
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Association of aspirin therapy with prognosis in patients with non obstructive coronary artery disease: A systematic review and meta-analysis
Hua-Ping Fan1; Shuai Mao2; Yu Zhou1; Jun Jin3*; Quan-You Zheng4*
1Department of Cardiology, 63650 Military Hospital, Urumqi 841700, China.
2Department of Cardiology, PLA Strategic Support Force Characteristic Medical Center, Beijing 100101, China.
3Institute of Cardiovascular Diseases, Xinqiao Hospital, Army Medical University, Chongqing 400038, China.
4Department of Nephrology and Urology, The 958th Hospital, The First Affiliated Hospital, Army Medical University, Chongqing 400020, China.
*Corresponding Author : Jun Jin
Institute of Cardiovascular Diseases, Xinqiao Hospital, Army Medical University, 83 Gaotanyan Road, Shapingba District, Chongqing 400038, China.
Phone: +86 023 68755601;
Email: jjxqyy011@163.com
Quan-you Zheng
Department of Nephrology and Urology, The 958th Hospital, The First Affiliated Hospital, Army Medical University, 29 Jianxing Dong Road, Jiangbei District, Chongqing 400020, China.
Phone: +86 023 68762177;
Email: zhengqy1205@126.com
Received : Aug 09, 2022
Accepted : Sep 02, 2022
Published : Sep 09, 2022
Archived : www.jcimcr.org
Copyright : © Jin J, Zheng QY (2022).
Abstract
Background: The effect of aspirin therapy in patients with nonobstructive Coronary Artery Disease (CAD) remains controversial. This study aimed to investigate the association between aspirin therapy and prognosis in nonobstructive CAD.
Methods: We searched for observational cohort studies on Pubmed, Embase, the Cochrane Library and Web of Science. Studies were included that compared the endpoint differences in patients with nonobstructive CAD who were treated with aspirin or not. The primary endpoint was a composite of Major Adverse Cardiovascular Events (MACEs). Secondary endpoints included all-cause death, cardiovascular death and Myocardial Infarction (MI). The pooled effect size was estimated as Hazard Ratio (HR) with 95% Confidence Interval (CI), which was measured by a random effect model using the generic inverse variance method.
Results: Thirteen published studies with 34,463 patients were included Pooled data showed that aspirin therapy was not associated with the risk of MACEs (HR 1.10; 95% CI 0.85–1.41; P=0.47, I2=57%). Similar results were observed in cardiovascular death (HR 1.12; 95% CI 0.73–1.73; P=0.60, I2=0%) and MI (HR 0.53; 95% CI 0.09–3.20; P=0.49, I2=68%), except all-cause death (HR 0.77; 95% CI 0.63–0.95; P=0.02, I2=25%). Subgroup analyses showed that there were no associations between aspirin therapy and MACEs in all subsets.
Conclusions: Routine aspirin therapy might not be associated with a decreased risk of cardiovascular events in patients with nonobstructive CAD. Aspirin therapy in non-obstructive CAD should be better investigated and future research is needed. A personalized antiplatelet regimen may contribute to reduction in ischemic cardiovascular events for these patients.
Registration: PROSPERO (CRD42021281706).
Keywords: Coronary artery disease; Nonobstructive; Antiplatelet; Aspirin; Prognosis.
Abbreviations: CAD: Coronary Artery Disease; Maces: Major Adverse Cardiovascular Events; MI: Myocardial Infarction; HR: Hazard Ratio; CI: Confidence Interval; CAS: Coronary Artery Spasm; NOS: Newcastle–Ottawa Scale; ACS: Acute Coronary Syndrome; DAPT: Dual Antiplatelet Therapy; CV: Cardiovascular; NR: Not Reported.
Citation: Hua-Ping F, Mao S, Zhou Y, Jin L, Quan-You Z. Association of aspirin therapy with prognosis in patients with non obstructive coronary artery disease: A systematic review and meta-analysis. J Clin Images Med Case Rep. 2022; 3(9): 2042.
Background
Non obstructive Coronary Artery Disease (CAD) is characterized by symptoms of suspected myocardial ischemia with stenosis of < 50% on angiography [1]. Non obstructive CAD accounts for 67% of patients with stable angina and 13% of patients with non-ST-segment elevation acute coronary syndrome [2]. Non obstructive CAD, a heterogeneous disease with limited atherosclerosis, is closely related to multiple conditions, including vulnerable plaque, thrombus, Coronary Artery Spasm (CAS), microvascular dysfunction, myocarditis, and cardiomyopathy [1,3]. The prognosis of patients with nonobstructive CAD varies substantially depending on their underlying causes [4,5]. Overall, accumulating evidence reveals that the presence of non obstructive CAD contributes to higher risks of mortality, Myocardial Infarction (MI), and re-hospitalization for angina [6,7].
Currently, the detection of non obstructive CAD increases the prescription of cardiovascular preventive medical therapies, including aspirin [8,9]. Aspirin, a cornerstone agent, significantly reduces the risk of ischemic events in patients with obstructive CAD [10]. However, the prognosis of aspirin therapy in patients with non obstructive CAD remains controversial, and there are no randomized controlled trials or systematic reviews regarding this topic. Hwang et al. reported that aspirin therapy was associated with a decreased risk of all-cause death, but with no effect on cardiovascular events [11], whereas another study found that aspirin failed to reduce the risk of all-cause death or cardiovascular events [12]. Furthermore, a few studies with smaller sample sizes lack adequately statistical power to determine the effect of aspirin on the outcomes of non obstructive CAD [13-15].
