
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Awareness of sick day rules and use of steroid cards among patients taking long term synthetic oral glucocorticoids for immunosuppression and adrenal hormone replacement at a tertiary hospital in Ethiopia: A cross-sectional study
Rediet Ambachew*; Yared N Demssie; Theodros Aberra; Getahun Tarekegn; Tedla Kebede
Department of Endocrinology, Addis Ababa University, College of Health Sciences, Addis Ababa, Ethiopia
*Corresponding Author : Rediet Ambachew
Department of Endocrinology, Addis Ababa University, College of Health Sciences, Addis Ababa, Ethiopia.
Email: redixnew21@yahoo.com
Received : Aug 10, 2022
Accepted : Sep 01, 2022
Published : Sep 08, 2022
Archived : www.jcimcr.org
Copyright : © Ambachew R (2022).
Abstract
Background: Glucocorticoids are among the most commonly prescribed medications owing to their generic anti-inflammatory and immunosuppressive effects. Adrenal insufficiency and adrenal crisis are among the major serious adverse effects of long course glucocorticoid treatment. Patient education on sick day rules and the use of steroid treatment identifiers are some of the strategies that are commonly employed to mitigate the risk of AI and adrenal crisis. This study aimed to assess awareness of sick day rules and the use of steroid cards at a tertiary referral hospital in Ethiopia.
Methods: A cross-sectional study was conducted at the outpatient medical clinics at Tikur Anbessa Specialized Hospital over a study period of consecutive six months. A total of 100 patients from medical and endocrine clinics who fulfilled the eligibility criteria were recruited to take part in the study on the day they attended their routine follow-up clinics. Interviewer administered questioner regarding sick day rules and use of steroid identifier was used and statistical analysis was done using SPSS software version 20.
Results: The mean age of the participants was 42 years and 72% were females. Only 27% of the study participants were aware of the need to make changes on their steroid dose in the event of acute illness or injury. Endocrine patients showed a better awareness of steroid sick day rules [15/35, 42%] as compared to medical patients [12/65, 18.4%], P-value < 0.05. Among the total participants only 2 endocrine patients carried a steroid card.
Conclusion and recommendations: The data highlights that awareness of sick day rules and the provision of steroid use identifiers is very low among both endocrine and medical patients receiving GC treatment. Urgent intervention to address this gap in clinical practice is needed to mitigate serious adverse effects such as AI and Adrenal crisis.
Citation: Ambachew R, Demssie YN, Aberra T, Tarekegn G, Kebede T, et al. Awareness of sick day rules and use of steroid cards among patients taking long term synthetic oral glucocorticoids for immunosuppression and adrenal hormone replacement at a tertiary hospital in Ethiopia: A cross-sectional study. J Clin Images Med Case Rep. 2022; 3(9): 2040.
Introduction
The discovery of the anti-inflammatory and immunosuppressive properties of Glucocorticoids (GCs) in the 1950s has been a major game-changer in the fight against autoimmune and inflammatory disorders. Since then, GCs have become one of the most commonly prescribed medications in clinical practice [1].
The chronic use of GCs is associated with many adverse effects. One of the most commonly encountered adverse effects is suppression of the Hypothalamic-Pituitary-Adrenal (HPA) axis which could culminate in Adrenal Insufficiency (AI) and life-threatening adrenal crisis under certain circumstances [2,3].
Observational studies have revealed AI prevalence as high as 14-63% among patients taking long-term GC treatment [4-6]. AI was demonstrated in GC treatment dose equivalent to < 5 mg/day of prednisolone and duration of treatment as short as 4 weeks. Moreover, studies indicate that about one-third of patients who take GC develop AI upon tapering treatment dose and 15% of patients display evidence of persisting AI up to 3 years after cessation of GC treatment [7-9]. Hence, patients who receive long course GC treatment would need appropriate follow-up and screening for clinical and/or biochemical evidence of AI.
