
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Giant apical cyst in anterior maxilla: A case report
Renato Gomes Azevedoa1; Percy Regis Bomentea1; Gestter Willian Lattari Tessarin1,2*
1University Center North Paulista (UNORP), São José do Rio Preto, SP, Brazil.
2Department of Basic Sciences, São Paulo State University (UNESP), School of Dentistry, Araçatuba, SP, Brazil.
*Corresponding Author : Gestter WL Tessarin
North University of São Paulo (UNORTE), São José do Rio Preto, SP 3460 10, Brazil.
Tel: (55) 17- 3203-2500;
Email: gestter@unorte.edu.br
Received : Aug 15, 2022
Accepted : Sep 05, 2022
Published : Sep 12, 2022
Archived : www.jcimcr.org
Copyright : © Tessarin GWL (2022).
Abstract
Apical or periapical cysts are the most common type of cyst, affecting the local and systemic health of patients. This pathology can manifest as an inflammatory condition in periodontal tissues due to the stimulation and proliferation of the epithelial cell rests of Malassez and it can be identified in clinical visits and imaging exams of routine. Apical cysts do not cause facial pain and/or swelling and appear as a well-defined radiolucent region when analyzed radiographically. Differential diagnosis include dentigerous cyst, ameloblastoma, odontogenic keratocyst, and periapical cementoma. Only a histopathological analysis can provide a definite diagnosis. Several methods have been described to treat apical cysts, such as endodontic therapies, decompression, marsupialization and cystectomy. A healthy 60-year-old man looked the dental office and reported successful endodontic treatment in the upper central and lateral incisors teeth and a tomographic exam suggested the presence of the large periapical cystic lesions located in the anterior region of the maxillary. After complementary exams, the cystic lesion was enucleated without endodontic. Histopathological analysis confirmed the hypothetical diagnosis which had been observed in the imaging exam. The patient’s clinical follow-up showed good evolution with no clinical symptoms and bone healing was observed in the region of the lesion. It is essential for dentists to have knowledge about diagnostic methods and treatments to avoid adverse effects in healthy teeth or other structures present in the face. Disseminating information about an uncommon case to the scientific community may help achieving success in similar situations.
Keywords: Apical cyst; Enucleation; Maxilla; Regression of apical cyst; Treatment.
Citation: Azevedoa RG, Bomentea PR, Tessarin GWL. Giant apical cyst in anterior maxilla: A case report. J Clin Images Med Case Rep. 2022; 3(9): 2047.
Introduction
Apical Cysts (AC) are probably developed by the stimulation and proliferation of epithelial cell rests of Malassez in teeth with periapical inflammatory conditions [1]. This type of lesion could be caused by many factors that affect healthy teeth, such as microorganism and their toxins, traumatic injury, unsuccessful endodontic therapy, and others [2,3]. Two forms of AC have been described: 1) true periapical cyst: with no connection or continuity to the root canal; 2) pocket cyst (also known as “bay cyst”): with a continuous connection to the root canal system through the apical foramen [1,3,4]. A study performed with human periapical lesions obtained from extracted teeth showed that, in 256 cases analyzed, 15% were periapical cysts, 9% of which were true cysts, while 6% were pocket cysts [5].
Clinically, in the initial stage, the Apical Cysts (ACs) are painless and do not swell, except when there are several inflammatory infiltrates around the cystic cavity [2,3]. Generally, this type of lesion is associated with non-vital teeth and is commonly discovered in routine radiographic exams in dental departments [3,6]. Radiographically, the AC often appears as a well-defined radiolucent region at the apex of a tooth that can cause bone resorption or expansion, mobility and displacement of teeth, and malocclusion when it is in an advanced stage of development [4,6-9]. Tomographic exams can also be used to evaluate cyst extension in coronal, sagittal, and axial extensions and bone and soft-tissue deficiencies can be evaluated with more precision and improve the plan of treatment [7,10,11]. In addition, histological analyses of AC have shown the presence of highly-vascularized dense connective tissue and chronic inflammatory infiltrates delimited by discontinuous, non-keratinized, and stratified squamous epithelium. In the center of the cystic lesion, cholesterol crystals can also be observed [12-14].