Given these uncertainties, we aimed to clarify the efficacy and safety of aspirin therapy in patients with non obstructive CAD through a systematic review and meta-analysis of observational studies.
Methods
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. The protocol for this study was revised on October 30, 2021, and November 10, 2021; the search words were amended, and additional statistical analyses were performed according to the Cochrane handbook suggestions [17]. The protocol was registered on PROSPERO (registration number: CRD42021281706).
Inclusion and exclusion criteria
Patients with suspected myocardial ischemia with < 50% coronary stenosis on angiography were included in the study. The intervention and control groups included patients who received aspirin therapy and those who did not, respectively. Hazardratios (HRs) of endpoints were the outcome indicators. We included prospective and retrospective cohort studies. Studies were excluded as per the following criteria: (1) reviews, (2) duplicate reports, (3) prior revascularization, (4) case reports, and (5) detailed antiplatelet regimens unavailable.
Data sources
We searched Pubmed, Embase, the Cochrane Central RegRegister of Controlled Trials, and Web of Science core collection (from 1985 to January 3, 2022) without language limitations. The detailed search strategies for each database are shown in Supplementary Table S1. The references of relevant reviews and included studies were manually searched.
Study selection and data extraction
We screened the title and abstracts and identified potentially eligible studies. Of these, the included studies were identified after reading the full texts. The reasons for exclusion were recorded in detail. The following data were extracted from the included studies: Information about first author name, study name, publication year, location, study design, demographics and baseline characteristics, pathophysiological mechanisms, antiplatelet strategies, sample size, follow-up duration, cardiovascular events, titles, and notable labels. If propensitys core-matched data or adjusted data were available, these were preferentially extracted because outcomes might be masked or overstated by these confounding factors. Two investigators independently conducted the above processes, and the discrepancies were resolved through discussion with a third investigator.
Endpoint definition
The primary endpoint was defined as a composite of Major Adverse Cardiovascular Events (MACEs), including all-cause or cardiovascular death, MI, and hospitalization for angina, heart failure, or stroke. The secondary endpoints included all-cause death, cardiovascular death and MI. The safety endpoint was bleeding risk, as defined in the original study.
Individual study quality assessment and publication bias
Two authors independently assessed the bias risk of each study using the Newcastle–Ottawa Scale (NOS) [18], which includes three aspects: Population selection, comparability and outcome assessment. Semi-quantification of NOS was assessed using the following scores: Low, 0–3; medium, 4–6; high quality, 7–9. Publication bias was visually described using funnel plots and quantitatively analyzed by Egger’s tests when more than 10 studies were included. Statistical significance was set at a P-value of < 0.05.
Statistical analysis
The pooled effect size with the 95% Confidence Interval (CI) was analyzed using Rev Man (version 5.3; Nordic Cochrane Center, Cochrane Collaboration). The variability of effect size among studies was assessed using the I² statistical magnitude and P-value for heterogeneity. I2 of >50% or P-value of < 0.05 indicated wide heterogeneity [19]. Heterogeneity was inevitable because of the variations in sample size, follow-up duration, baseline MI, and pathophysiological mechanisms. Therefore, pooled HR was measured with a random effect model utilizing the generic inverse variance method. Sensitivity analysis was conducted by excluding individual studies to explore the sources of heterogeneity. In addition, predefined subgroup analyses were performed based on study design (prospective vs. retrospective), follow-up duration (>36 months vs. ≤36 months), baseline MI (positive vs. negative), CAS (definite vs. indefinite), sample size (≤600 vs.>600) and adjustment (yes vs.no). Statistical significance wa s set at a P-value of < 0.05.
Results
Study selection and baseline characteristics
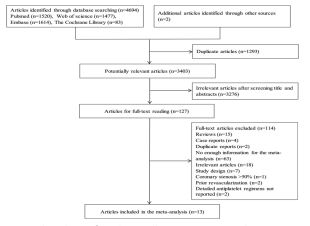
A total of 4694 studies were identified from the four databases, and two additional studies were selected by manually searching the references (Figure 1). Thirteen published studies [11-15,20-27] with 34,463 patients were enrolled in our meta-analysis. The median follow-up duration was 36 months (range, 12–98 months). A history of baseline MI was reported in five studies [13,22-24,27], and a potential pathophysiological mechanism associated with CAS was published in four studies [14,15, 21,22]. The prescription rate of aspirin in these studies ranged from 29.0% to 90.1% (Table 1).
Quality assessment of individual study
The NOS score of one study [22] was five, indicating medium quality, and all the other studies were of high quality. Another study [12] recruited participants with diabetes mellitusonly, which might contribute to bias risk regarding representativeness of the population (Table 2).