Patient education on sick day rules, the use of steroid treatment identifiers such as steroid cards, and the provision of rescue parenteral glucocorticoid kit are some of the strategies that are commonly employed to mitigate the risk of AI and adrenal crisis [10-12].
However, studies indicate a significant gap in patient knowledge and awareness of these life-saving measures. Anecdotal evidence paints a grim picture of the existing practice in a resource-limited setup such as ours due to poor supervision of glucocorticoid treatment, the availability of over-the-counter products, and a low level of awareness among patients and health care professional alike.
In this study, we looked at the awareness of sick day rules and the use of steroid cards among patients taking synthetic oral glucocorticoids for immunosuppression and adrenal hormone replacement at a tertiary hospital in Ethiopia. We also checked the use of bone protective treatment with bisphosphonates for patients who are treated with long-term GCs.
Methods
A cross-sectional study was conducted to determine the awareness of sick day rules and use of steroid cards among patients taking synthetic oral glucocorticoids for immunosuppression and adrenal hormone replacement at a tertiary hospital in Ethiopia.
Participants and settings
The study was conducted at Tikur Anbessa Specialized Hospital [TASH], which is located in Addis Ababa, the capital city of Ethiopia. It is a national referral hospital and medical training center with different specialized outpatient clinics and over 700 beds. The study was done from July, 1 - December 30, 2020, for 6 consecutive months.
One hundred patients who fulfilled the eligibility criteria (those taking oral glucocorticoids at a dose equivalent to prednisolone 5 mg per day or more for duration of greater than 1 month) were included in the study. Sixty-five patients were enrolled from the outpatient medical clinics [Nephrology, Rheumatology, Respiratory and Neurology] and thirty-five patients from the endocrine clinic.
Data obtained using a well-structured questionnaire designed and pre-tested to assess knowledge of sick day rules and the use of steroid identifiers for patients on long-term steroids. (See Appendix 1).
Statistical analysis
The result was analyzed and reported as proportions for each item in the questioner and a comparison between the groups was made using the chi-square test and the difference was considered statistically significant at p < 0.05. SPSS statistical software version 20 was used.
Ethical considerations
We obtained approval of the research proposal from the ethical review committee of the department of internal medicine, college of health sciences, Addis Ababa University. Informed consent was obtained from each respondent to participate in the study.
Operational definitions
● Acute adrenal insufficiency [adrenal crisis]: Is a life-threatening endocrine emergency due to deficiency of the adrenal hormone cortisol, the major glucocorticoid based on the clinical diagnosis made by the health care provider [13].
● Sick day rule:
- The need to double daily oral glucocorticoid dose during intercurrent illness or injury that requires bed rest and/or antibiotics [13].
- The need to administer parenteral glucocorticoids in the event of vomiting and diarrheal illness, medical procedures such as endoscopy, acute trauma, and surgical procedures requiring general anesthesia [13].
● Steroid use identifier: Use of steroid card, medical alert bracelets, or any other form of steroid use identifier that has to be carried by patients on long term GCs at all times so that health care professionals and emergency caregivers have this vital piece of information when they make treatment decisions [13].
● Long term steroid use: duration of steroid use for >1 month [14].
Results
Characteristics of patients on the study
A total of 100 patients from medical and endocrine clinics who fulfilled the eligibility criteria were included in the study. The mean age of the participants was 42 years, ranging from 13 to 81 years and 72% of them were female. More than half of the patients have completed a minimum of secondary School i.e.
Table 1: Characteristics of patients on the study.
| Characteristics | N | Percentage | |
|---|---|---|---|
| Sex | Male | 28 | 28 |
| Female | 72 | 72 | |
| Educational level | None | 16 | 16.0 |
| Primary | 27 | 27.0 | |
| Secondary | 39 | 39.0 | |
| College and university | 18 | 18.0 | |
| Place of follow up | Medical | 65 | 65 |
| Endocrine | 35 | 35 | |
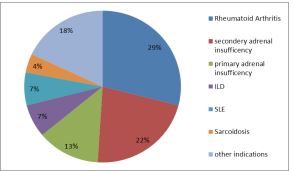
From the participants, 65% were from Internal medicine outpatient clinic with the most common indication for steroid initiation being rheumatoid arthritis followed by Systemic lupus erythematous and interstitial lung disease while 35 % were from the endocrine clinic with secondary adrenal insufficiency being the major indication followed by primary adrenal insufficiency (Figure 1).