AC can be treated via non-surgical root canal or periapical surgery with or without tooth extraction [3]. The complexity anatomy of root canals system of teeth, the presence of several collateral canals, unsuccessful instrumentation or inaccessible regions from roots can promote difficult for removal the total infection may be permissive for maintenance of the periapical lesion, as AC [13]. In addition, true periapical cysts do not appear to respond adequately to conventional endodontic treatments and require Periapical Surgery (PS) [3]. In this situation, the PS consists in creating an access in the tooth apex, root, or resection, enucleating the lesion, and carrying out an endodontic treatment [15]. Clinical studies have reported that conventional endodontic retreatments before periapical surgery increase successful healing rates from 24% to 90%, when compared with periapical surgeries in isolation [3,16]. It is important to mention that the association between endodontic treatments and periapical surgery also removes chronically inflamed tissues, disinfects the root system canals, and promotes the formation of a fresh blood clot that increases the healing lesion site [3,15]. The latest choice treatment for AC is tooth extraction. This decision must be made after considering several factors, including tooth mobility, local and periapical lesion size, and systemic and oral health conditions [15,17,18].
As described above, the apical cyst is the most common type of lesion, representing from 7% to 54% of all cysts [19,20] but the presence of large cystic lesions in the anterior maxillary region is not reported frequently. Thus, in this case report, we described the history of a large apical cyst in the anterior region of the maxilla, the methods adopted for diagnosis, the treatment of choice, and the follow-up.
Case report
A healthy 60-year-old man showed up at the at the Oral and Maxillofacial Surgery and Traumatology division of the Centro Universitário do Norte de São Paulo (UNORTE) reporting the presence of an unobtrusive volumetric argumentation located in the anterior region of the maxilla, in the upper left central and lateral incisors and canine teeth (teeth 21,22,23, Figure 1A). The patient also reported that upper left and right central and lateral incisive teeth 12,11,21,22 had been submitted to endodontic therapy about 5 years prior (Figure 1B). The patient also mentioned the inability of tasting salty flavors, felt no pain or skin alterations, and his temperature seemed normal. The clinical exam (intraoral exam) only revealed a blend argumentation located in the anterior region of the maxilla, as described by the patient (Figure 1A). In addition, the digital pressure in the vestibular and/or lingual alveolar region did not show any suppuration in the tooth elements, and no alterations of color, size or morphology were observed in other regions of the oral cavity (Figure 1A). Percussion and vital tests were performed the teeth and no signals were detected.
