
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Fas cell surface death receptor/Fas ligand genetic variants in gastric cancer patients: A case control study
Rezvan Asgari1; Ali Bidmeshkipour2*; Kamran Mansouri1; Mitra Bakhtiari3; Hadi Mozafari1; Amir Abdolmaleki4
1Medical Biology Research Center, Health Technology Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran.
2Department of Biology, Faculty of Sciences, Razi University, Kermanshah, Iran.
3Fertility and Infertility Research Center, Health Technology Institute, Kermanshah University of Medical Sciences, Kermanshah, Iran.
4Department of Anatomical Sciences & Cell Biology, Kermanshah University of Medical Sciences, Kermanshah, Iran.
*Corresponding Author : Ali Bidmeshkipour
Department of Biology, Faculty of Sciences, Razi University, Kermanshah, Iran.
Email: a.bidmeshkipour@gmail.com,
abidmeshki@razi.ac.ir
Received : Aug 06, 2022
Accepted : Aug 31, 2022
Published : Sep 07, 2022
Archived : www.jcimcr.org
Copyright : © Bidmeshkipour A (2022).
Abstract
Background & objectives: Various studies have suggested a correlation between Fas Cell Surface Death Receptor/Fas Ligand (FAS/FASL) variants and multiple types of cancers. The present study aimed to investigate the association between FAS-670A/G and FASL-844C/T and the synergistic effects of both variants on the risk of Gastric Cancer (GC) in the Kurdish population of West of Iran.
Methods: This study was conducted by polymerase chain reaction-restriction fragment length polymorphism technique using MvaI and BsrDI restriction enzymes in 98 GC patients and 103 healthy control individuals.
Results: According to the obtained results, a significant association (P=0.008) of FASL polymorphism among GC patients and the control group was detected. Furthermore, no significant differences were found in the FAS polymorphism frequencies between GC patients and the control group. Codominant and dominant models in FASL polymorphism showed significant protective effects against GC [odds ratio (OR) =0.307, 95% confidence interval (CI) (0.134-0.705), P=0.005; OR=0.205, 95% CI (0.058-0.718), P=0.013 and OR=0.295, 95% CI (0.129-0.673), P=0.004 for models of codominant CC vs. CT, codominant CC vs. TT and dominant, respectively]. Furthermore, the presence of both FAS-670G and FASL-844T alleles represented a significant protective effect against GC occurrence [OR=0.420, 95% CI (0.181-0.975), P=0.043].
Interpretation & conclusions: So far, we believe this is the first study the results of which suggest that FASL gene variation and its synergistic effects with FAS gene could be associated with the risk of GC in the Kurdish population in the west of Iran.
Keywords: FAS-670A/G; FASL-844C/T; Gastric cancer; Synergistic effect; Variant.
Citation: Asgari R, Bidmeshkipour A, Mansouri K, Bakhtiari M, Mozafari H, et al. Fas cell surface death receptor/Fas ligand genetic variants in gastric cancer patients: A case control study. J Clin Images Med Case Rep. 2022; 3(9): 2037.
Introduction
Gastric Cancer (GC) is one of the most common malignancies and the second most common cause of cancer-related deaths in human societies [1]. GC, is affected by various environmental and genetic factors. According to the genetic background, lifestyle, diet, alcohol consumption, smoking and pathogenic infections, the prevalence of this type of cancer varies between populations [2-6]. Single-Nucleotide Polymorphisms (SNPs), as common disorders, have an essential role in pathogenesis of GC. At the outset various human diseases, such as cancers, are associated with apoptosis dysregulation. Apoptosis is one of the most important regulatory mechanisms in cellular homoeostasis, regulation of cell density and removing undesirable multicellular organisms [7]. Programmed cell death occurs via two pathways: intrinsic or mitochondrial dependent and extrinsic or receptor mediated8. Interaction between FAS Cell Surface Death Receptor (FAS) and Fas Ligand (FASL) is considered a crucial factor particularly in the in extrinsic pathways [9,10].