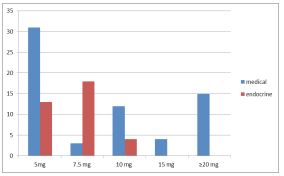
Prednisolone was used by all of the participants. The dose used by the participants during the study period ranged from 5 - 50 mg, the mean dose being 10 mg of prednisolone per day. Among the endocrine patient, 88% received 5 to 7.5 mg replacement dose while medical patients required relatively higher dose where 49 % of them were requiring ≥ 10 mg per day (Figure 2).
Awareness of sick day rules and usage of steroid card
From the study participants, only 27% were aware of the need to increase their steroid dose in the event of acute illness or injury. Endocrine patients exhibited better steroid use awareness [15 out of 35, 42%] than patients in the medical group [12 out of 65, 18.4%], P-value < 0.05.
Educational level and respondents’ steroid awareness were significantly correlated in this study (p=0.039). Those patients who had college-level educational background were 2.6 times more aware of sick day rules than other respondents [COR: 2.551, 95%CI (1.004-6.289)].
Verbal or written information regarding steroid sick day rules was given only to 21% of the participants. Thirteen out of thirty-five endocrine patients [37.1%] received verbal or written information regarding steroid sick day rules as compared to only eight out of sixty-five medical patients [12.3%], P-value < 0.05.
Only 15% of the participants knew what to do if they develop a vomiting illness and unable to take their oral steroid tablets. Eight [22.8%] of endocrine and seven [10.7%] of medical patients knew what to do if they develop a vomiting illness and unable to take their oral steroid tablets [P value 0.143].
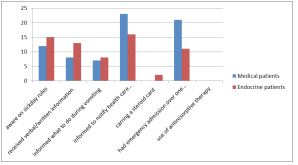
In the study, 39% of the participants were informed of the need to notify health care professionals that they are taking steroid medication. Sixteen [45.7%] of endocrine and twenty-three [35.3%] of medical patients were informed of the need to notify health care professionals [P value 0.391].
Among the total participants, only 2 endocrine patients carried a steroid identifier card of long-term steroid use.
From the thirty-two participants that required emergency hospital admission over the preceding year, 43.7% had steroid dose amendment while in the hospital and 31.2% received instruction on sick day rules upon discharge.
None of the study participants were given antiresorptive therapy like bisphosphonates.
Discussion
Adrenal insufficiency has been recognized as a potential life-threatening side effect of glucocorticoid therapy since its discovery in the 1950s. Glucocorticoid-induced adrenal crisis can be preventable but unfortunately continues to be a major cause of morbidity and mortality.
Patient education on sick day rules, the use of steroid treatment identifiers such as steroid cards, and the provision of rescue parenteral glucocorticoid kit are some of the strategies that are commonly employed to mitigate the risk of AI and adrenal crisis [10-12]. However, there are significant gaps in knowledge and awareness of sick day rules and the use of steroid cards among patients taking long-term steroid therapy.
Studies conducted in high-income countries have revealed that adherence to these preventative strategies is unsatisfactory, thereby predisposing patients to life-threatening adrenal crises [15,16].
Lack of similar data from low-income countries is a major drawback to the successful implementation of effective preventative strategies. Our study tried to assess the awareness of sick day rules and use of steroid cards among patients taking synthetic oral glucocorticoids for immunosuppression and adrenal hormone replacement at a tertiary hospital in Ethiopia.
Our data demonstrated that the majority of the patients taking steroids are unaware of these basic preventative measures that they need to implement in the event of intercurrent illness.
One of the factors associated with this can be poor educational background, which was seen from our study where those who attended higher education were 2.6 times more aware of sick day rules than the other respondents.