Table 1: Baseline characteristics of the included studies.
| Source | Study design | Total | Age (years) | Male (%) | Mechanisms | Baseline MI | Coronary stenosis | Antiplatelet strategy (%) | Statin (%) | Follow-up (months) | Outcomes | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aspirin | DAPT | |||||||||||
| Vicente-Ibarra[35] 2021 (Spain) | Retrospective | 120 | 59 | 64.2 | Indefinite | Positive | < 50% | 60.0 | 18.3 | 59.2 | 35 | All-cause death, MI, stroke, hospitalization for CV causes |
| Olesen 2021[20](Denmark) | Retrospective | 4124 | 60 | 50.3 | Indefinite | Negative | < 50% | 60.0 | NR | 70.7 | 59 | All-cause and CV death, MI, stroke, bleeding risk |
| Gu 2021[33] (China) | Retrospective | 757 | 53 | 61.2 | Indefinite | Negative | 1%–49% | 44.4 | NR | 46.1 | 59 | CV death, ACS, revascularization |
| Ciliberti 2021[32] (Italy) | Retrospective | 621 | 65 | 44.6 | Indefinite | Positive | < 50% | 87.9 | 58.8 | 81.0 | 90 | All-cause death, ACS, hospitalization for heart failure, stroke |
| Paolisso 2020[21] (Italy) | Prospective | 88 | 67 | 37.5 | Indefinite | Positive | < 50% | 85.2 | 56.8 | 75.0 | 19 | All-cause death, MI, stroke |
| Lee 2018[22](South Korea) | Retrospective | 154 | 51 | 74.7 | Definite | Negative | < 50% | 50.0 | NR | NR | 36 | Death, MI, angina for hospitalization |
| SWEDEHEART[31] 2017(Sweden) | Retrospective | 8118 | 65 | 39 | Indefinite | Positive | < 50% | 90.1 | 66.4 | 84.5 | 12 | All-cause and CV death, hospitalization for MI, heart failure and stroke |
| Conte 2017[34](Italy) | Retrospective | 245 | 63 | 69.8 | Indefinite | Negative | 1%–49% | 29 | NR | 22.9 | 98 | All-cause and CV death, ACS, revascularization |
| KAMIR 2016[30](South Korea) | Retrospective | 501 | 58 | 69.3 | Definite | Positives | < 50% | 77.3 | NR | 58.3 | 12 | All-cause death, MI, revascularization |
| Ishii 2016[23](Japan) | Retrospective | 224 | 67 | 58.0 | Definite | Negative | ≤50% | 50.0 | NR | 34.8 | 60 | CV death, ACS |
| Lim 2016[29](South Korea) | Retrospective | 721 | 56 | 83.5 | Definite | Negative | ≤50% | 60.2 | NR | 40.9 | 52 | All-cause and CV death, ACS, revascularization |
| Hwang 2015[19](South Korea) | Retrospective | 8372 | 61 | 70.3 | Indefinite | Negative | 1%–49% | 44.8 | NR | 23.7 | 28 | All-cause death, revascularization |
| ONFIRM[28]2015(Canada) | Prospective | 10418 | 57 | 52.7 | Indefinite | Negative | < 50% | 37.7 | NR | 33.3 | 27 | All-cause death |
MI, myocardial infarction; ACS, acute coronary syndrome; DAPT, dual antiplatelet therapy; CV, cardiovascular; NR, not reported.
Primary endpoint
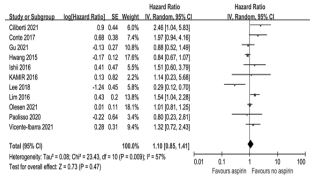
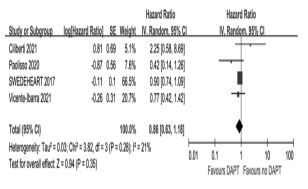
Eleven studies [11-15,20-22,24-27] compared the risk of MACEs in patients treated with aspirin or not. Pooled data showed that aspirin therapy was not associated with the risk of MACEs (HR 1.10; 95% CI0.85–1.41; P=0.47); however, the results had a large heterogeneity (I2=57%) (Figure 2). A small sample study [14] with extreme values might be the main source of heterogeneity, as excluding this study reversed the large heterogeneity (Supplementary Figure S1a). In addition, after excluding the study with diabetes mellitus only [12] and another one with medium quality [22], the changes in heterogeneity were not obvious, which suggested that they were not the main sources of heterogeneity (Supplementary Figure S1b,c). To further explore the source of heterogeneity, predefined subgroup analyses were performed. The interactions for all subgroups were not significant, except the follow-up duration (>36 vs.≤ 36 months), and aspirin use was not associated with the risk of MACEs in all subsets (Table 3). Similarly, dual antiplatelet therapy was not associated with the risk of MACEs (HR 0.86; 95% CI 0.63–1.18; P=0.35, I2=21%) among the four studies that enrolled subjects with Myocardial Infarction with Non Obstructive Coronary Arteries (MINOCA) (Supplementary Figure S2) [13,23,24,27].
Table 2: Bias risk of individual studies using the Newcastle-Ottawa Scale.
| Study | Selection | Comparability | Outcome | Total score | |||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the exposed | Selection of the non-exposed | Ascertainment of exposure | Demonstrati on | Assessment of outcome | Follow-up length | Adequacy of follow-up | |||
| Vicente-Ibarra 2021[35] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | |
| Olesen 2021[20] | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 8 | |
| Gu 2021[33] | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 8 | |
| Ciliberti 2021[32] | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8 | |
| Paolisso 2020[21] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | |
| Lee 2018[22] | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 7 | ||
| SWEDEHEART 2017[31] | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9 |
| Conte 2017[34] | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | ☆ | 7 | |
| KAMIR 2016[30] | ☆ | ☆ | ☆ | ☆ | ☆ | 5 | |||
| Ishii 2016[23] | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 7 | ||
| Lim 2016[29] | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 8 | |
| Hwang 2015[19] | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | 8 | |
| CONFIRM 2015[28] | ☆ | ☆ | ☆ | ☆ | ☆☆ | ☆ | ☆ | ☆ | 9 |
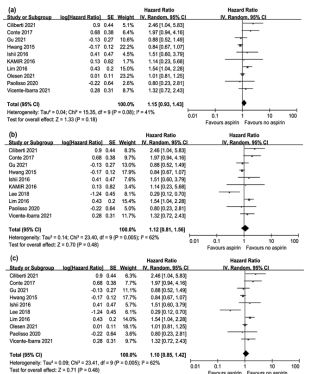
Supplementary Figure S1: Association of major adverse cardiovascular events with aspirin therapy after excluding individual studies. (a) Pooled hazard ratio after excluding the study by Lee et al. (b) Pooled hazard ratio after excluding the study by Olesen et al. (c) Pooled hazard ratio after excluding the KAMIR study.