According to previous reports, association between genetic polymorphisms is involved in apoptosis and cancer incidence [11,12]. FAS (Apo-1, CD-23) and its normal ligand (FASL, CD952) have a vital role in initiating the apoptotic signalling pathway [13]. FAS and FASL genes are found on 10q24.1 and 1q23 chromosomes, respectively [14]. The genes responsible for FAS and FASL encoding represented several functional polymorphisms affecting FAS and FASL expression levels. FAS-670A/G and FASL-844 C/T polymorphisms are the functional SNPs in the promoter region of these two genes [15]. FAS-670A/G polymorphism is caused by two events of A to G substitution at the position of -670 in the promoter region of FAS gene and disorder in binding site of Signal Transducer and Activator of Transcription 1 (STAT-1) [16]. These alterations can lead to a reduction in the promoter activity and as a result, a decreased expression level of the FAS gene. In addition, FASL-844C/T polymorphism at FASL gene promoter could affect the expression rate of this gene by T to C substitution [17]. FASL-844C/T variant occurs in a putative binding motif of a transcription factor (including CAAT/enhancer-binding protein β) which leads to alteration of its binding site. This polymorphism can lead to a higher basal expression level in FASL-844C allele carriers than FASL-844T [17]. Some studies have demonstrated a significant association between FAS-670A/G and FASL-844C/T polymorphisms with GC [18,19]. The present study was designed to investigate the association between these two functional polymorphisms in the promoter regions of FAS and FASL genes and their synergistic effects on GC risk in the Kurdish population in the west of Iran.
Material & methods
Study subjects: Ninety eight GC patients and 103 healthy controls with a mean age of 53 ± 6.43 and 47 ± 7.43 yr, respectively, were included in the present study. All patients and healthy individuals had a Kurdish ethnic background, and were recruited amongst the patients referred to the Imam Reza Hospital, Kermanshah University of Medical Sciences, Kermanshah, Iran from March 2018 to April 2019. All patients were selected amongst the population referred to the hospital by an oncologist for endoscopic procedure (due to the dyspeptic symptoms) and whole cancer cases of gastric adenocarcinoma (for post-operative histopathological diagnosis). Individuals with other ethnic backgrounds, incomplete clinical data and medical history of other disorders (such as diabetes and cardiovascular diseases) were excluded from the study. The control group with the same ethnic background, gender and age had no history of cancer. They were also visited to confirm the absence of cancer in Imam Reza Hospital during the same period. The study was approved by the Ethics Committee of Kermanshah University of Medical Sciences (Kermanshah, Iran). All participants were informed about the study’s objectives, and a written informed consent was also obtained.
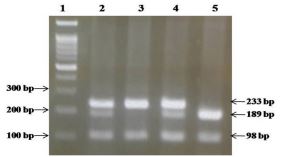
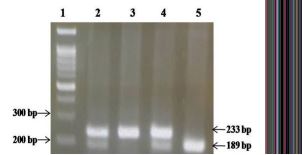
DNA extraction and genotyping: Genomic DNA was extracted from 3 ml peripheral blood from each of the samples using the standard phenol–chloroform extraction method. Purified genomic DNA was evaluated with a NanoDrop Spectrophotometer (wavelengths of 260 and 280 nm) and electrophoresis on one percent agarose gel. FAS and FASL polymorphisms were analyzed using Polymerase Chain Reaction-Restriction Fragment Length Polymorphism (PCR-RFLP) method (Figures 1 and 2). PCR was carried out for polymorphism amplification of FAS-670A/G and FASL-844C/T. The previously published primers used were 5-GGCTGTCCATGTTGTGGCTGC-3’ (forward) and 5-CTACCTAAGAGCTATCTACCGTTC-3’ (reverse) for FAS-670A/G variant [20] and 5-CAGCTACTCAGGAGGCCAAG-3’ (forward) and 5-GCTCTGAGGGGAGAGACCAT-3’ (reverse) for FASL-844C/T variant [21]. PCR and RFLP techniques were conducted according to the conditions mentioned in our previous study [22].
