
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Cervical lymph node metastasis from a remote
primary site with an airway emergency
Ambreen Abdullah Unar1; Muhammad Ozair Awan2; Haissan Iftikhar3*; Muhammad Sohail Awan4
1ENT Department, Aga Khan University Hospital, Karachi, Pakistan.
2Aga Khan University, Karachi, Pakistan.
3University Hospital Birmingham, Birmingham, UK.
4ENT Department, Aga Khan University Hospital, Karachi, Pakistan.
*Corresponding Author : Haissan Iftikhar
Epidemiology and Biostatistics Fellow Anterior Skull Base, University Hospital Birmingham, Birmingham, UK.
Phone: +92-334-5292533;
Email: haissaniftikhar@gmail.com
ORCID ID: 0000-0003-3266-4015
Received : Aug 17, 2022
Accepted : Sep 06, 2022
Published : Sep 13, 2022
Archived : www.jcimcr.org
Copyright : © Iftikhar H (2022).
Abstract
Cervical lymphadenopathy usually represents lymphomas or metastasis from head and neck primary tumors, but it can also occasionally be a manifestation of a remote primary site. PET-CT has improved identification of the location of such unknown primaries, particularly when they are distant in location. The mechanism, however, of head and neck metastases from many of these distant primary tumours remains obscure as there are often no obvious lymphatic pathways to explain their mode of spread. Cervical metastatic disease from a remote primary is often incurable and becomes even more challenging when the airway is compromised. Management of these cases is quite difficult and requires a multidisciplinary team. We report a rare case of a 45-year-old patient with a neck swelling and threatened airway due to metastatic breast cancer. The prognosis of breast cancer with distant metastases to the head and neck is generally poor, and the management of these lesions is controversial. Overall extent of the disease and individual patient prognosis must guide these treatment decisions.
Citation: Unar AA, Awan MO, Iftikhar H, Awan MS. Cervical lymph node metastasis from a remote primary site with an airway emergency. J Clin Images Med Case Rep. 2022; 3(9): 2048.
Introduction
Metastasis from an infraclavicular breast carcinoma to the cervical lymph node basin is a rare presentation, and for such a lesion to cause an airway distress is even more unusual. Approximately 1% of all cancers from the base of the skull to the thoracic inlet are metastases from a remote primary site and among these malignancies the frequently involved sites are the breast, lung, gastrointestinal tract, genitourinary tract, and uncommonly, the central nervous system [1]. Around 1% of all breast cancers are reported in men [2] and all of the histologic types of carcinomas identified in the female breast have been encountered in males as well, with ductal carcinomas being the most common due to the absence of a lobular system in the male breast [2]. Involvement of the lymphatics above the clavicular region and metastasis to the mandibular and the maxillary bone are the most common presentations of metastatic breast cancers to the head and neck region [3,4]. The prognosis of metastatic breast cancer is not good, and its management is controversial. In this paper, we report a are case of a 45-year-old male with a swelling in the neck, secondary to metastatic breast cancer, that caused an airway emergency.
Case
A 45-year male patient with a history of smoking presented to the emergency department with a progressive neck swelling for several months and significant difficulty in breathing for the past one month maintaining 96% saturation on 5 L of oxygen. On examination, the patient had a large right sided neck mass approximately 6 x 8 cm. The mass was firm to hard in consistency and fixed to underlying tissue with the overlying skin uninvolved. There were no tracheal landmarks palpable on further examination. A fiberopticlaryngoscope examination was carried out which revealed supraglottic edema as well as a medial bulge onthe lateral pharyngeal wall with an inability to visualize the true vocal folds. The patient’s voice was reported to be normal, and the rest of the ENT examination was unremarkable.