Secondary endpoints
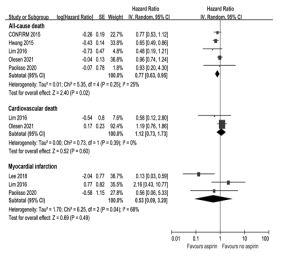
Five studies [11-13,20,21] compared the risk of all-cause death in non obstructive CAD patients treated with aspirin or not. Pooled data showed that aspirin use reduced the risk of all-cause death by 23% (HR 0.77; 95% CI 0.63–0.95; P=0.02, I2=25%) (Figure 3). Post-hoc sensitivity analysis was performed to confirm the effect of individual studies on the pooled data. The result was no longer statistically significant after excluding the study by Hwangetal. (Supplementary Figure S3) [11]. Two [12,21] and three studies [13,14,21] compared the risk of cardiovascular death and MI in patients treated with or without aspirin, respectively. As shown in Figure 3, aspirin use was not associated with the risk of cardiovascular death (HR 1.12; 95% CI 0.73–1.73; P=0.60, I2=0%) and MI (HR 0.53; 95% CI 0.09–3.20; P=0.49, I2=68%).
Safety endpoint
Only one study [12] reported the adverse effects of aspirin on bleeding risk. No difference in bleeding risk was found in nonobstructive CAD patients who received aspirin or not (HR 0.95; 95% CI 0.73–1.23; P=0.70).
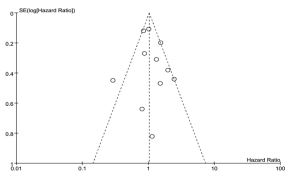
Publication bias
Publication bias for MACEs across studies was evaluated using funnel plot and Egger’s tests. The funnel plot was symmetrical and the Egger’s value was P=0.517, suggesting that there was no publication bias (Figure 4).
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis to investigate the association between aspirin use and the prognosis of nonobstructive CAD. Based on the pooled data from thirteen studies with 34,463 participants, this study revealed that routine aspirin therapy was not associated with decreased risks of MACEs, cardiovascular death and MI, but correlated with a reduced risk of all-cause death.
Table S1: Supplementary Table S1 Detailed search strategies.
| Databases | Search strategies |
|---|---|
| Pubmed (1520) | |
| #1 | "non?obstruct*"[tiab] OR "non obstruct*"[tiab] OR "no obstruct*"[tiab] OR "without obstruct*"[tiab] OR "absent obstruct*"[tiab] OR "non?significant"[tiab] OR "insignificant"[tiab] OR "non significant"[tiab] OR "no significant"[tiab] OR "near normal"[tiab] OR "mild"[tiab] |
| #2 | "atherosclerotic stenosis"[tiab] OR "coronary stenosis"[Mesh] OR "stenotic lesion*"[tiab] OR"coronary artery"[tiab] OR "coronary arteries"[tiab] |
| #3 | "aspirin"[tw] OR "anti?platelet"[tiab] OR "acetylsalicylic acid"[tw] OR "anti?thrombocytic"[tiab] OR "prevention"[tiab] OR "medication"[tiab] |
| #4 | #1 AND #2 AND #3 |
| Embase (1614) | |
| #1 | 'non?obstruct*':ab,ti OR 'non obstruct*':ab,ti OR 'no obstruct*':ab,ti OR 'without obstruct*':ab,ti OR 'absent obstruct*':ab,ti *’’ OR ’'absence of obstruct*':ab,ti OR 'non?significant':ab,ti OR 'insignificant':ab,ti OR 'non significant':ab,ti OR 'no significant':ab,ti OR 'near normal’’:ab,ti OR 'mild’':ab,ti |
| #2 | 'atherosclerotic stenosis':ab,ti OR 'coronary stenosis'/exp OR 'stenotic lesion*':ab,ti OR 'coronary artery'/exp OR 'coronary arteries':ab,ti |
| #3 | 'aspirin' OR 'anti?platelet':ab,ti OR 'acetylsalicylic acid' OR 'anti?thrombocytic':ab,ti OR 'prevention':ab,ti OR ' medication':ab,ti |
| #4 | #1 AND #2 AND #3 |
| Web of Science (1477) | |
| #1 | TS="nonobstruct*" OR TS="non obstruct*" OR TS="no obstruct*" OR TS="without obstruct*" OR TS="absent obstruct*" OR TS="absence of obstruct*" OR TS="non?significant" OR TS="insignificant" OR TS="non significant" OR TS="no significant" OR TS="near normal" OR TS="mild" |
| #2 | TS="atherosclerotic stenosis" OR TS="coronary stenosis" OR TS="stenotic lesion*" OR TS="coronary artery" OR TS="coronary arteries" |
| #3 | ALL="aspirin" OR TS="anti?platelet" OR ALL="acetylsalicylic acid" OR TS="anti?thrombocytic" OR TS="prevention" OR TS="medication" |
| #4 | #1 AND #2 AND #3 |
| Cochrane (83) | |
| ("non?obstruct*" OR "non obstruct*" OR "no obstruct*" OR "without obstruct*") AND ("atherosclerotic stenosis" OR "coronary stenosis" OR "stenotic lesion*" OR "coronary artery" OR "coronary arteries") AND ("aspirin" OR "anti?platelet" OR "acetylsalicylic acid" OR "anti?thrombocytic" OR "prevention" OR "medication") | |
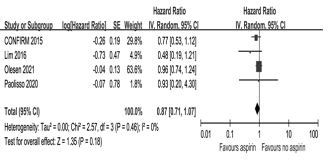
Table 3: Subgroup analyses for major adverse cardiovascular events.