Statistical analysis
SPSS statistical software version 21.0 (IBM Corp., Armonk, NY, USA) was used. Genotype and allele frequencies of polymorphisms in both patient and healthy groups were analyzed using Pearson’s Chi-square test. Odds Ratios (ORs) were computed to determine the risk of GC with 95 per cent Confidence Intervals (CIs) for FAS-670A/G and FASL-844C/T polymorphisms in patient and control groups using logistic regression models. In this test, the GC and controls were the dependent index (Y variable), and also, different genotypes or alleles were independent variables (X variables). In all tests, P< 0.05 was considered as significant and the data were shown as the mean ± standard deviation
Results
Association of Fas Cell Surface Death Receptor (FAS) and Fas Ligand (FASL) variants with Gastric Cancer (GC) risk: The frequency of G and C alleles was found to be higher in patients as compared to the healthy controls. In FAS-670A/G polymorphisms, AA and GG genotype frequency was lower in patients than healthy controls. However, the frequency of AG genotypes was higher in patients compared to the control group (P=0.13). In addition, the results of FASL-844 C/T polymorphisms showed that the frequency of CT and TT genotypes was significantly lower in patients than the control group, while the frequency of CC genotypes was significantly higher in patients compared to the healthy controls (P=0.008). Analysis models of dominant and codominant in FASL polymorphism had a significant protective effect against GC incidence (P< 0.05) (Table 1). Moreover, the OR of CT, TT and CT+TT genotypes suggested that these genotypes may have protective effects against GC risk (P< 0.05) (Table 2).
Association of combined Fas cell surface death receptor and Fas ligand (FAS and FASL) genotypes with GC risk: The synergistic effects of FAS-670G and FASL-844T alleles on the risk of GC incidence were also analyzed. Based on our results, the presence of both FAS-670G and FASL-844T alleles in individuals suggested a significant protective effect against GC occurrence [OR=0.420, 95% CI (0.181-0.975), P=0.043]. In fact, a considerable interaction between FAS-670G and FASL-844T alleles in GC was observed (Table 3).
Discussion
Numerous complexes of molecular variations are involved in the pathogenesis of GC. Previous reports suggested that the FAS/FASL system could be promote the apoptotic cell death [13,23,24]. It has also been suggested that the alteration in FAS and FASL gene expression is associated with the risk of various cancers such as GC. Furthermore, in comparison with healthy individuals, the functional variants in these genes could potentially alter the expression levels of FAS and FASL genes by affecting the promoter activity and binding sites of transcription factors [16,17]. The results of the present study suggest that the FASL-844C/T polymorphism is significantly related to the risk of GC (P=0.008), while the association of FAS-670A/G polymorphism was found non-significant in patients with GC in comparison with healthy controls (P=0.13). In addition, our results showed that both FAS-670G and FASL-844T alleles had a significant protective role in GC development in the Kurdish population in the west of Iran (P=0.043) (Table III).
Table 1: Percent of Fas cell surface death receptor and Fas ligand genotype and allele frequencies in gastric cancer patients and healthy controls.
| Genotype/allele | Patient group (n=98) | Control group (n=103) |
|---|---|---|
| FAS-670A/G (genotypes) | ||
| AA (%) | 22 (22.4) | 31 (30.1) |
| AG (%) | 63 (64.3) | 52 (50.5) |
| GG (%) | 13 (13.3) | 20 (19.4) |
| χ2, df, P | 3.943, 2, 0.13 | |
| FAS-670A/G (alleles) | ||
| A (%) | 107 (54.6) | 114 (55.4) |
| G (%) | 89 (45.4) | 92 (44.6) |
| χ2, df, P | 0.000, 1, 1.00 | |
| FASL-844 C/T (genotypes) | ||
| CC (%) | 24 (24.5) | 9 (8.7) |
| CT (%) | 68 (69.4) | 83 (80.6) |
| TT (%) | 6 (6.1) | 11 (10.7) |
| χ2, df, P | 9.660, 2, 0.008 | |
| Dominant (CC vs. CT+TT) | 24 (24.5%) vs. 74 (75.5%) | 9 (8.7%) vs. 94 (91.3%) |
| χ2, df, P | 9.080, 1, 0.003 | |
| Co dominant CC versus CT | 24 (26.1%) vs. 68 (73.9%) | 9 (9.8 %) vs. 83 (90.2%) |
| χ2, df, P | 8.308, 1, 0.004 | |
| Co dominant CC versus TT | 24 (80.0%) vs. 6 (20.0%) | 9 (45.0%) vs. 11 (55.0%) |
| χ2, df, P | 6.551, 1, 0.010 | |
| FASL-844 C/T (alleles) | ||
| C (%) | 116 (59) | 101 (49) |
| T (%) | 80 (41) | 105 (51) |
| χ2, df, P | 2.013, 1, 0.156 | |
| FAS: Fas Cell Surface Death Receptor; FASL: Fas Ligand; Df: Degree Of Freedom | ||
Table 2: The odds ratios of Fas ligand-844 C/T genotypes and alleles with respect to CC genotype and C allele in the patient group.