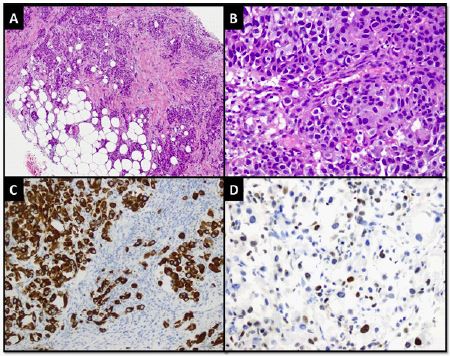
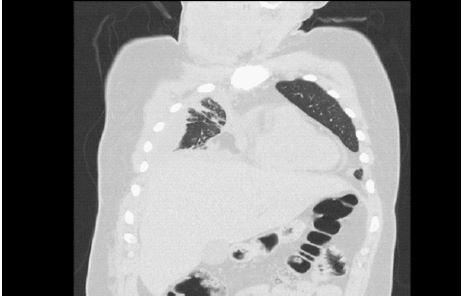
Initially a trucut biopsy of the neck mass was performed. Microscopic examination revealed linear cores of a neoplastic lesion infiltrating into the fibro-collagenous and adipose tissue. The tumour was arranged in nests of epithelioid cells without lumen formation. These cells had a moderate amount of lightly eosinophilic cytoplasm and moderate to markedly pleomorphic, vesicular nuclei with frequently visible nucleoli and mitotic figures. In addition, the neoplastic cells demonstrated positive expression for Cytokeratin CAM5.2, Cytokeratin 7, and GATA-3 Immunohistochemical (IHC) stains (Figure 1). However, Cytokeratin 20, p63, TTF-1, PAX-8, and CDX-2 IHC stains were found to be negative in the tumour cells. Moreover, the cells demonstrated negative expression for oestrogen, progesterone and Her 2/neu receptors. PET-CT scan revealed a mass in the neck involving the thyroid and measuring 6.4 x 7.6 x 6.8 cm (SUVmax = 21.3) as well as lymph node in the root of the neck on same side and lymph node in the right para tracheal region and carina (SUVmax = 9.7). In addition, right sided pleural thickening was seen in the right hemi thorax (SUVmax = 10.0) which showed lobulated effusion. Also seen was a lesion in the left acetabular roof (SUV = 6.7) and T9 (SUV = 5.3), reported as a lesion in the neck, chest, and bone secondary to IDC (Figures 2 & 3). The patient had no palpable breast masses however, the family history was positive for malignancies with the patient’s father diseased due to leukaemia and mother currently a patient of acute T cell lymphocytic leukaemia.
Worsening respiration and audible difficulty in breathing prompted us to advise the patient to undergo tracheostomy however, the patient. Thus, given the critical nature of the illness and the patient’s desire for a less aggressive palliative approach, a DNR was signed by the patient. Subsequently, the patient then expired two weeks after presenting to the emergency room.

Discussion
The mechanism of head and neck metastases from many of these distant primary tumours remains obscure as there are often no obvious lymphatic pathways to explain their mode of spread. However, current literature still notes that there is a predilection for such metastases for the left side of the neck [5]. Anatomy of the thoracic duct might explain this route of spread as it starts from the level of T12 at the confluence of cisterna chilli just below the diaphragm and ascends upward to level IV of the neck [6]. At the junction of the left subclavian and internal jugular veins, the thoracic duct drains into the systemic circulation resulting in the formation of the brachiocephalic vein. Therefore, lymphatic flow towards the left neck starts in the superior mediastinum with afferent drainage from the thorax, abdomen, liver, and pelvis to the lymphatics above the left clavicle to the left supraclavicular node known as Virchow’s node as described by Virchow and Trouser in the 19th century [7]. Obstruction inflow of lymph drainage belowthe left level IV to level VII of the neck may allow spread in a retrograde direction which can also involvethe superior or contralateral neck nodes. Involvement of nodes on the right side of the neck, however, may be associated with more advanced mediastinal involvement [5].
