
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare case of mammary analogue secretory carcinoma of the parotid gland; A diagnostic and management challenge
Ainulakbar Mughal1; Muhammad Ozair Awan2*; Aabiya Arif3; Muntazir Hussain4; Muhammad Wasif5; Mahum Zaidi6; Sabeeh Siddique7
1MBBS, Year 3 Resident, ENT Department, Aga Khan University Hospital, Karachi, Pakistan.
2A-Levels, Year 4 Medical Student, Aga Khan University Hospital, Karachi, Pakistan.
3FSC, Year 4 Medical Student, Ziauddin University, Karachi, Pakistan.
4MBBS, FCPS, Assistant Professor, Cancer Foundation Hospital, Karachi, Pakistan.
5MBBS, FCPS, Assistant Professor Ziauddin Hospital, Karachi, Pakistan.
6MBBS, FCPS, Assistant Professor Department of Radiology, Liaquat National Hospital, Karachi, Pakistan.
7MBBS, FCPS, Assistant Professor and Consultant Histopathologist, Department of Pathology, Aga Khan University Hospital, Karachi, Pakistan.
*Corresponding Author : Muhammad O Awan
Aga Khan University Hospital, Stadium Road, Karachi, Pakistan.
Email: ozair.awan@scholar.aku.edu.
Received : Aug 17, 2022
Accepted : Sep 06, 2022
Published : Sep 13, 2022
Archived : www.jcimcr.org
Copyright : © Awan MO (2022).
Abstract
Mammary Analogue Secretory Carcinomas (MASCs) are rare slow growing salivary gland tumors that mimic the histological and genetic features of secretory carcinoma, a rare tumor of the breast. In this article, we present the case of a 24-year-old woman diagnosed as a case of mammary analogue secretory carcinoma. The patient underwent left superficial parotidectomy to excise the parotid mass. A multilobulated solid cum cystic mass of around 60 x 50 mm was excised with clear margins with preservation of the facial nerve. The lesion demonstrated an infiltrative pattern extending beyond the capsule of the tumor and immunohistochemical stains were positive for Cytokeratin AE1/AE3, Cytokeratin 7, SOX-10, and Mammaglobin. Due to vague clinical presentation and lack of certain imaging, MASC is a challenging definitive diagnosis to make, and less than 100 cases of MASCs have been reported in existing literature and management guidelines for the tumor are not yet clearly defined. We aim to help improve upon the existing knowledge base by reporting this rare case and lay down future groundwork for larger studies involving MASCs.
Keywords: MASC: mammary analogue secretory carcinoma; Salivary gland malignancy; Parotid gland tumors; S-100; Mammaglobin.
Citation: Mughal A, Awan MO, Arif A, Hussain M, Wasif M, et al. A rare case of mammary analogue secretory carcinoma of the parotid gland; A diagnostic and management challenge. J Clin Images Med Case Rep. 2022; 3(9): 2049.
Introduction
Mammary Analogue Secretory Carcinomas (MASCs) are rare slow growing salivary gland tumors that mimic the histological and genetic features of secretory carcinoma, a rare tumor of the breast [1]. They were first described by Skalova et al. in 2010 after reviewing 16 salivary gland tumor cases, previously labelled as either acinic cell carcinoma or adenocarcinoma – not otherwise specified, and finding features similar to secretory carcinoma of the breast [2]. Characterized by the t(12;15) (q13;q25) translocation, MASCs are generally solitary and well circumscribed lesions and can be found in all age groups, including children and young adults, and typically involve the parotid region, but have been known to affect other locations in the head and neck region as well [1,3,4]. Due to its propensity to display histologic features, such as central nuclei in tumor cells or a pink granulated or vacuolated cytoplasm, typically found in relatively common salivary gland malignancies, MASCs were commonly misdiagnosed as adenocarcinomas – not otherwise specified and acinic cell carcinomas of the salivary glands [5]. Therefore, a significant number of MASC cases now reported in the literature are cases that have been reclassified following secondary review [6].
