septic emboli are at the origin of brain ischemia (the most common complication) or hemorrhage, Brain Abscesses (BAs) and infectious aneurysms.
Symptomatic neurological complications (15–30% of patients) may be the presenting symptom [2,3]. These complications are associated with a high morbidity and mortality. Bacterial brain abscess is a rare complication of IE, affecting from 1% to 5% of patients [2]. Although a BA can present as a solitary lesion like in our case, multiple ring-enhancing lesions are usually seen [2].
The reported frequency (2-4%) of IIAs in IE is probably underestimated, since they may be clinically silent and resolve under antibiotic therapy [4].
They are produced by inflammation and destruction of arterial walls and carry a high risk of rupture and hemorrhage. Staphylococcus aureus and Streptococcus viridans are the most frequent germs found in this context.
Their evolution is unpredictable: IIAs, whether silent or symptomatic, may rupture at any time during the course of the IE. Rapid onset and rupture and rapid growth of IIA during IE have been reported in a few cases [5]. The current case was due to S.viridans and the IIA was silent: the headaches were most likely related to the BA. IIAs diagnosis is challenging and cerebral angiography is the gold standard for diagnosis and monitoring, but is invasive. Many non-invasive imaging methods are widely utilized for the screening of IIAS (Brain angio-CT, MR angiography, contrast-enhanced MR angiography) but all these methods have limitations related to the size these IIAs, often very small- less than 3 mm in diameter- and very distally located on cerebral arteries. The association of an IIA and a brain abscess is even rare in IE-patients.
The interest of the current case is in its unusual radiological presentation: A ring-enhancing abscess with side by side a small round-shaped enhancing lesion, raises the question of the nature of this rounded lesion, and adds an extra diagnostic challenge. Given the IE context, these findings lead to rule out the diagnosis of unruptured IIA. This «signet-ring» aspect may be misinterpreted for a daughter-abscess.
Conclusion
Intracranial aneurysm in IE context may be silent and their association with a brain abscess is even rare.
Faced to unusual cerebral imaging findings in IE context, an IIA must be considered and a vascular imaging must be performed urgently, initially by non-invasive methods.
Declarations
Conflicts of interest: The authors declare that they have no conflicts of interest.
Funding: The authors have not received any financial support.
References
- Yang A, Tan C, Daneman N, et al. Clinical and echocardiographic predictors of embolism in infective endocarditis: Systematic review and meta-analysis. Clin Microbiol Infect. 2019; 25: 178-187.
- Garcia Cabrera E, Fernandez Hidalgo N, Almirante B, et al. Neurological complications of infective endocarditis: Risk factors, outcome, and impact of cardiac surgery: A multicenter observational study. Circulation. 2013; 127: 2272–2284.
- Habib G, Lancellotti P, Antunes MJ, et al. 2015 ESC guidelines for the management of infective endocarditis. Eur Heart J. 2015; 36: 3075–3128.
- Ducruet AF, Hickman ZL, Zacharia BE, et al. Intracranial infectious aneurysms: A comprehensive review. Neurosurg Rev. 2010; 33: 37-46.
- Boukobza M, Naggara O, Duval X, Laissy JP. Acute enlargement, morphological changes, and rupture of intracranial infectious aneurysm in infective endocarditis. Serial imaging. J Clin Neurosci. 2020; 82: 237-240.