Awareness of sick day rules is particularly lower in patients taking GCs for immunosuppressive indications compared to those taking them for adrenal hormone replacement therapy [P < 0.05]; similar results were seen in a recent study conducted in the United Kingdom where endocrine patients had better awareness as compared to patients taking glucocorticoids for miscellaneous causes [17]. In this study, endocrine patients doubled their steroid dose during inter current illness (89 v/s 23%), obtained parenteral steroid during vomiting (83 v/s 27%), and carried a steroid card (82 v/s 21%), p < 0.001 for all comparisons [17].
GC-induced osteoporosis is the most common form of secondary osteoporosis and the first leading cause in young people. Bone loss and increased rate of fractures occur early after the initiation of GC therapy and are then related to dosage and treatment duration [18].
A meta-analysis of over 80 studies in adults found that use of ≥5 mg/day of prednisolone (or equivalent) was associated with significant reductions in Bone Mineral Density (BMD) and an increase in fracture risk within 3 to 6 months of treatment initiation; this increased fracture risk was independent of patient age, gender and the underlying disease [19].
Most guidelines and evidence support the use of bisphosphonates as first-line therapy for the prevention and treatment of GC-induced osteoporosis in adults. However, across the 100 GC-exposed patients included in our study, none were started on antiresorptive therapy for the prevention of osteoporosis.
The other finding of significant concern from this study is the poor use of steroid cards, demonstrated by only 2 of the 100 participants taking any form of an identifier of prolonged steroid use.
Patient education alone would not be successful to address the problem unless it is coupled with appropriate education and engagement of Health Care Professionals (HCPS).
A study conducted in the United Kingdom revealed that HCPs had poor knowledge of when to issue ‘steroid cards’, did not give advice about ‘sick day’ rules, and over a tenth failed to recommend increasing steroids at times of stress [20]. This is of great concern as HCPs are expected to be the primary source of information for patients taking steroid therapy.
Therefore, appropriate education of HCPs about the importance of implementing basic strategies to mitigate the risk of AI associated with steroid therapy is of paramount importance.
Conclusion and recommendation
The awareness of sick day rules and practice of steroid use identifiers is very low both in medical and endocrine patients under follow-up in TASH as seen in this study. Our study highlights the urgent need for developing locally applicable patient information resources on steroid therapy and sick day rules as well as the provision of steroid use identifiers.
We recommend formal education of patients on the risks associated with the use of GCs at the point of initiation of treatment, with particular emphasis on sick day rules and the need for keeping steroid use identifiers such as steroid cards.
HCPs should provide the necessary education about the risk of AI associated with GC use as well as providing patients with appropriate patient information leaflets and steroid use identifiers. A national guideline for HCPs on the appropriate implementation of sick day rules would also help to address the risk of AI associated with GC use.
Acknowledgement
We want to thank the patients and the hospital staff who collaborated in the study period.
References
- Fardet L, Petersen I, Nazareth I. Prevalence of long-term oral glucocorticoid prescriptions in the UK over the past 20years. Rheumatology (Oxford). 2011; 50: 1982–1990. http://dx.doi.org/10.1093/rheumatology/ker01
- Paragliola RM, Papi G, Ponteocorvi A, et al. Treatment with synthetic glucocorticoids and the Hypothalamus-Pituitary-Adrenal axis. Int J of Mol Sci. 2017; 18: 2001.
