
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Cervical epidural blood patch in spontaneous
intracranial hypotension: A case report
Saqiba Tahir; Zainab Shabbir; Azhar Rehman; Gauhar Afshan*
Department of Anaesthesiology, Aga Khan University Hospital, Pakistan.
*Corresponding Author : Gauhar Afshan
Professor & Consultant, Department of Anaesthesiology, Aga Khan University Medical College, Karachi-74800, Pakistan.
Tel: (+92) 213-4864545,
Fax: (+92) 213-493 4294, 493 2095;
Email: gauhar.afshan@aku.edu
Received : Aug 15, 2022
Accepted : Sep 05, 2022
Published : Sep 12, 2022
Archived : www.jcimcr.org
Copyright : © Afshan G (2022).
Abstract
Background: Spontaneous Intracranial Hypotension (SIH) results from a decrease in cerebrospinal fluid volume without any iatrogenic cause and presents most commonly with orthostatic headache. Cervical dural tears are an uncommon cause of SIH. Cervical epidural blood patch has been successfully used in many developed countries for the treatment of spontaneous intracranial hypotension after failure of conservative management.
Case presentation: A 35-year-old woman came with a unilateral orthostatic headache radiating to the neck along with vomiting. She did not have any history of trauma or any recent neuraxial anaesthesia/analgesia. MRI cervical spine suggested a breach in dura at C2 level with extradural collection extending from C2-4 level. CT myelogram showed dural leak at C2-3 level. She failed to respond to conservative management. A multidisciplinary team was involved, and it was decided to proceed with cervical epidural blood patch with surgery for dural repair being the last resort.
Fluoroscopy guided cervical epidural blood patch was planned. Epidural space at T7-T8 was located under fluoroscopy using a 16-gauge Tuohy needle however, the 20 gauge epidural catheter could not be advanced to the desired site i.e. C2-C4. Tuohy needle was re-sited at T5-T6 level and catheter was advanced. Tip of the catheter was confirmed with Omnipaque dye under fluoroscopy and 5 mls of autologous blood was given with spread seen up to C2 level. Patient had complete resolution of the headache and no neurological deficits were seen. She was observed for 24 hours and discharged home the next day.
Conclusion: Fluoroscopy guided cervical epidural blood patch is an effective treatment for cervical dural tears causing symptoms of spontaneous intracranial hypotension that are not responding to conservative management.
Keywords: Intracranial hypotension; Cervical epidural blood patch; Dural leak.
Citation: Tahir S, Shabbir Z, Rehman A, Afshan G. Cervical epidural blood patch in spontaneous intracranial hypotension: A case report. J Clin Images Med Case Rep. 2022; 3(9): 2046.
Introduction
Intracranial pressure is the result of production, flow and absorption of CSF. Any changes in these processes leads to altered CSF pressure causing various neurological symptoms, most common of which is an orthostatic headache [1]. However patients may also present with focal neurological deficits or altered mentation [2]. Spontaneous Intracranial Hypotension (SIH) is an unusual cause of orthostatic headache in young and middle-aged individuals [3]. It was first described by Georg Schaltenbrand in 1938 [4]. It is now thought that it occurs as a result of a decrease in CSF volume resulting from spontaneous CSF leaks rather than a decrease in CSF pressure [5,6]. A decrease in CSF volume precipitates brain sagging in the cranial vault which causes traction on the sensory nerves of the meninges and the bridging veins, leading to headaches.
Postural or orthostatic headache is due to the fact that the traction on the meninges is increased in an upright position (vertical) leading to increased intensity of headache when standing. Low CSF pressure in the cranial vault is compensated by an increase in vasodilation of the cerebral vessels. This phenomenon causes headaches due to increased brain volume [7].
Incidence is estimated to be 5 in 100,000 cases per year with peak occurring at 40 years of age [8,9]. Females are twice more commonly affected than males [8]. CSF leak occurs due to dural defects which are present either congenitally or are acquired secondary to trauma. Therefore, various factors contribute to CSF leakage such as congenital connective tissue disorders, defective dura around nerve root sheaths, osteophytic protrusions, intervertebral disc herniation or meningeal diverticula [10,11].
Low CSF pressure may show up in MRI scans as pachymeningeal enhancement, brain “sagging”, tonsillar descent, posterior fossa crowding and dilated epidural veins [12]. Radioisotope cisternography can be done for a suspected CSF leak where MRI is normal or non-diagnostic [12]. The best test to identify the exact site of CSF leak is CT myelography [13,5].