| Subgroup | No. of studies | No. of patients | HR | 95% CI | I2 | P | P for interacti on |
|---|---|---|---|---|---|---|---|
| Follow-up | |||||||
| ≤36months | 5 | 9235 | 0.80 | 0.51-1.27 | 49% | 0.34 | 0.08 |
| >36months | 6 | 6692 | 1.31 | 0.97-1.76 | 49% | 0.07 | |
| Study design | |||||||
| Prospective | 1 | 88 | 0.80 | 0.23-2.81 | 0.73 | 0.62 | |
| Retrospective | 10 | 15839 | 1.11 | 0.86-1.44 | 61% | 0.43 | |
| CAS | |||||||
| Definite | 4 | 1600 | 0.95 | 0.41-2.20 | 74% | 0.90 | 0.78 |
| Indefinite | 7 | 14327 | 1.07 | 0.85-1.36 | 43% | 0.55 | |
| Baseline MI | |||||||
| Positive | 4 | 1330 | 1.45 | 0.93-2.26 | 0% | 0.10 | 0.20 |
| Negative | 7 | 14597 | 1.02 | 0.77-1.36 | 67% | 0.88 | |
| Sample size | |||||||
| ≤600 | 6 | 1332 | 1.03 | 0.57-1.86 | 59% | 0.91 | 0.86 |
| >600 | 5 | 14595 | 1.10 | 0.84-1.44 | 64% | 0.50 | |
| Adjustment | |||||||
| Yes | 7 | 14973 | 1.03 | 0.76-1.39 | 69% | 0.85 | 0.24 |
| No | 4 | 954 | 1.41 | 0.92-2.15 | 0% |
HR: hazard ratio; CI: confidence interval; CAS: coronary artery spasm; MI: myocardial infarction.
The benefit of aspirin therapy is well established for secondary prevention in patients with at herosclerotic diseases, and a low-dose of aspirin is recommended by the guidelines of the European Society of Cardiology [28]. Unfortunately, in contrast to previous randomized trials that majorly recruited patients with obstructive CAD, few randomized trials have probed the association between routine aspirin use and cardiovascular events in patients with non obstructive CAD. Increasing evidence indicates that patients with non obstructive CAD already develop slight at herosclerotic alterations with a higher risk of cardiovascular events [7,29]. As a result, more aggressive management might be needed for these patients. At present, the recommendations of guidelines for aspirin therapy in patients with non obstructive CAD are ambiguous. Indeed, the extreme variation in aspirin prescription rates (29.0%–90.1%) in our study corroborated the dilemma of aspirin use in non obstructive CAD. Therefore, evidence from our study that aspirin therapy failed to improve the prognosis of non obstructive CAD might shed light on the management of this disease with aspirin in the future.
Several studies have assessed the impact of antiplatelet therapy on cardiovascular events in patients with non obstructive CAD. In patients diagnosed with MINOCA, an observational study reported that aspirin use was not associated with a significantly reduced risk of the composite of adverse cardiovascular events (odds ratio 0.601; 95% CI 0.305–1.183) during 2-year follow-up [30]. Similarly, another study with a 3-year follow-up showed that antiplatelet agents did not improve the prognosis of non obstructive CAD (HR 1.089; 95% CI 0.642–1.847) [31]. Because of the different effect sizes and lack of detailed antiplatelet regimens, these two studies were excluded from our meta-analysis. Another two studies that enrolled participants without a medical history of MI also found that aspirin therapy had no beneficial effect [12,20], which was consistent with our findings. However, these studies were insufficiently representative, as participants with MI were either included or excluded. Our combined data showed that aspirin therapy did not improve the prognosis of patients with non obstructive CAD regardless of whether they suffered from baseline MI or not, which was first reported (Table 3).
Of note, according to current guidelines, once a diagnosis of MI is confirmed, aspirin as well as P2Y12 receptor antagonists should be routinely administered [28]. However, there is a debate as to whether antiplatelet agents should be routinely prescribed to patients with MINOCA. Luiset al. reported that insufficient secondary prevention medications (e.g., aspirin) were responsible for the poor outcome among MINOCA patients with “normal” cardiac magnetic resonance images [32]. On the contrary, a post-hoc analysis of the CURRENT-OASIS 7 trial showed that potent antiplatelet therapy might increase the risk of cardiovascular events [33]. The pooled data from our study indicated that aspirin therapy was not associated with improved prognosis in patients with nonobstructive CAD. Consistently, the results of dual antiplatelet therapy data from four studies could further strengthen this conclusion.