Immunohistochemistry is a very useful tool to help differentiate MASC from other tumors. Markers such as DOG1, PAS-D, S100 and mammaglobin are especially useful when used in conjunction to accurately identify MASC [7]. However, immunohistochemistry is utilized as a supportive tool only and confirmation of the diagnosis is made only by demonstrating the characteristic t(12;15)(q13;q25) translocation, which results in the fusion gene ETV6-NTRK3, with the ETV6 gene from chromosome 12 and the NTRK3 gene from chromosome 15 [1,4]. In total, less than 100 cases of MASCs have been reported in existing literature and management guidelines for the tumor are not yet clearly defined. In this article, we present the case of a 24-year-old woman who presented with a slow growing, painless lesion in the right pre-auricular region. Initially diagnosed as a salivary gland neoplasm, the final histopathology report revealed a mammary analogue secretory carcinoma.
Case presentation
A 24-year-old lady, resident of Karachi, presented to the ENT Clinic at Aga Khan University Hospital, Karachi with a history of left-sided painless preauricular lesion for the past 2 months. The lesion was rapidly increasing in size and had no aggravating or relieving factors. The patient denied any radiation exposure in the past and had no systemic signs or symptoms pointing towards an inflammatory or infectious disorder. There was no family history of cancers, and she had no addictions to tobacco or alcohol. On examination, there was a 4 x 5 cm diffuse swelling around the left preauricular region. The swelling was generally non-tender and firm but soft at some places on palpation. Oropharyngeal and ear examinations were normal and facial nerve function was intact. In addition to that there was no sensory deficit over the lesioned area.
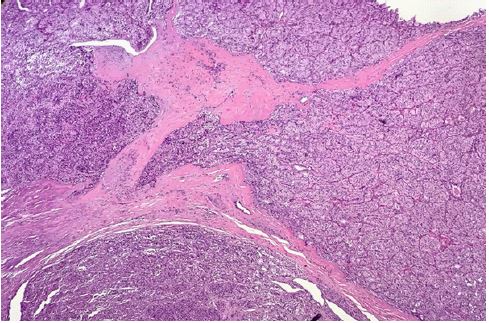
The patient underwent fine-needle aspiration subsequently which reported a suspicion for salivary gland neoplasm. On T1 weighted images, MRI demonstrated an irregular hypointense, multilobulated mass (51 x 37 x 40 mm) in the left parotid reinfiltrative pattern extending beyond the capsule of the tumor (Figure 1). Immunohistochemical stains were positive for Cytokeratin AE1/AE3, Cytokeratin 7, SOX-10, and Mammoglobin, and the diagnosis of MASC was established.
The patient’s case was discussed in the head and neck tumor board meeting, and it was decided to advise adjuvant radiation therapy. Subsequently the patient received 66Gy in 33 cycles. On 1-year-follow up the patient is doing well with no signs and/or symptoms of disease recurrence.
Discussion
A rare case of slow growing MASC of the left parotid gland is being reported in this article. Due to vague clinical presentation and lack of certain imaging, MASC is a challenging definitive diagnosis to make [8]. It typically presents as a slow growing lesion and affects both sexes’ equally. The age of onset is variable, and the disease is seen in both pediatric and adult demographics [8,9] with patients ranging in age from 14 to 77 years old. An average age of 45.7 years has been reported in existing literature [1,3,9]. MASCs are generally low-grade tumors with minimal recurrence rate and rare metastasis, but high-grade transformation and aggressive clinical characteristics have been witnessed and recorded on rare occasions, which manifests as recurrence, regional lymph node metastases, or even disease-related fatalities [1,3,4,6,8]. On gross appearance, MASCs may get misdiagnosed as a cystic mass, lymphangioma or a benign nodule.