| Patient group, OR (95% CI) | Control group |
|---|---|
| FASL-844 C/T | |
| CC=Reference group (n=24) CT=0.307 (0.134-0.705, P=0.005, n=68) TT=0.205 (0.058-0.718, P=0.013, n=6) CT+TT=0.295 (0.129-0.673, P=0.004, n=74) |
Reference group (n=9) (n=83) (n=11) (n=94) |
| CI: Confidence Interval; OR: Odds Ratio. | |
Table 3: Odds ratios interaction between Fas cell surface death receptor-670G and Fas ligand-844T alleles in the patient group.
| FAS-670 G | FASL-844 T | Control group, n (%) | Patient group, n (%) [OR (95% CI, P)] |
|---|---|---|---|
| − − + + |
− + − + |
9 (8.7%) reference group 22 (21.4%) 0 (0) 72 (69.9%) |
22 (22.4%) reference group 0 (0) 2 (2) 74 (75.6%), [OR=0.420, 95% CI (0.181-0.975, P=0.043)] |
| The simultaneous occurrence of different alleles of both studied mutations. | |||
Various investigations have so far been carried out to clarify the probable impacts of FAS-670A/G and FASL-844C/T polymorphisms on GC [18,25-27]. For example, Liu et al [27] in China proposed the FAS/FASL polymorphisms as a risk factor for GC incidence and introduced its multifactorial interactions with MMP-2 polymorphism as an effective impact on GC development. Similar to the present study, Li et al [25], in a meta-analysis investigation, demonstrated that FASL-844 T>C polymorphism could be associated with the risk of developing GC. In addition, another study reported that the FAS and FASL polymorphisms are crucial factors in the development of gastric atrophy and intestinal metaplasia in Helicobacter pylori-infected patients [19]. In this study, it was found that the FASL-844C allele considerably increased the risk of gastric atrophy development [19]. In another study by Wang et al [28], it was concluded that an increased level of FAS gene expression could improve the therapeutic outcomes in GC patients. However, in the study by Kupcinskas et al [29], no significant association was found amongst FAS-670A/G and FASL-844C/T polymorphisms with GC in the Caucasian population. In addition, it has been showed that the FAS‐670A/G genotype could reduce the risk of gastric cardiac carcinoma (GCA) in smokers. The A/G genotype among smokers were found to have a lower risk of GCA compared to A/A genotype. However, the FASL-844T/C variant was not associated with the risk of GCA development [18]. Thus, the previous studies and the data presented in the present investigation proposed that genetic variations in FAS/FASL system could play an essential role in the GC pathogenesis.
Some of the studies evaluated the association of FAS and FASL variants with various types of cancers (including prostate, breast, chronic myeloid leukaemia, oesophageal, head-and-neck and cervical cancers) [11,12,21,30,31]. These displayed a significant association between the alleles and genotypes of FAS and FASL with the risk of cancer. For example, Sun et al. [21] demonstrated that the genetic variants in FAS and FASL genes were associated with an increased risk of oesophageal squamous cell carcinoma in the Chinese population. Another study reported these to have increased the apoptosis rate of lymphocytes associated with the susceptibility of individuals to breast cancer [11]. Edathara et al [12] suggested a considerable association between FAS-670GG, FASL-844TC and CC genotypes with the risk of chronic myeloid leukaemia in the Indian population [12]. Various polymorphic variants have been reported in the field of GC with different results related to the sample size, techniques, heterogeneity of GC phenotype, ethnic differences and geographical variations. Phenotypic effects of gene variants are moderated by other genetic and environmental factors, which is a clear example of gene–environment interaction in specific phenotypic development. In present study, the data related to environmental risk factors (including family history, alcohol consumption, smoking, dietary and pathogenic infections) were not available for investigation of GC development and this was a limitation.