Our study showed that aspirin use reduced the risk of all-cause death in patients with non obstructive CAD, with no effects on cardiovascular death or MI. Post-hoc sensitivity analyses of all-cause death indicated a reversible result after excluding the study by Hwang et al (Supplementary Figure S3) [11]. In their study, more than half of aspirin users did not receive statin therapy, which suggested that the beneficial effects of aspirin on all-cause death might be influenced by a lower prescription rate of statins (23.7%). Currently, statins are widely available at a low price, and the effect of statinsis superior to that of aspirin in primary prevention [10]. Multiple studies have shown that statins can perform well in the management of patients with non obstructive CAD [12,15,20,22,23]. The efficacy of aspirin is likely to be attenuated or covered because of the gradually increasing prescription rate of statins [10]. Hence, the association between routine aspirin therapy and all-cause death remains unclear in patients with non obstructive CAD under the comprehensive management of risk factors, such as smoking, diabetes, dyslipidemia, and hypertension, which requires further investigation.
Non obstructive CAD is a heterogeneous disease with multiple potential underlying conditions, including vulnerable plaque, CAS, microvascular dysfunction and myocarditis, which may explain why aspirin use was not associated with improved outcomes.
First, critical findings might be ignored when evaluating coronary stenosis with coronary angiography alone. Intravascular imaging showed that vulnerable plaques, such as plaque rupture and plaque erosion, were detected in a few patients with non obstructive CAD, which could eventually develop into thrombi [34]. It was reasonable to prescribe antiplatelet agents to patients with thrombi. Although antiplatelet therapy based on intravascular imaging should be the target, in actual clinical practice it is not readily available due to the cost–benefit ratio. Additionally, it was showed that plaque burden, rather than vulnerable plaque, was a stronger predictor for patients with non obstructive CAD [35]. The plaque burden was also associated with similar ischemic events, regardless of the presence or absence of obstructive CAD [36]. Indeed, coronary stenosis is positively correlated with plaque burden [36]. Overall, patients with non obstructive CAD had a lower plaque burden than those with obstructive CAD [36]. This might explain why aspirin therapy was not as effective as expected in patients with non obstructive CAD. On the other hand, those with a higher plaque burden may benefit from antiplatelet therapy. For example, two studies showed that only patients with a coronary artery calcium score of ≥100 were likely to benefit from aspirin therapy in the primary prevention of a therosclerotic disease [37,38]. Therefore, future research is needed to support our hypothesis that a personalized antiplatelet regimen based on plaque burden might contribute to reduction in ischemic cardiovascular events in patients with non obstructive CAD.
Second, a previous study showed that CAS accounted for approximately 60% of patients with stable angina, indicating that it isa commoncondition in patients with non obstructive CAD [39]. Similarly, a systematic review revealed that approximately 30% of MINOCA might be induced by CAS [3]. The presence of CAS was associated with poor outcomes in these patients [5]. However, limited evidence is available regarding the effects of aspirin therapy on CAS. A high dose of aspirin (>325 mg daily) was considered as a potential inducer of coronary spasm [40], whereas a low dose of aspirin had the opposite effect [41]. Conversely, another study found that aspirin therapy might lead to CAS even at a low dose [42]. Hence, the impact of aspirin therapy on the prognosis of CAS was under ongoing debate. A recent meta-analysis showed that there was no significant association between aspirin use and clinical outcomes among patients with vasospastic angina without organic stenosis [43]. In the present study, pooled data based on a subset of CAS also indicated that aspirin use was not associated with the risk of cardiovascular events (Table 3). Of note, this finding should be interpreted with caution because of the post-hoc nature of subgroup analysis.
Third, althougha few of patients with nonobstructive CADcould presentwith angina-like chest pain, there was no evidence of myocardial ischemia [1,3]. Several non-ischemic diseases, including myocarditis, cardiomyopathy, and Takotsubo syndrome, can mimic MI in patients with MINOCA. Previous studies have shown that routine aspirin usedoes not reduce the risk of cardiovascular events in non-ischemia settings [44,45]. In addition, a meta-analysis reported that aspirin therapy might worsen the long-term prognosis of patients with Takotsubo syndrome without any benefit [46].
Limitations
There are several limitations of our study. First, the definitions of the primary endpoint differed slightly between the studies, which might be a potential source of heterogeneity in our results. Second, our results were extracted from observational cohort studies, most of which were retrospective. In addition, a small amount of the extracted data was unadjusted. Although subgroup analyses based on study design and adjustment revealed no interaction effects, our results might still be affected by potential confounding factors. Third, the lack of reported haemorrhagic events might affect the outcome in patients on aspirin therapy. Finally, only published studies were included in the meta-analysis. The results might be corrected by unpublished studies, despite no evidence of publication bias. Currently, a prospective, multicenter, randomized trial is in progress, in which 4422 women suspected of myocardial ischemia with non obstructive CAD have been recruited [47]. This trial may provide additional information about the efficacy of aspirin therapy (NCT03417388).
Conclusion
Routine aspirin therapy might not be associated with reduced risks of cardiovascular events in patients with non obstructive CAD. A personalized antiplatelet regimen might contribute to reduction in ischemic cardiovascular events for these patients.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Not applicable.
Declaration of interest: None.
Funding: This work was supported by the National Natural Science Foundation of China (No.81900628), Youth Training Program of General Logistics Department Health Research Project (20QNPY033), and Military Medicine Youth Training Program of Army Medical University (2019XQN018).
Acknowledgements: We would like to thank Editage (www.editage.cn) for English language editing.
Author contributions:
Hua-ping Fan: Conceptualization, methodology, data curation and extraction, writing-original draft preparation.