In most cases, MASC seems to be a single, well-circumscribed, and encapsulated, dark or grey mass with a rubbery feel to it [6,8]. Histologically, the tumor islobulated with fibrous septa, and can have a cystic, tubular, solid, and/or papillary architecture [1], with the cystic or tubular areas containing bubbly or homogeneous secretions [1]. Cell atypia is not commonly seen howeversome tumor cells do appear transparent due to the presence of mucous [8]. MASC is a neoplasm with pale nuclei and eosinophilic vacuolated cytoplasm [8,10,11] and immunohistochemistry plays an important role in its diagnosis. Cells are found to be positive for Calcium binding S100 protein, Vim, muc-4, mammaglobin, and cytokeratin 7, 8, 18 and 19 [3,4,8].
The bulk of MASC research is based on a review of previously diagnosed salivary cancers [5]. These MASCs were formerly identified as adenocarcinomas, acinic cell carcinomas, low-grade mucoepidermoid carcinomas, or mucin-producing signet ring carcinomas [5,6,12]. The most common MASC misdiagnosis isacinus cell carcinoma, which is characterized by diastase PAS-resistant zymogen granules and an immunohistochemical profile that includes negative immunohistochemistry staining for mammaglobin and S100 [5,12]. In addition to that, both clinically and histologically, MASC can also mimic Pleomorphic Adenomas (PA). The main causes of PA misdiagnoses are the development of a sharply demarcated growth pattern, typically seen in MASC, and positive S100 immunohistochemistry staining with a histologically tubulo-cystic appearance [5,12]. However, PAs have been found to be negative for mammaglobin and/or muc-4, hence these markers can be used to rule out PA [12,13]. Adenocarcinoma not otherwise specified (adenocarcinoma NOS) is a diagnosis of exclusion that should be carefully evaluated since these tumors are high-grade neoplasms, and identification at biopsy may result in a more aggressive treatment strategy [14].
According to existing literature, in addition to primary tumor surgery, 26% of MASC patients also underwent lymph node dissection, 20% were given post-operative radiation and 2% were subjected to chemotherapy with radiation [15]. E. Boon et al in their study presented the data of 31 patients who underwent surgical removal as the initial treatment, and only those with involved or close surgical margins (n=15) underwent radiation post operatively [16]. They concluded that addressing the neck electively in surgery is not indicated. In addition to that, no differences in the rate of regional metastases are reported in minor or major salivary gland MASC [6] with an overall regional metastasis rate of 17.6% reported in literature. Sethi et al. in his review of 86 patients of MASC with treatment details on record, reported that 21 underwent neck dissection while 17 underwent radiation therapy and 2 underwent both radiation therapy and chemotherapy [1]. Therefore, addressing the neck is currently considered to be the surgeon’s decision based on the clinical assessment [1].
Declarations
Conflicts of interest: We have no conflict of interest.
Funding statement: No funding is involved.
References
- Sethi R, Kozin E, Remenschneider A, Meier J, VanderLaan P, et al. Mammary analogue secretory carcinoma: update on a new diagnosis of salivary gland malignancy. Laryngoscope. 2014; 124: 188–195. https://doi.org/10.1002/lary.24254.
- Skálová A, Vanecek T, Sima R, Laco J, Weinreb I, Perez Ordonez B, et al. Mammary analogue secretory carcinoma of salivary glands, containing the ETV6-NTRK3 fusion gene: A hitherto undescribed salivary gland tumor entity. Am J Surg Pathol. 2010; 34: 599–608. https://doi.org/10.1097/PAS.0b013e3181d9efcc.
- Bissinger O, Götz C, Kolk A, Bier HA, Agaimy A, Frenzel H, et al. Mammary analogue secretory carcinoma of salivary glands: diagnostic pitfall with distinct immunohistochemical profile and molecular features. Rare Tumors. 2017; 9: 7162. https://doi.org/10.4081/rt.2017.7162.
- Gaopande VL, Kulkarni MM, Khandeparkar SGS, Joshi AR. Mammary analog secretory carcinoma parotid gland: Case report of a recently described tumor with review of literature. Asian J Oncol. 2017; 03: 139–143.