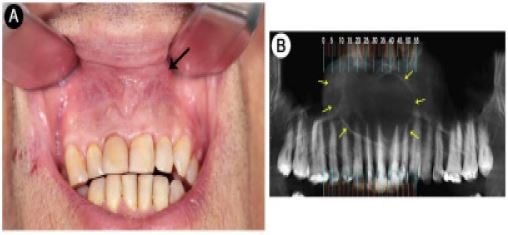
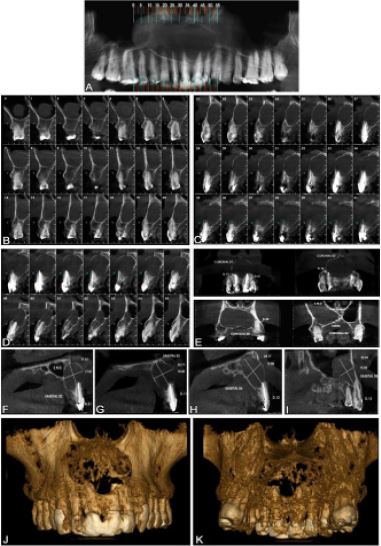
The first analysis of a radiographic face exam (panoramic exam) showed the presence of a circumscribed radiolucent area in the anterior region of the maxillary with extension from second high upper pre-molar teeth (15 tooth) to upper left canine (23 tooth) (Figure 1B), suggesting the presence of a cystic lesion in the anterior region of the maxillary, but the extensions and dimensions of the lesion were unclear (Figure 1B). In the same image exam, the anterior dental elements [teeth 11,12,21,22] were evaluated and alterations observed did not justify endodontic retreatment (Figure 1B). Thus, a tomographic exam was requested and showed the presence of a large hypodense lesion located in the anterior region of the maxillary with osteolytic, unilocular, and cystic characteristics (Figure 2B-2I). Vertically, the lesion extended from the periapical region of teeth 13, 12, 11, 21, and 22 to the floor of the nasal cavity (Figure 2E-2I). A 3D reconstruction showed bone resorption in the bilateral anterior region of the maxilla (Figure 2J-2K). After clinical and imaging exams, the hypothetical diagnosis of apical radicular cyst was confirmed. It is important to mention that the patient presented no systemic dysfunction at the time of anamnesis and no alterations were observed in complementary exams.
Treatment
Prior to surgery, we submitted the patient to a routine blood analysis, and conventional limits were verified. Thus, surgical enucleation of the cyst was chosen as the ideal clinical maneuver. For this, the patient was medicated with antibiotic prophylaxis (oral administration of 2 g of amoxicillin 60 minutes before the procedure, following the recommendations from the American Association of Endodontists [21]; Sanofi Medley Farmacêutica Ltda, Campinas, São Paulo, Brazil;), anti-inflammatory medication (oral administration of 8 mg dexamethasone 2 hours before the procedure; Teuto Brasileiro S.A, Anápolis, GO, Brazil following Alexander and Throndson, 2000 [22]), and underwent mouth rinsing with 0.12% chlorhexidine gluconate (Colgate-Palmolive Company, New York, New York, United States), extra oral disinfection with 10% povidin iodine (São José do Rio Preto, São Paulo, Brazil), and was applied with local anesthesia with 3% mepivacaine with 1:100,000 adrenaline (DFL Indústria e Comércio S/A, Rio de Janeiro, RJ, Brazil). An intraoral semilunar approach was performed on the anterior portion of the maxillary body as described by Ong et al. (2007) [23]. After that, no purulent secretion was observed emerging from the chirurgical access. At this moment, the AC was removed from the maxillary using the appropriate instruments. In addition, the cystic lesion was fixated in a 4% formaldehyde solution diluted in a 0.1M (pH 7.4) phosphate saline buffer and submitted to histopathological analysis (Lapat –Laboratório de Patologia Dr. Moriel, São José do Rio Preto, São Paulo, Brazil). Microscopy images showed the presence of lined non-keratinized stratified squamous epithelium, large fibroblasts in the wall of the cyst cavity with small blood vessels, and inflammatory infiltrates consistent with apical cyst as described by Myers et al. (1988) [24] and García et al. (2007) [25] (see the histopathological appraisal report in supplementary material). After surgical produces were finished, an acellular biological membrane of bovine origin (Techgraft membrane, Baumer S.A., Mogi Mirim, São Paulo, Brazil) was positioned on the surgical access and the soft tissues were sutured with 4.0 surgical cotton line (Ethilon, New Brunswick, New Jersey, United States). Antibiotic (oral administration of 500 mg of amoxicillin, 8/8 hours for 7 days, Sanofi Medley Farmacêutica Ltda, Campinas, São Paulo, Brazil) and anti-inflammatory (oraladministration of 100 mg of nimesulide, 12/12 hours during 3 days, Eurofarma, São Paulo, São Paulo, Brazil) post-surgery therapies were indicated, as well as mouth rising with 0.12% chlorhexidine gluconate (Colgate-Palmolive Company, New York, New York, United States). It is important to mention that the patient agreed with the plan of treatment and signed a consent form before the surgery.