Shuai Mao: Conceptualization, methodology, data curation and extraction.
Yu Zhou: Software.
Jun Jin: Conceptualization, supervision, reviewing and editing.
Quan-you Zheng: Funding acquisition, conceptualization, supervision, reviewing and editing.
Data availability: All data generated or analyzed during this study are available from the first or corresponding author upon reasonable request.
References
- Bairey Merz CN, Pepine CJ, Walsh MN, Fleg JL. Ischemia and No Obstructive Coronary Artery Disease (INOCA): Developing Evidence-Based Therapies and Research Agenda for the Next Decade. Circulation. 2017; 135: 1075-1092.
- Wang ZJ, Zhang LL, Elmariah S, Han HY, Zhou YJ, et al. Prevalence and Prognosis of Nonobstructive Coronary Artery Disease in Patients Undergoing Coronary Angiography or Coronary Computed Tomography Angiography: A Meta-Analysis. Mayo Clin Proc. 2017; 92: 329-346.
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF, et al. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015; 131: 861-870.
- Dastidar AG, Baritussio A, De Garate E, et al. Prognostic Role of CMR and Conventional Risk Factors in Myocardial Infarction With Nonobstructed Coronary Arteries. JACC Cardiovasc Imaging. 2019; 12: 1973-1982.
- Nishimiya K, Suda A, Fukui K, et al. Prognostic Links Between OCT-Delineated Coronary Morphologies and Coronary Functional Abnormalities in Patients With INOCA. JACC Cardiovasc Interv. 2021; 14: 606-618.
- Bugiardini R, Bairey Merz CN. Angina with “normal” coronary arteries: A changing philosophy. Jama. 2005; 293: 477-484.
- Maddox TM, Stanislawski MA, Grunwald GK, et al. Nonobstructive coronary artery disease and risk of myocardial infarction. Jama. 2014; 312: 1754-1763.
- Honigberg MC, Lander BS, Baliyan V, et al. Preventive Management of Nonobstructive CAD After Coronary CT Angiography in the Emergency Department. JACC Cardiovasc Imaging. 2020; 13: 437-448.
- Hulten E, Bittencourt MS, Singh A, et al. Coronary artery disease detected by coronary computed tomographic angiography is associated with intensification of preventive medical therapy and lower low-density lipoprotein cholesterol. Circ Cardiovasc Imaging. 2014; 7: 629-638.
- Baigent C, Blackwell L, Collins R, et al. Aspirin in the primary and secondary prevention of vascular disease: Collaborative meta-analysis of individual participant data from randomised trials. Lancet. 2009; 373: 1849-1860.
- Hwang IC, Jeon JY, Kim Y, et al. Association between Aspirin Therapy and Clinical Outcomes in Patients with Non-Obstructive Coronary Artery Disease: A Cohort Study. PLoS One. 2015; 10: e0129584.
- Olesen KKW, Heide Jørgensen U, Thim T, et al. Statin but not Aspirin Treatment is Associated with Reduced Cardiovascular Risk in Patients with Diabetes without Obstructive Coronary Artery Disease. Eur Heart J Cardiovasc Pharmacother. 2021.
- Paolisso P, Bergamaschi L, Saturi G, et al. Secondary prevention medical therapy and outcomes in patients with myocardial infarction with non-obstructive coronary artery disease. Frontiers in Pharmacology. 2020; 10: 1606.
- Lee Y, Park HC, Shin J. Clinical efficacy of aspirin with identification of intimal morphology by optical coherence tomography in preventing event recurrence in patients with vasospasm-induced acute coronary syndrome. Int J Cardiovasc Imaging. 2018; 34: 1697-1706.
- Ishii M, Kaikita K, Sato K, et al. Impact of aspirin on the prognosis in patients with coronary spasm without significant atherosclerotic stenosis. International Journal of Cardiology. 2016; 220: 328-332.
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. Bmj. 2009; 339: b2700.
- Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011.
- Wells G, Shea B, O’Connell J. The Newcastle-Ottawa Scale (NOS) for Assessing The Quality of Non randomised Studies in Meta-analyses. Ottawa Hospital Research Institute. oxford. asp, 2011.
- Yang YL, Xiang ZJ, Yang JH, et al. Association of beta-blocker use with survival and pulmonary function in patients with chronic obstructive pulmonary and cardiovascular disease: A systematic review and meta-analysis. Eur Heart J. 2020; 41: 4415-4422.
- Chow BJ, Small G, Yam Y, et al. Prognostic and therapeutic implications of statin and aspirin therapy in individuals with nonobstructive coronary artery disease: Results from the CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An Inte Rnational Multicenter registry) registry. Arterioscler Thromb Vasc Biol. 2015; 35: 981-989.
- Lim AY, Park TK, Cho SW, et al. Clinical implications of low-dose aspirin on vasospastic angina patients without significant coronary artery stenosis; a propensity score-matched analysis. Int J Cardiol. 2016; 221: 161-166.
- Piao ZH, Jeong MH, Li Y, et al. Benefit of statin therapy in patients with coronary spasm-induced acute myocardial infarction. Journal of Cardiology. 2016; 68: 7-12.
- Lindahl B, Baron T, Erlinge D, et al. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation. 2017; 135: 1481-1489.
- Ciliberti G, Verdoia M, Merlo M, et al. Pharmacological therapy for the prevention of cardiovascular events in patients with Myocardial Infarction With Non-Obstructed Coronary Arteries (MINOCA): Insights from a multicentre national registry. International Journal of Cardiology. 2021; 327: 9-14.