Overall, the authors believe the present study, for the first time, suggest that FASL-844C/T polymorphism and its synergistic effects with FAS gene could be significantly related to the GC risk in the Kurdish population in the west of Iran. Further case–control studies among different ethnicities are however, recommended to determine the accurate biological roles of these variations in cancer development.
Declarations
Financial support & sponsorship: This study received financial support from a grant (97278) from the Vice Chancellor for Research of Kermanshah University of Medical Sciences in Iran.
Conflicts of interest: The authors declare that they have no conflict of interest.
References
- Guo LL, Song CH, Wang P, Dai LP, Zhang JY, et al. Competing endogenous RNA networks and gastric cancer. World J Gastroenterol. 2015; 21: 11680-11687.
- Lichtenstein P, Holm NV, Verkasalo PK, Iliadou A, Kaprio J, Koskenvuo M, et al. Environmental and heritable factors in the causation of cancer-analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med. 2000; 343: 78-85.
- Nomura AM, Wilkens LR, Henderson BE, Epplein M, Kolonel LN, et al. The association of cigarette smoking with gastric cancer: The multiethnic cohort study. Cancer Causes Control. 2012; 23: 51-58.
- Duell EJ, Travier N, Lujan Barroso L, Clavel Chapelon F, Boutron Ruault MC, et al. Alcohol consumption and gastric cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC) cohort. Am J Clin Nutr. 2011; 94: 1266-1275.
- Sivachandran N, Dawson CW, Young LS, Liu FF, Middeldorp J, et al. Contributions of the Epstein-Barr virus EBNA1 protein to gastric carcinoma. J Virol. 2012; 86: 60-68.
- Yang CS. Vitamin nutrition and gastroesophageal cancer. J Nutr. 2000; 130: 338S-339S.
- Hashemi M, Fazaeli A, Ghavami S, Eskandari Nasab E, Arbabi F, Mashhadi MA, et al. Functional polymorphisms of FAS and FASL gene and risk of breast cancer – Pilot study of 134 cases. PLoS One. 2013; 8: e53075.
- Loreto C, La Rocca G, Anzalone R, Caltabiano R, Vespasiani G, Castorina S, et al. The role of intrinsic pathway in apoptosis activation and progression in Peyronie’s disease. Biomed Res Int. 2014; 2014: 616149.
- Itoh N, Yonehara S, Ishii A, Yonehara M, Mizushima S, Sameshima M, et al. The polypeptide encoded by the cDNA for human cell surface antigen Fas can mediate apoptosis. Cell. 1991; 66: 233-243.
- Oehm A, Behrmann I, Falk W, Pawlita M, Maier G, et al. Purification and molecular cloning of the APO-1 cell surface antigen, a member of the tumor necrosis factor/nerve growth factor receptor superfamily. Sequence identity with the Fas antigen. J Biol Chem. 1992; 267: 10709-10715.
- Zhang B, Sun T, Xue L, Han X, Zhang B, Lu N, et al. Functional polymorphisms in FAS and FASL contribute to increased apoptosis of tumor infiltration lymphocytes and risk of breast cancer. Carcinogenesis 2007; 28: 1067-1073.
- Edathara PM, Gorre M, Kagita S, Vuree S, Cingeetham A, Nanchari SR, et al. Association of promoter polymorphisms of Fas-FasL genes with development of Chronic myeloid leukemia. Tumour Biol. 2016; 37: 5475-5484.
- Nagata S. Fas ligand-induced apoptosis. Annu Rev Genet. 1999; 33: 29-55.
- Ji G, Gu A, Hu F, Wang S, Liang J, Xia Y, et al. Polymorphisms in cell death pathway genes are associated with altered sperm apoptosis and poor semen quality. Hum Reprod. 2009; 24: 2439-2446.
- Wang S, Wu S, Meng Q, Li X, Zhang J, Chen R, et al. FAS rs2234767 and rs1800682 polymorphisms jointly contributed to risk of colorectal cancer by affecting SP1/STAT1 complex recruitment to chromatin. Sci Rep. 2016; 6: 1-8.