Uncomplicated mild to moderate headaches may initially be treated conservatively with bed rest, hydration, caffeine and abdominal binders [14]. Mainstay of interventional therapy is Epidural Blood Patch (EBP) [2]. Repeat epidural blood patch may be considered using a higher volume after 5 days [3]. Percutaneous fibrin sealant may be placed if epidural blood patch fails [3]. Surgery is considered in those where all non-surgical measures including two or more epidural blood patches have failed and the leak sites are clearly identified [15,16]. In one study, epidural blood patch done via fluoroscopy at the lumbar level completely resolved symptoms in 85% of patients with post-dural puncture headaches [17]. Another study reported relief of headache with EBP in 52% patients whereas 22% required a second EBP for relief of symptoms [2]. However, cervical epidural blood patch is uncommon due to the fear of neurological complications such as spinal cord compression [9].
Cases have been described from the developed world, but we did not find any case reports from developing countries on this subject. We hereby describe a case of a young lady who had postural headache secondary to spontaneous intracranial hypotension due to a cervical dural tear and was successfully treated with a fluoroscopy guided cervical epidural blood patch.
Case report
A 35-year-old lady with no prior co-morbids came to the neurology clinic with the complaint of headache in the left parieto-occipital region radiating to the left side of the neck and upper back for the past 5 days along with vomiting for 2 days. It had a gradual onset with no history of trauma, fall or any recent lumbar puncture. No recent history of spinal or epidural anaesthesia/analgesia was present. Patient had 3 lower segment Caesarean sections and the last one was done one and a half years back under spinal anaesthesia. Pain was continuous without any associated aura, photophobia, phono-phobia, visual changes, dizziness, rhinorrhea, otorrhea, fever, seizures or any neurological deficits. Headache increased on sitting and standing and persisted even with lying down. Conservative management including use of analgesics prescribed brought only a transient decrease in symptom intensity.
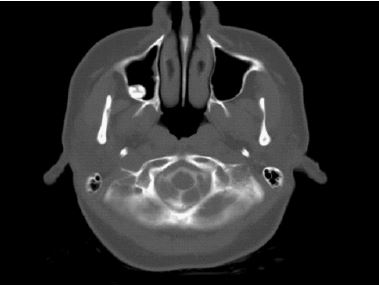
MRI of the spine was done. MRI cervical spine showed an extradural collection with high intensity on T1 and T2 weighted images compared to CSF along anterior thecal sac extending from C2-4 level in bilateral parasagittal location with suggestion of breach in anterior thecal sac at C2 vertebral body level (Figure 1). MRI lumbar spine revealed an extradural collection along anterior thecal sac of variable signal intensity extending from upper border of L2 to lower border of S2 vertebral body with suggestion of breach at L1-L2 level and diffuse dural enhancement seen in the lumbar spine. CT myelogram was subsequently done to localize CSF leak which was found at level of C2-C3, and no evidence of CSF leak was identified at the lumbar region.
A multidisciplinary team was involved, and the patient was planned for an epidural blood patch keeping surgical repair of dura mater as the last option. Informed consent for the epidural blood patch was taken.
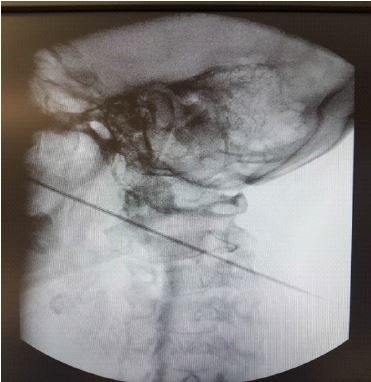
In the operating room, the patient was placed in a prone position and basic monitoring was applied. After all aseptic measures and local infiltration of lignocaine 2%, a 16-gauge Tuohy needle was inserted at T2 vertebral level and epidural space was identified using loss of resistance technique and fluoroscopy guidance. A 20-gauge catheter was advanced cephalad until it would not go any further, subsequently dye was injected, and spread was not seen at C2-C3 level. Thereafter, Tuohy needle was re-inserted. Epidural space was located using the same technique and a 20-gauge epidural catheter was threaded in viathe Tuohy needle and advanced. Tip of the catheter was confirmed with radio-opaque dye, Omnipaque, under fluoroscopy and 5 mls of autologous blood was given with spread seen up to C2 level (Figure 2). At this point, the patient complained of transient pain in left arm. Post-procedure, the patient was kept under close observation with relief of headache seen within the hour and no neurological deficits were seen. Patient remained stable throughout her stay and was discharged home after 24 hours. 3 months since the procedure, she remains pain free.