- Gu H, Lu B, Gao Y, et al. Prognostic Value of Atherosclerosis Progression for Prediction of Cardiovascular Events in Patients with Nonobstructive Coronary Artery Disease. Academic Radiology. 2021; 28: 980-987.
- Conte E, Annoni A, Pontone G, et al. Evaluation of coronary plaque characteristics with coronary computed tomography angiography in patients with non-obstructive coronary artery disease: A long-term follow-up study. Eur Heart J Cardiovasc Imaging. 2017; 18: 1170-1178.
- Vicente-Ibarra N, Feliu E, Bertomeu-Martínez V, et al. Role of cardiovascular magnetic resonance in the prognosis of patients with myocardial infarction with non-obstructive coronary arteries. J Cardiovasc Magn Reson.2021; 23(1):83.
- Visseren FLJ, Mach F, Smulders YM, et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021; 42: 3227-3337.
- Jespersen L, Hvelplund A, Abildstrøm SZ, et al. Stable angina pectoris with no obstructive coronary artery disease is associated with increased risks of major adverse cardiovascular events. Eur Heart J. 2012; 33: 734-744.
- Abdu FA, Liu L, Mohammed AQ, et al. Effect of Secondary Prevention Medication on the Prognosis in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. J Cardiovasc Pharmacol. 2020; 76: 678-683.
- Gu XH, He CJ, Shen L, Han B. Association Between Depression and Outcomes in Chinese Patients With Myocardial Infarction and Nonobstructive Coronary Arteries. J Am Heart Assoc. 2019; 8: e011180.
- Luis SA, Luis CR, Habibian M, et al. Prognostic Value of Cardiac Magnetic Resonance Imaging in Acute Coronary Syndrome Patients With Troponin Elevation and Nonobstructive Coronary Arteries. Mayo Clin Proc. 2021; 96: 1822-1834.
- Bossard M, Gao P, Boden W, et al. Antiplatelet therapy in patients with myocardial infarction without obstructive coronary artery disease. Heart. 2021; 107: 1739-1747.
- Gerbaud E, Arabucki F, Nivet H, et al. OCT and CMR for the Diagnosis of Patients Presenting With MINOCA and Suspected Epicardial Causes. JACC Cardiovasc Imaging. 2020; 13: 2619-2631.
- Arbab-Zadeh A, Fuster V. The myth of the “vulnerable plaque”: Transitioning from a focus on individual lesions to atherosclerotic disease burden for coronary artery disease risk assessment. J Am Coll Cardiol. 2015; 65: 846-855.
- Mortensen MB, Dzaye O, Steffensen FH, et al. Impact of Plaque Burden Versus Stenosis on Ischemic Events in Patients With Coronary Atherosclerosis. J Am Coll Cardiol. 2020; 76: 2803-2813.
- Ajufo E, Ayers CR, Vigen R, et al. Value of Coronary Artery Calcium Scanning in Association With the Net Benefit of Aspirin in Primary Prevention of Atherosclerotic Cardiovascular Disease. JAMA Cardiol. 2021; 6: 179-187.
- Cainzos-Achirica M, Miedema MD, McEvoy JW, et al. Coronary Artery Calcium for Personalized Allocation of Aspirin in Primary Prevention of Cardiovascular Disease in 2019: The MESA Study (Multi-Ethnic Study of Atherosclerosis). Circulation. 2020; 141: 1541-1553.
- Ohba K, Sugiyama S, Sumida H, et al. Microvascular coronary artery spasm presents distinctive clinical features with endothelial dysfunction as nonobstructive coronary artery disease. J Am Heart Assoc. 2012; 1: e002485.
- Miwa K, Kambara H, Kawai C. Exercise-induced angina provoked by aspirin administration in patients with variant angina. Am J Cardiol. 1981; 47: 1210-1214.
- Bax WA, Renzenbrink GJ, van der Linden EA, et al. Low-dose aspirin inhibits platelet-induced contraction of the human isolated coronary artery. A role for additional 5-hydroxytryptamine receptor antagonism against coronary vasospasm? Circulation. 1994; 89: 623-629.
- Park JY, Rha SW, Poddar KL, et al. Impact of low-dose aspirin on coronary artery spasm as assessed by intracoronary acetylcholine provocation test in Korean patients. J Cardiol. 2012; 60: 187-191.
- Lin Y, Chen Y, Yuan J, et al. Impact of aspirin use on clinical outcomes in patients with vasospastic angina: a systematic review and meta-analysis. BMJ Open. 2021; 11: e048719.
- Gaziano JM, Brotons C, Coppolecchia R, et al. Use of aspirin to reduce risk of initial vascular events in patients at moderate risk of cardiovascular disease (ARRIVE): a randomised, double-blind, placebo-controlled trial. Lancet. 2018; 392: 1036-1046.
- McNeil JJ, Wolfe R, Woods RL, et al. Effect of Aspirin on Cardiovascular Events and Bleeding in the Healthy Elderly. N Engl J Med. 2018; 379: 1509-1518.
- Rizzetto F, Lia M, Widmann M, et al. Prognostic impact of antiplatelet therapy in Takotsubo syndrome: A systematic review and meta-analysis of the literature. Heart Fail Rev. 2021.
- Handberg EM, Merz CNB, Cooper-Dehoff RM, et al. Rationale and design of the Women’s Ischemia Trial to Reduce Events in Nonobstructive CAD (WARRIOR) trial. Am Heart J. 2021; 237: 90-103.