Results and follow-up
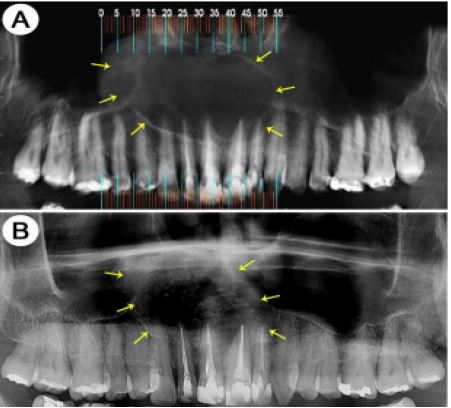
Clinical analyses after 7 days of surgical treatment showed good healing of soft tissues, and no pain or swelling. Radiographic examination after 11 months, approximately, showed that the region affected by the lesion presented good healing and signs of bone formation (Figure 3). There was no purulent secretion draining into the oral cavity after the intervention and the patient was completely asymptomatic after the surgical produces. A longer follow-up period is necessary to fully analyze the evolution of bone formation and the complete recovery of the injured area.
Discussion
In this study, we reported the presence of a large apical cyst in the maxillary anterior region. Apical Cysts (AC) are the most common odontogenic cysts observed in dental offices [1,26] and affect mostly 30-to-50-year-old males [27]. In the case presented here, we discussed the presence of an uncommon and large AC in a 60-year-old male patient and speculated that the AC could have started via the stimulation of epithelial cell rests of Malassez after an endodontic therapy involving the teeth 12, 11, 21, and 22. Cytokine secretions mediate this condition, as well as the presence of inflammatory cells, factor kappa-B ligand, and osteoprotegerin, which may promote the cystic expansion to the bone [28].
Apical cysts are frequently diagnosed during routine radiographic examinations and the prevalence of apical cysts is 60% higher in the maxilla than in the mandible [29]. Apical cysts are very small, reaching from 0.5 to 1.5 cm on average, with asymptomatic evolution and crepitations followed by erosion and an acute swelling fluctuation of the soft tissue. In the maxilla, sometimes, the cyst can be associated with molars or premolars and it encroaches on almost the entire sinus, and the residual sinus space may appear very thin [29]. Apical cysts are often connected with the root apex of a decayed or necrotic tooth pulp [30]. In radiographic analyses, the apical cysts appear as round or pear-shaped unilocular radiolucent shapes at the apex of necrosed tooth. Generally, the margins of these types of cysts are radiopaque hyperostotic borders that are continuous with the dental lamina dura. At this point, it is important to mention that chronic radicular cysts may cause resorption of tooth roots and cause several issues to the patient [30]. Besides that, this type of pathology can be confused with ameloblastoma, Pindborg tumors, odontogenic fibromas and cementomas, and may share the same radiological features as radicular cysts. Our patient’s history did not show unsuccessful non-surgical endodontic treatments in anterior teeth, nasal congestion, dizziness, and alterations in his sense of smell. Clinically, no swelling, pain, or dental mobility were observed on the right side of the face. Initially, the panoramic radiographic exam showed an undefined radiolucent region located in the apex of anterior and pre-molar teeth, suggesting the apical cystic lesion. At this moment, a tomographic exam was recommended to investigate the extension accurately, as well as the location and anatomical structures involved in the lesion. After that, a discrete opacification of airspace was observed within the right maxillary sinus, compatible with a large cyst (5 cm x 4 cm) located in the anterior maxillary region. It is important to mention that some types of radicular cysts can transform into squamous carcinomas, which is usually associated with long-standing cases [31-33]. In these cases, only good histophatological analyses can accurately diagnose the type of cystic lesion and discard the probable existence of tumors or other kinds of lesion that extend within the maxillary sinus.