Discussion
Intracranial hypotension syndrome is caused by low CSF volume secondary to either CSF leak or medical conditions causing dehydration. CSF leak may occur either due to trauma, iatrogenically during surgery or with performance of neuraxial anaesthesia/analgesia techniques, or it may occur spontaneously. The initial misdiagnosis remains the norm because of lack of physician’s familiarity with the disease process [3]. Patients typically present with orthostatic headache and may have nausea/vomiting, neck stiffness, visual defects, and other neurological symptoms [14,15,9,18,19]. However, when CSF leak remains untreated, the orthostatic component may decrease or disappear [3,15]. The pain may be diffuse or localized and is rarely unilateral [3].
Interestingly, our patient presented with a unilateral headache. SIH usually responds to conservative management. However, failure to respond to medical management may need treatment with invasive procedures such as epidural blood patch. CSF leak at cervical level is uncommon. Cervical epidural blood patch is feared for its complications such as spinal cord compression, cranial nerve palsies, altered mentation, subdural hematomas, seizures, transient bradycardia but still has been used successfully in the treatment of cervical epidural tears.
In a literature review done by Kapoor and Ahmed that included 19 patients, the most common complication seen was neck pain or pressure and no neurological or vascular complications were seen [9]. Our patient complained of transient arm pain only. Some of the case reports reviewed had patients with CSF leak at lower cervical levels [16,20] whereas others reported higher levels of CSF leak [14,21-24]. Direct epidural blood patch was placed under CT guidance in some studies as the initial approach and in others if previous approach failed [15,18,21,25,26] whereas some other studies reported using an epidural catheter to reach the site of dural leak [14,19,22,23,27].
Repeat blood patch may be needed in case of failed treatment with the first blood Patch [2,9,19,28,29]. The anatomical epidural space becomes smaller as we ascend from the lumbar to the cervical region [15]. Required blood volume is determined by the onset of pain or radiculopathy [30]. We injected 5 mls of blood at the leak site. Most commonly used blood volume was between 5 to 8 mls (range: 2.5 mls to 15 mls) at the cervical level [9,14,19,21,18]. A targeted blood patch at the site of leak is preferable to blood patch placed other levels [9,31]. It may be because the main bulk of blood clot only extends three to five segments from the site of injection as seen by Beards in his study [32]. In our patient, we targeted the site of dural leak using an epidural catheter.
A different type of headache has also been reported to develop following successful treatment with epidural blood patch as a result of rebound intracranial hypertension. These headaches may wake the patient up from sleep and improve with upright positioning. It may take days, weeks, or months for CSF production to return back to normal [6]. However, we did not see any such adverse event in our patient.
Conclusion
Based on our experience and literature search, we feel that fluoroscopy guided cervical epidural blood patch is an effective treatment for cervical dural tears causing symptoms of spontaneous intracranial hypotension that are not responding to conservative management and saves the patient from a more invasive procedure of surgical dural repair.
References
- Muhammad Talha L, Sameer J. Spontaneous Intracranial Hypotension. 2020.
- Hazama A, John L, Braley AE, Chin LS, Krishnamurthy S. Spontaneous Intracranial Hypotension and the durability of Epidural Blood Patch. Neurosurgery. 2019; 66.
- Wouter S. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA. 2006; 295: 2286–2296.
- Kim D, Small JE. Intracranial Hypotension. In: Neuroradiology. 2019; 158-162.
- Bahram M. Spontaneous Intracranial Hypotension. Contin (Minneap Minn). 2015; 21: 1086–1088.
- Limaye K, Samant R, Lee RW. Spontaneous intracranial hypotension: diagnosis to management. Acta Neurol Belg. 2016; 116: 119–125.
- Mokri B. The Monro-Kellie hypothesis: applications in CSF volume depletion. Neurology. 2001; 56: 1746–1748.
- Deline C, Schievink WI, Cedars-Sinai. Spontaneous Intracranial Hypotension. Available from: https://rarediseases.org/rare-diseases/spontaneous-intracranial-hypotension/
- Kapoor SG, Ahmed S. Cervical epidural blood patch-A literature review. Pain Med (United States). 2015; 16: 1897–1904.
- Schievink WI, Gordon OK, Tourje J. Connective tissue disorders with spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension: a prospective study. Neurosurgery. 2004; 54: 65–70.
- Schievink WI, Jacques L. Recurrent spontaneous spinal cerebrospinal fluid leak associated with “nude nerve root” syndrome: case report. Neurosurgery. 2003; 53: 1216–1218.
- Sun-Edelstein C, Lay CL, Tung GA. Spontaneous intracranial hypotension: Pathophysiology, clinical features, and diagnosis. UpToDate,2020. Available from: https://www.medilib.ir/uptodate/show/3359
- Schievink WI, Meyer FB, Atkinson JL, Mokri B. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. J Neurosurg.1996; 84: 598–605.
