
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Extensive cranial langerhans cell histiocytosis
revealed by acute mastoiditis
Khadija El Bouhmadi*; Myriam Loudghiri; Youssef Oukessou; Sami Rouadi; Redallah Abada; Mohamed Roubal; Mohamed Mahtar
Otorhinolaryngology and Head and Neck surgery Department, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
*Corresponding Author : Khadija El Bouhmadi
Otorhinolaryngology and Head and Neck surgery Department, Ibn Rochd University Hospital, Faculty of Medicine and Pharmacy, Hassan II University, Casablanca, Morocco.
Tel: +212 662 53 10 11;
Email: elbkhadija25@gmail.com
Received : Aug 09, 2022
Accepted : Sep 01, 2022
Published : Sep 08, 2022
Archived : www.jcimcr.org
Copyright : © El Bouhmadi K (2022).
Citation: El Bouhmadi K, Loudghiri M, Oukessou Y, Rouadi S, Abada R, et al. Extensive cranial langerhans cell histiocytosis revealed by acute mastoiditis. J Clin Images Med Case Rep. 2022; 3(9): 2039.
Clinical image description
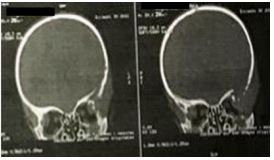
Langerhans cell histiocytosis is a group of diseases characterized by an inflammatory neoplasia of myeloid precursor cells driven by mutations in the mitogen-activated protein kinase pathway leading to the proliferation and accumulation of Langerhans cells [1,2]. Clinical manifestations range from isolated disease to multifocal lesions and systemic involvement with a worse prognosis [2,3]. The otologic features are rare and may include otorrhea, otalgia, subjective hearing loss and vertigo misleading the diagnosis to an inflammatory process [3]. The CT scan shows destruction of the skull with characteristic “punched out” lytic lesions that can be multiple and multifocal. Tissue biopsy confirms the diagnosis [3].
We report the case of a 4 years old boy who presented to the E.R with a 2-week left-sided otalgia and otorrhea without any improvement under local antibiotics, associated to superficial temporal tenderness. The physical examination revealed an acute otitis media, with an inflammatory swelling in the mastoid area with no facial palsy or pain. The CT scan showed destructive “punched out” lytic bilateral lesions of the temporal bones with signs of mastoiditis and significant soft tissue thickening in the left side, associated to multiple lytic lesions in the Diploë with destruction of the cortical outer layer of the skull vault, suggesting an extensive cranial Langerhans cell histiocytosis. The diagnosis was confirmed by histology. Regarding the extensive nature of the disease process, the patient was referred to haematology for further treatment.

References
- Leung AKC, Lam JM, Leong KF. Childhood Langerhans cell histiocytosis: A disease with many faces. World J Pediatr. 2019; 15: 536-545.
- Krooks J, Minkov M, Weatherall AG. Langerhans cell histiocytosis in children: History, classification, pathobiology, clinical manifestations, and prognosis. J Am AcadDermatol. 2018; 78: 1035-1044.
- Darr A, Mughal Z, Martin T. A rare case of extensive cranial Langerhans cell histiocytosis, synchronously presenting as otitis externa and giant cell arteritis. J Surg Case Rep. 2016; 2016: rjw094.