The neck lymph nodes commonly involved by distant primary tumours are the supraclavicular lymph nodes while metastases to the jugulodigastric chain are extraordinarily rare events [8]. Cervical lymphadenopathy from a distant primary can occurages after the primary tumour as well however, the involvement of supraclavicular lymph nodes should also alert the surgeon to the possibility of infraclavicular primary cancers [5]. Approximately 1% of all cancers from the base of the skull to the thoracic inlet are metastases from a remote primary site and among these malignancies the frequently involved sites are the breast, lung, gastrointestinal tract, genitourinary tract, and uncommonly, the central nervous system [4,8]. Although distant metastasis is comparatively common in breast cancer, spread to the head and neck region is still uncommon and can pose a diagnostic challenge to the head and neck surgeon [4]. The reported incidence of cervical metastases from breast carcinoma in current literature is around 2.3% to 4.3% [9]. According to the current revised version of the American Joint Committee on Cancer Staging System for Breast Cancer and the current classification of the International Union Against Cancer, lymph node metastases in the supraclavicular region are classified as pN3c (metastases in ipsilateral supraclavicular lymph nodes). This classification also states that these cancers are considered stage IIIC (any T, N3, or M0) if no distant metastases are present [10]. Being the most common breast cancer in males due to the absence of a lobular system in the male breast, there are multiple tools for the diagnosis of invasive ductal carcinoma including imaging and histopathology evaluation. These tools are digital mammography, ultrasound, MRI, and staging workup and pathology. The management of these patients is controversial but generally the treatment strategy would include surgery with or without breast reconstruction followed by chemotherapy or targeted molecular therapy, radiotherapy, and other hormonal therapy.
Lung cancer is another distant primary tumor that has been known to metastasize in the cervical region [10]. In addition, the incidence reported in literature for involvement of neck nodes from esophageal carcinomas is 20% to 30% approximately [7]. However, the role of cervical lymphadenectomy for oesophageal squamous cell carcinoma remains controversial.
Dixon et. al. [11] described clinical and pathological features of 25 patients with metastatic breast carcinoma to the head and neck region in their study. The authors concluded that the time of primary diagnosis to head and neck metastasis was highly variable ranging from 1 to 33 months with a mean of 10.9 years. Furthermore, they reported that the most common location for head and neck metastases were neck nodes (8 cases), orbital soft tissue (5 cases), oral cavity (3 cases), skull base (3 cases), mastoid sinus (2 cases), nasal cavity (1 case), palatine tonsil (1 case), and fascial skin (1 case). Bone is reported to be the most common site for distant metastasis of breast carcinoma after lungs with an apparent predilection to the mandible and maxilla but there is only one case of metastatic breast cancer reported in current literature involving the musculature of the head and neck region. Hirschberg et al. [3] retrospectively reviewed metastatic tumours to the head and neck cancers and concluded that breast cancers are the most common source of metastatic tumours to the jaw bone whereas lungs are the most common source for soft tissue metastasis to the head and neck region [3]. Supraclavicular nodal involvement of infraclavicular cancers generally have poor prognosis [8]. The median survival in most series is reported to be 6 to 15 months depending on patient and disease related factors [12]. Differentials of supraclavicular lymphadenopathy are broad and include benign lymphadenopathy, congenital cysts, tumours as well as infectious aetiology.
The diagnostic tools for cervical metastasis are ultrasound and FNAC. These tools are even helpful in clinically negative necks. However, the tissue obtained from cytology may be not sufficient for molecular testing. Other techniques such as core biopsies and excisional biopsies may become necessary if molecular testing is required. Typically, these metastases are challenging to assess with computed tomography due to the density with adjacent musculature and thus may be more properly distinguished with an MRI or FDG PET-CT [13]. Unfortunately, metastatic breast cancers still have a poor prognosis despite the advent of newer systemic therapies in the last decade [12].
Surgical management of difficult airway is of paramount importance in such patients. Treatment options to achieve airway patency include emergency tracheostomy, LASER therapy, contact electrocautery, argon plasm coagulation, photodynamic therapy, cryotherapy, brachytherapy, and airway stenting [14]. A team of doctors including anaesthetists, intensivists, surgeons, medical oncologists, and radiation oncologists is essential in delivering the most appropriate intervention in these cases.
Cervical lymphadenectomy may be indicated in select cases of distant primaries. The involvement of lymph nodes above the clavicle in breast and lung cancers (stage III disease) is important to note asin such casesloco-regional therapy can be considered but only with a curative intent [8]. In cervical oesophageal cancers, neck lymphadenectomy has shown good results [15]. In other cancers, however, there is no current reported evidence to support therapeutic neck dissection. Limited excision of the resectable neck disease may benefit patient in reducing local symptoms.