Histological analysis of the enucleated cyst showed the presence of non keratinized stratified squamous epithelial and connective tissues with inflammatory infiltrates. This description corroborates Chen et al. (2018) [14], in whose study 98.3% of ACs presented non-keratinized stratified squamous epithelial tissues followed by mucoepidermoid epithelium, and the respiratory epithelium was present in 0.9% of the cases, while 0.4% have shown 226 epithelial lining dysplasia [14]. Thus, as described above, a histopathologic examination is crucial to determine cyst type accurately and provide a reliable diagnosis, which, in this case, was AC.
Several techniques have been described to treat large Apical Cysts (ACs), such as endodontic therapies with or without root canal medication, decompression, marsupialization, and cystectomy [3,34-36]. Among these techniques, the cystectomy is the complete enucleation of the lesion, considering the vital structures and allowing a reliable definite diagnosis through microscopy analysis [14,36]. The treatment of choice was determined by several factors such as the dental and medical history of the patient, his clinical aspects, anatomy features, hypothetic image diagnosis, and systemic health (according with Riviş and Văleanu, 2013 [37]). Many ACs can be treated with common endodontic therapies, but this treatment does not allow for a correct histopathological analysis of the cyst tissues, which may have malignant cell features [28]. In addition, a large cyst located in the anterior region of the maxillary with extension to the maxillary sinus can cause recurrent sinusitis [38,39]. Our patient did not relate nasal congestion, dizziness, and alterations in smell for several days, despite feeling uncomfortable with his current situation and wanting to solve his dental condition. Thus, the surgical intervention was selected as treatment. Finally, according to the patient’s desire, dental history, cyst extension, health condition, and probable image diagnosis, the chosen treatment was positive. As a result, with knowledge about cyst characteristics and respecting the biological principles of stomatognathic functions, the dental health of the patient was restored.
Conclusion and clinical relevance
Depending on the clinical case reported, several techniques can be adopted to deal with an apical cyst lesion, and patients should be informed about the complications and risks of each one. However, considering the patient’s health, the anatomic features of the region, dental history, and complementary exams, the cystectomy (enucleation) was chosen. In addition, knowledge about the anatomic structures, methods available, and local physiology is necessary to improve the patient’s health and deal with the case. Furthermore, histopathological analyses may be important for definite diagnoses and it be safety for dentist interventions.
In conclusion, large cystic lesions in males, occupying the anterior region of the maxilla with discrete extension to the maxillary sinus are extremely rare and seldom discussed among health professionals. Thus, radiographic imaging exams should be performed routinely in dental offices not only to look for common pathologies, since cysts can be asymptomatic. Early diagnosis and treatment are very important to avoid adverse effects in healthy teeth or other structures present in the face. Finally, when an uncommon pathology is analyzed, it is important to disseminate the knowledge acquired in its regard throughout the scientific community, so professionals can feel safer when caring for these issues.
Declarations
Ethical approval: This manuscript was approved by the patient and authors.
Declaration of competing interest: None.
Acknowledgments: We would like to thank Centro Universitário do Norte de São Paulo – UNORTE and the Chirurgical Department to perform the chirurgical techniques. We also to thank the Lapat – Laboratório de Patologia Dr. Moriel for carrying out the histological analysis.
References
- Hwang MJ, Lee YP, Lang MJ, Wu YH, Chiang CP, et al. Clinicopathological study of radicular cysts with actinomycosis. J Dent Sci. 2021; 16: 825-830.
- Bronzato JD, Davidian MES, de Castro M, de-Jesus-Soares A, Ferraz CCR, Almeida JFA, et al. Bacteria and virulence factors in periapical lesions associated with teeth following primary and secondary root canal treatment. Int Endod J. 2021; 54: 660-671.