- Sibley K, Rollinson S, Allan JM, Smith AG, Law GR, et al. Functional FAS promoter polymorphisms are associated with increased risk of acute myeloid leukemia. Cancer Res. 2003; 63: 4327-4330.
- Wu J, Metz C, Xu X, Abe R, Gibson AW, Edberg JC, et al. A novel polymorphic CAAT/enhancer-binding protein beta element in the FasL gene promoter alters Fas ligand expression: A candidate background gene in African American systemic lupus erythematosus patients. J Immunol. 2003; 170: 132-138.
- Zhou RM, Wang N, Chen ZF, Duan YN, Sun DL, Li Y. Polymorphisms in promoter region of FAS and FASL gene and risk of cardia gastric adenocarcinoma. J Gastroenterol Hepatol. 2010; 25: 555-561.
- Hsu PI, Lu PJ, Wang EM, Ger LP, Lo GH, Tsay FW, et al. Polymorphisms of death pathway genes FAS and FASL and risk of premalignant gastric lesions. Anticancer Res. 2008; 28: 97-103.
- Huang QR, Morris D, Manolios N. Identification and characterization of polymorphisms in the promoter region of the human Apo-1/Fas (CD95) gene. Mol Immunol. 1997; 34: 577-582.
- Sun T, Miao X, Zhang X, Tan W, Xiong P, et al. Polymorphisms of death pathway genes FAS and FASL in esophageal squamous-cell carcinoma. J Natl Cancer Inst. 2004; 96: 1030-1036.
- Asgari R, Mansouri K, Bakhtiari M, Bidmeshkipour A, Yari K, Shaveisi-Zadeh F, et al. Association of FAS-670A/G and FASL-844C/T polymorphisms with idiopathic azoospermia in Western Iran. Eur J Obstet Gynecol Reprod Biol. 2017; 218: 55-59.
- Waring P, Müllbacher A. Cell death induced by the Fas/Fas ligand pathway and its role in pathology. Immunol Cell Biol. 1999; 77: 312-317.
- Ohno S, Tachibana M, Shibakita M, Dhar DK, Yoshimura H, Kinugasa S, et al. Prognostic significance of Fas and Fas ligand system-associated apoptosis in gastric cancer. Ann Surg Oncol. 2000; 7: 750-757.
- Li J, Cen H, Pan HF, Yin Y. Association between the FAS/FASL polymorphisms and gastric cancer risk: A meta-analysis. Asian Pac J Cancer Prev. 2012; 13: 945-951.
- Zhang W, Li C, Wang J, He C. Functional polymorphisms in FAS/FASL system contribute to the risk of occurrence but not progression of gastric cardiac adenocarcinoma. Hepatogastroenterology. 2012; 59: 141-146.
- Liu L, Wu C, Wang Y, Zhong R, Wang F, Zhang X, et al. Association of candidate genetic variations with gastric cardia adenocarcinoma in Chinese population: A multiple interaction analysis. Carcinogenesis. 2011; 32: 336-342.
- Wang X, Fu Z, Chen Y, Liu L. Fas expression is downregulated in gastric cancer. Mol Med Rep. 2017; 15: 627-634.
- Kupcinskas J, Wex T, Bornschein J, Selgrad M, Leja M, Juozaityte E, et al. Lack of association between gene polymorphisms of angiotensin converting enzyme, Nod-like receptor 1, Toll-like receptor 4, FAS/FASL and the presence of Helicobacter pylori-induced premalignant gastric lesions and gastric cancer in Caucasians. BMC Med Genet. 2011; 12: 112.
- Zhang Z, Wang LE, Sturgis EM, El-Naggar AK, Hong WK, et al. Polymorphisms of FAS and FAS ligand genes involved in the death pathway and risk and progression of squamous cell carcinoma of the head and neck. Clin Cancer Res. 2006; 12: 5596-5602.
- Sun T, Zhou Y, Li H, Han X, Shi Y, et al. FASL–844C polymorphism is associated with increased activation-induced T cell death and risk of cervical cancer. J Exp Med. 2005; 202: 967-974.