- Kwon SY, Kim YS, Han SM. Spontaneous C1-2 Cerebrospinal Fluid Leak Treated with a Targeted Cervical Epidural Blood Patch Using a Cervical Epidural Racz Catheter. Pain Physician. 2014; 17: E381–E384.
- Lin J, Zhang S, He F, Liu M, Ma X, et al. The status of diagnosis and treatment to intracranial hypotension, including SIH. J Headache Pain. 2017; 18: 4.
- Wong AK, Rasouli MR, Ng A, Wang D. Targeted Epidural Blood Patches Under Fluoroscopic Guidance For Incidental Durotomies Related To Spine Surgeries: A Case Series. J Pain Res. 2019; 12: 2825–2833.
- Özütemiz C, Köksel YK, Huang H, Rubin N, Rykken JB, et al. The efficacy of fluoroscopy-guided epidural blood patch in the treatment of spontaneous and iatrogenic cerebrospinal fluid leakage. Eur Radiol. 2019; 29: 4088–4095.
- Rai A, Rosen C, Carpenter J, Miele V. Epidural blood patch at C2: Diagnosis and treatment of spontaneous intracranial hypotension. Am J Neuroradiol. 2005; 26: 2663–2666.
- Sykes KT, Yi X. Intracranial Hypotension Headache Caused by a Massive Cerebrospinal Fluid Leak Successfully Treated with a Targeted C2 Epidural Blood Patch: A Case Report. Pain Physician. 2013; 16: 399–404.
- Waguri N, Tomita M, Hayatsu K, Okamoto K, Shimoji K, et al. Epidural blood patch for treatment of spontaneous intracranial hypotension. Acta Anaesthesiol Scand. 2002; 46: 747–750.
- Allegri M, Lombardi F, Custodi VM, Scagnelli P, Corona M, Minella CE, et al. Spontaneous Cervical (C1-C2) Cerebrospinal Fluid Leakage Repaired with Computed Tomography-Guided Cervical Epidural Blood Patch. J Pain Symptom Manag. 2010; 40: e9–12.
- Wang E, Wang D. Successful treatment of spontaneous intracranial hypotension due to prominent cervical cerebrospinal fluid leak with cervical epidural blood patch. Pain Med. 2015; 16: 1013–1018.
- Inamasu J, Nakatsukasa M. Blood patch for spontaneous intracranial hypotension caused by cerebrospinal fluid leak at C1-2. Clin Neurol Neurosurg. 2007; 109: 716–719.
- Peng PW, Farb R. Spontaneous C1-2 CSF Leak Treated with High Cervical Epidural Blood Patch. Can J Neurol Sci. 2008; 35: 102–105.
- Cousins MJ, Brazier D, Cook R. Intracranial hypotension caused by cervical cerebrospinal fluid leak: Treatment with epidural blood patch. Anesth Analg. 2004; 98: 1794–1797.
- Dillo W, Josef Hollenhorst, Brassel F, Katharina von Hof-Strobach, Heidenreich F, et al. Successful treatment of a spontaneous cervical cerebrospinal fluid leak with a CT guided epidural blood patch. J Neurol. 2002; 249: 224-225.
- Megumi Kanao Kanda, Onodera Y, Kanda H, Sato I, Anno E, Kunisawa T. Targeted fluoroscopic guided epidural blood patch using a Racz catheter for spontaneous intracranial hypotension. J Clin Anesth. 2019; 57: 122–123.
- Sencakova D, Mokri B, McClelland RL. The efficacy of epidural blood patch in spontaneous CSF leaks. Neurology. 2001; 57: 1921-1923.
- Berroir S, Loisel B, Ducros A, Boukobza M, Tzourio C, Valade D, et al. Earlyepidural blood patch in spontaneous intracranial hypotension. Neurology. 2004; 63: 1950-1951.
- Martin R, Louy C, Babu V, Jiang Y, Far A, et al. A two-level large-volume epidural blood patch protocol for spontaneous intracranial hypotension: retrospective analysis of risk and benefit. Reg Anesth Pain Med. 2020; 45: 32-37.
- Gottschalk A. Cerebrospinal fluid leakage. Indications, technique and results of treatment with a blood patch. Radiologe. 2015; 55: 471–478.
- Beards SC, Jackson A, Griffiths AG, Horsman EL. Magnetic resonance imaging of extradural blood patches: Appearances from 30 min to 18 h. Br J Anaesth. 1993; 71: 182-188.