- Karamifar K, Tondari A, Saghiri MA. Endodontic Periapical Lesion: An Overview on the Etiology, Diagnosis and Current Treatment Modalities. Eur Endod J. 2020; 5: 54-67.
- Ricucci D, Rôças IN, Hernández S, Siqueira JF Jr. “True” Versus “Bay” Apical Cysts: Clinical, Radiographic, Histopathologic, and Histobacteriologic Features. J Endod. 2020; 46: 1217-1227.
- Ramachandran Nair PN, Pajarola G, Schroeder HE. Types and incidence of human periapical lesions obtained with extracted teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 81: 93-102.
- Mupparapu M, Shi KJ, Ko E. Differential Diagnosis of Periapical Radiopacities and Radiolucencies. Dent Clin North Am 2020; 64: 163-189.
- Chybicki D, Lipczyńska Lewandowska M, Ratajek Gruda M, Janas Naze A. Massive Radicular Cyst in the Maxillary Sinus as a Result of Deciduous Molar Tooth Pulp Necrosis. Case Rep Dent. 2020.
- Couto AMD, Meirelles DP, Valeriano AT, Almeida DS, Moraes Ê, et al. Chronic inflammatory periapical diseases: A Brazilian multicenter study of 10,381 cases and literature review. Braz Oral Res. 2021; 35: e033.
- Galler KM, Weber M, Korkmaz Y, Widbiller M, Feuerer M. Inflammatory Response Mechanisms of the Dentine-Pulp Complex and the Periapical Tissues. Int J Mol Sci. 2021; 22: 1480.
- Biočanin V, Brajković D, Stevanović M, Tatić Z, Andrić M, et al. Decompression as an effective primary approach to large radicular cyst in the maxillary sinus -A case report. Vojnosanit Pregl. 2015; 72: 634-638.
- Levy DH, Dinur N, Becker T, Azizi H, Ben Itzhak J, et al. Use of Cone-beam Computed Tomography as a Critical Component in the Diagnosis of an Infected Nasopalatine Duct Cyst Mimicking Chronic Apical Abscess: A Case Report. J Endod. 2021; 47: 1177-1181.
- Savage NW, Adkins KF, Weir AV, Grundy GE. An histological study of cystic lesions following pulp therapy in deciduous molars. Journal of Oral Pathology and Medicine 1986; 15: 209–212.
- Schulz M, von Arx T, Altermatt HJ, Bosshardt, D. Histology of Periapical Lesions Obtained During Apical Surgery. J Endod 2009; 35: 634–642.
- Chen JH, Tseng CH, Wang WC, Chen CY, Chuang FH, et al. Clinicopathological analysis of radicular cysts of the jawbone in a population of southern Taiwanese patients. Kaohsiung J Med Sci. 2018; 34: 249-254.
- Von Arx T. Apical surgery: A review of current techniques and outcome. Saudi Dent J. 2011; 23: 9-15.
- Grung B, Molven O, Halse A. Periapical surgery in a Norwegian county hospital: Follow-up findings of 477 teeth. J Endod. 1990; 16: 411–417.
- Nica D, Ianes E, Brad S. CBCT fine preoperative evaluation of inflammatory radicular cysts and postoperative local integration appreciation of alloplastic grafts materials. Rev Med Chir Soc Med Nat Iasi. 2014; 118: 828-832.
- Huh JK, Yang DK, Jeon KJ, Shin SJ. Progression of periapical cystic lesion after incomplete endodontic treatment. Restor Dent Endod. 2016; 41: 137-142.
- Toomarian L, Moshref M, Mirkarimi M, Lotfi A, Beheshti M, et al. Radicular cyst associated with a primary first molar: A case report. J Dent (Tehran). 2011; 8: 213-217.
- Mahesh BS, Shastry S, Murthy P, Jyotsna TR. Role of cone beam computed tomography in evaluation of radicular cyst mimicking dentigerous cyst in a 7-year-old child: A case report and literature review. Int J Clin Pediatr Dent. 2017; 10: 213-216.