- Dinsen S, Baslund B, Klose M, et al. Why glucocorticoid withdrawal may sometimes be as dangerous as the treatment itself. Eur J Intern Med. 2013; 24: 714–720. http://dx.doi.org/10.1016/ j.ejim.2013.05.014
- Sacre K, Dehoux M, Chauveheid MP, et al. Pituitary–adrenal function after prolonged glucocorticoid therapy for systemic inflammatory disorders: An observational study. J Clin Endocrinol Metab. 2013; 98: 3199–3205. http://dx.doi.org/10.1210/jc.2013–1394
- Schlaghecke R, Kornely E, Santen RT, et al. The effect of long-term glucocorticoid therapy on pituitary–adrenal responses to exogenous corticotropin-releasing hormone. N Engl J Med. 1992; 326: 226–230. http://dx. doi.org/10.1056/NEJM199201233260403
- Jamilloux Y, Liozon E, Pugnet G, et al. Recovery of adrenal function after long-term glucocorticoid therapy for giant cell arteritis: A cohort study. PLoS One. 2013; 8: e68713. http://dx.doi.org/ 10.1371/journal.pone.0068713
- Joseph RM, Hunter AM, Ray DW, et al. Systemic glucocorticoid therapy and adrenal insufficiency in adults: A systematic review: Semin Arthritis and Rheu. 46: 133–141.
- Miro J, Amado JA, Pesquera C, et al. Assessment of the hypothalamic–pituitary–adrenal axis function after corticosteroid therapy for MS relapses. Acta Neurol Scand. 1990; 81: 524–528.
- Boots JM, vanden Ham EC, Christiaans MH, et al. Risk of adrenal insufficiency with steroid maintenance therapy in renal transplantation. Transplant Proc. 2002; 34: 1696–1697
- Hahner S, Loeffler M, Bleicken B, et al. Epidemiology of adrenal crisis in chronic adrenal insufficiency: the need for new preventative strategies. Eur J Endocrinol. 2010; 162: 597- 602.
- Peacey SR, Pope RM, Naik KS et al. Corticosteroid therapy and intercurrent illness: The need for continuing education. Postgrad Med J. 1993; 69: 282-284
- Quinkler M & Hahner S. What is the best long-term strategy for patients with primary adrenal insufficiency? Clin Endocrinol. 2012; 76: 21–25.
- Society for Endocrinology Endocrine Emergency Guidance: Emergency Management of Acute Adrenal Insufficiency (Adrenal Crisis) In Adult Patients, Royal College of Physicians. 2017.
- Lewis Mundell, Roberta Lindemann, Douglas. Monitoring long-term oral corticosteroids. BMJ Quality Improvement Report.
- Puar TH, Stikkelbroeck NM, Smans LC, et al. Adrenal Crisis: Still a Deadly Event in the 21st Century. Am J Med. 2016; 129: 339.e1-9.
- Smans LC, VanderValk ES, Hermus AR, et al. Incidence of adrenal crisis in patients with adrenal insufficiency. Clin Endocrinol (Oxf). 2016; 84: 17–22. http://dx.doi.org/10.1111/cen.12865.
- Salehmohamed MR, Griffin M, Branigan T, et al. Patients treated with immunosuppressive steroids are less aware of sick day rules than those on endocrine replacement therapy and may be at greater risk of adrenal crisis. Ir J Med Sci. 2018; 187: 69-74.
- Briot K, Roux C. Glucocorticoid-induced osteoporosis. RMD Open. 2015; 1: e000014.
- Van Staa TP, Leufkens HG, Cooper C. The epidemiology of corticosteroid-induced osteoporosis: A meta-analysis. Osteoporos Int. 2002; 13: 777-787.
- Grounds K, Khan I, Adlan M, Premawardhana L. Poor knowledge of safety aspects of long-term steroid use among patients and healthcare professionals. Clin Med (Lond). 2017; 17: 378-380.
Annex 1
Awareness to increase steroid medication in the event of an acute illness/injury? Yes/No
Received verbal or written information regarding sick day rules? Yes/No
Informed what to do in the event of vomiting illness and unable to take the steroid medication? Yes/No
Informed to notify health care professionals that you are taking steroid medications? Yes/No
Do you carry a steroid card or any other form of an identifier of long-term steroid use? Yes/No
Do you carry a steroid card or any other form of an identifier of long-term steroid use? Yes/No
If yes, has there been any change to the steroid medication dose? Yes/No
Have you received any verbal or written instruction regarding the steroid medication before discharge? Yes/No
Have you received antiresorptive therapy? Yes/No