Conclusion
Metastatic cervical nodes usually originate from the head and neck primary tumour, however, lymphadenopathy in the inferior neck should alert the surgeon to the possibility of disease from a remote primary. This case illustrates a unique presentation of metastatic breast cancer presenting as a neck swelling which resulted in airway compromise ultimately leading to expiry of the patient due to development of imminent respiratory failure. A wide variety of treatment options are available to patients with an airway compromise secondary to malignancy however, it is imperative that these therapies coincide with the goals of care.
Declarations
Author contributions: AAU: Study Conception, Study Design Literature Review. MOA: Writing and Critical Review. HI: Analysis, Interpretation and Critical Review. MSA: Supervision, Guarantor and Critical Review.
Funding: No funding to declare.
Ethical approval and patient consent was taken prior to beginning work on the study.
References
- Tracy JC, Mildenhall NR, Wein RO, O’Leary MA. Breast cancer metastases to the head and neck: Case series and literature review. Ear, Nose & Throat Journal. 2017; 96: E21-E4.
- Barnes L. Metastases to the head and neck: An overview. Head and neck pathology. 2009; 3: 217-224.
- Hirshberg A, Buchner A. Metastatic tumours to the oral region. An overview. European Journal of Cancer Part B: Oral Oncology. 1995; 31: 355-360.
- Baum SH, Mohr C. Metastases from distant primary tumours on the head and neck: Clinical manifestation and diagnostics of 91 cases. Oral and maxillofacial surgery. 2018; 22: 119-128.
- López F, Rodrigo JP, Silver CE, Haigentz Jr M, Bishop JA, Strojan P, et al. Cervical lymph node metastases from remote primary tumor sites. Head & neck. 2016; 38: E2374-E85.
- Riquet M, Barthes FLP, Souilamas R, Hidden G. Thoracic duct tributaries from intrathoracic organs. The Annals of thoracic surgery. 2002; 73: 892-898.
- Nakagawa S, Nishimaki T, Kosugi S, Ohashi M, Kanda T, et al. Cervical lymphadenectomy is beneficial for patients with carcinoma of the upper and mid-thoracic esophagus. Diseases of the Esophagus. 2003; 16: 4-8.
- Manoharan M, Satyanarayana D, Jeyarajah AR. Cervical lymphadenopathy–An unusual presentation of carcinoma of the cervix: A case report. Journal of Medical Case Reports. 2008; 2: 1-5.
- Olivotto IA, Chua B, Allan SJ, Speers CH, Chia S, et al. Long-term survival of patients with supraclavicular metastases at diagnosis of breast cancer. Journal of clinical oncology. 2003; 21: 851-854.
- Carlson ER, Reddi SP, Monteleone KL. Metastatic lung cancer of the neck: Report of 2 cases. Journal of oral and maxillofacial surgery. 2002; 60: 1057-1061.
- Dixon J, Page D, Anderson T, Lee D, Elton R, et al. Long‐term survivors after breast cancer. British journal of surgery. 1985; 72: 445-448.
- Güth U, Magaton I, Huang DJ, Fisher R, Schötzau A, Vetter M, et al. Primary and secondary distant metastatic breast cancer: Two sides of the same coin. The Breast. 2014; 23: 26-32.
- Emmering J, Vogel WV, Stokkel MP. Intramuscular metastases on FDG PET-CT: A review of the literature. Nuclear medicine communications. 2012; 33: 117-120.
- Breitenbücher A, Chhajed PN, Brutsche MH, Mordasini C, Schilter D, et al. Long-term follow-up and survival after UltraflexTM Stent insertion in the management of complex malignant airway stenoses. Respiration. 2008; 75: 443-449.
- Takashima T, Nakata B, Hatama M, Nomura S, Komoto M, Ishikawa T, et al. Gastric cancer with cervical lymph node metastasis as the first presentation: report of a case. International surgery. 2008; 93: 295-299.