- https://f3f142zs0k2w1kg84k5p9i1o-wpengine.netdna-ssl.com/specialty/wp341 content/uploads/sites/2/2017/06/aae_systemic-antibiotics.pdf
- Alexander RE, Throndson RR. A review of perioperative corticosteroid use in dentoalveolar surgery. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90: 406-415.
- Ong JC, De Silva RK, Tong DC. Retrieval of a root fragment from the maxillary sinus--an appreciation of the Caldwell-Luc procedure. N Z Dent J. 2007; 103: 14-16.
- Myers DR, Durham LC, Hanes CM, Barenie JT, McKinney RV, et al. Histopathology of radiolucent furcation lesions associated with pulpotomy treated primary molars. Pediatr Dent. 1988; 10: 291–294.
- García CC, Sempere FV, Diago MP, Bowen EM. The post-endodontic periapical lesion: histologic and etiopathogenic aspects. Med Oral Patol Oral Cir Bucal. 2007; 12: 585-590.
- Ricucci D, Mannocci F, Ford TR. A study of periapical lesions correlating the presence of a radiopaque lamina with histological findings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 101: 389-394.
- Joshi NS, Sujan SG, Rachappa MM. An unusual case report of bilateral mandibular radicular cysts. Contemp Clin Dent. 2011; 2: 59-62.
- Nik Abdul Ghani NR, Abdul Hamid NF, Karobari MI. Tunnel’ radicular cyst and its management with root canal treatment and periapical surgery: A case report. Clin Case Rep. 2020; 8: 1387-1391.
- Deshmukh J, Shrivastava R, Bharath KP, Mallikarjuna R. Giant radicular cyst of the maxilla. Case Reports. 2014; bcr2014203678.
- Pekiner FZ, Borahan O, Ugurlu F, Horasan S, Cem Şener B, et al. Clinical and radiological features of a large radicular cyst involving the entire maxillary sinus. J Marmara Univ Inst Health Scien. 2012; 2: 31-36.
- Kay LW, Kramer IR. Squamous-cell carcinoma arising in a dental cyst. Oral Surg Oral Med Oral Pathol. 1962; 15: 970-979.
- Swinson BD, Jerjes W, Thomas GJ. Squamous cell carcinoma arising in a residual odontogenic cyst: case report. J Oral Maxillofac Surg. 2005; 63: 1231-1233.
- Kolari V, Rao HTA, Thomas T. Maxillary and mandibular unusually large radicular cyst: A rare case report. Natl J Maxillofac Surg. 2019; 10: 270-273.
- Fernandes M, De Ataide I. Non-surgical management of a large periapical lesion using a simple aspiration technique: A case report. Int Endod J. 2010; 43: 536-542.
- Santos Soares SM, Brito-Júnior M, de Souza FK, Zastrow EV, Cunha CO, et al. Management of Cyst-like Periapical Lesions by Orthograde Decompression and Long-term Calcium Hydroxide/Chlorhexidine Intracanal Dressing: A Case Series. J Endod. 2016; 42: 1135-1141.
- Talpos-Niculescu RM, Popa M, Rusu LC, Pricop MO, Nica LM, Talpos Niculescu S. Conservative Approach in the Management of Large Periapical Cyst-Like Lesions. A Report of Two Cases. Medicina (Kaunas). 2021; 57: 497.
- Riviş M, Văleanu AN. Giant maxillary cyst with intrasinusal evolution. Rom J Morphol Embryol. 2013; 54: 889-892.
- Bell GW, Joshi BB, Macleod RI. Maxillary sinus disease: Diagnosis and treatment. Br Dent J 2011; 210: 113-118.
- Psillas G, Papaioannou D, Petsali S, Dimas GG, Constantinidis J, et al. Odontogenic maxillary sinusitis: A comprehensive review. J Dent Sci. 2021; 16: 474-481.