- Quattlebaum SC, Roby B, Dishop MK, Said MS, Chan K, et al. A pediatric case of mammary analogue secretory carcinoma within the parotid. Am J Otolaryngol. 2015; 36: 741–743. https://doi.org/10.1016/j.amjoto.2015.05.005.
- Boliere C, Murphy J, Qaisi M, Manosca F, Fung H, et al. Mammary Analogue Secretory Carcinoma of the Palate: Case Report and Review of the Literature. Case Rep Dent. 2019; 2019: 7416302. https://doi.org/10.1155/2019/7416302.
- Khurram SA, Sultan Khan J, Atkey N, Speight PM. Cytogenetic and immunohistochemical characterization of mammary analogue secretory carcinoma of salivary glands. Oral Surg Oral Med Oral Pathol Oral Radiol. 2016; 122: 731–742. https://doi.org/10.1016/j.oooo.2016.07.008.
- Min FH, Li J, Tao BQ, Liu HM, Yang ZJ, Chang L, et al. Parotid mammary analogue secretory carcinoma: A case report and review of literature. World J Clin Cases. 2021; 9: 4052–4062. https://doi.org/10.12998/wjcc.v9.i16.4052.
- Hwang MJ, Wu PR, Chen CM, Chen CY, Chen CJ, et al. A rare malignancy of the parotid gland in a 13-year-old Taiwanese boy: Case report of a mammary analogue secretory carcinoma of the salivary gland with molecular study. Med Mol Morphol. 2014; 47: 57–61. https://doi.org/10.1007/s00795-013-0051-y.
- Alves LDB, de Melo AC, Farinha TA, de Lima Araujo LH, Thiago L de S, Dias FL, et al. A systematic review of secretory carcinoma of the salivary gland: where are we? Oral Surg Oral Med Oral Pathol Oral Radiol. 2021; 132: e143–e152. https://doi.org/10.1016/j.oooo.2020.04.007.
- Rodríguez Cobo J, Lazuén Fernández S, Mayorga Fernández MM, Gómez Román J, Freire Salinas J, Rodríguez Duque MS, et al. ETV6-NTRK3-positive parotid mammary analogue secretory carcinoma: a case report. Rom J Morphol Embryol = Rev Roum Morphol Embryol. 2021; 62: 309–312. https://doi.org/10.47162/RJME.62.1.34.
- Ito S, Ishida E, Skalova A, Matsuura K, Kumamoto H, Sato I, et al. Case report of Mammary Analog Secretory Carcinoma of the parotid gland. Pathol Int. 2012; 62: 149–152. https://doi.org/10.1111/j.1440-1827.2011.02759.x.
- Jung MJ, Song JS, Kim SY, Nam SY, Roh JL, Choi SH, et al. Finding and characterizing mammary analogue secretory carcinoma of the salivary gland. Korean J Pathol. 2013; 47: 36–43. https://doi.org/10.4132/KoreanJ Pathol.2013.47.1.36.
- Bishop JA, Yonescu R, Batista D, Eisele DW, Westra WH, et al. Most nonparotid “acinic cell carcinomas” represent mammary analog secretory carcinomas. Am J Surg Pathol 2013; 37: 1053–1057. https://doi.org/10.1097/PAS.0b013e3182841554.
- Salat H, Mumtaz R, Ikram M, Din NU. Mammary Analogue Secretory Carcinoma of the Parotid Gland: A Third World Country Perspective-A Case Series. Case Rep Otolaryngol. 2015; 2015: 697254. https://doi.org/10.1155/2015/697254.
- Boon E, Valstar MH, van der Graaf WTA, Bloemena E, Willems SM, Meeuwis CA, et al. Clinicopathological characteristics and outcome of 31 patients with ETV6-NTRK3 fusion gene confirmed (mammary analogue) secretory carcinoma of salivary glands. Oral Oncol. 2018; 82: 29–33. https://doi.org/10.1016/j.oraloncology.2018.04.022.