
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Aesthetic rehabilitation of secondary alveolar cleft with transpositional flap as a pre prosthetic procedure: A case report of an interdisciplinary approach
Nivedita A Rane1*; Abhishekh N Zingade2; Ritvik Ranka3; Shivani Kalloli3; Prabhanjan V Mulasavalgi1
1Private practitioners, MDS Periodontology from Department of Periodontics, KAHER’s V.K.Institute of Dental sciences, Belagavi, Karnataka, India.
2Reader, Department of Periodontics, KLE V.K. Institute of Dental Sciences, Belagavi, Karnataka, India.
3Private practitioners, MDS Prosthodontics from Department of Prosthodontics, KAHER’s V.K.Institute of Dental sciences, Belagavi, Karnataka, India.
4This case is affiliated to KAHER’s V.K. Institute of dental sciences, Department of Periodontics, Belagavi, Karnataka, India.
*Corresponding Author : Nivedita A Rane
Private practitioners, MDS Periodontology from Department of Periodontics, KAHER’s V.K.Institute of Dental sciences, Belagavi, Karnataka, India.
Email: nivedita.rane2991@gmail.com
Received : Aug 10, 2022
Accepted : Sep 07, 2022
Published : Sep 14, 2022
Archived : www.jcimcr.org
Copyright : © Rane NA (2022).
Abstract
Aesthetics is a major concern for patients suffering from cleft lip-palate, and equally challenging to a dentist when approached at a later stage for rehabilitation. Regenerative procedure involving use of bone grafts is advocated at a younger age, due to higher regenerative capacity and greater acceptance rate. However, increased chances of failure prevail in adults and the current techniques used involve use of grafts which increase treatment cost and patient morbidity.
Transpositional flap was introduced as a root coverage procedure and in following report of two cases we have described the application of this technique for correction of secondary alveolar cleft to bring about an improved soft tissue contour and aesthetic enhancement.
Keeping this in mind, to harmonize the pink with the white, an interdisciplinary approach was planned and executed for correction of secondary alveolar cleft and irregular gingival zeniths, which was followed by prosthetic rehabilitation.
The article describes the step-by-step surgical procedure which was carried out after completion of orthodontic treatment and discusses the prosthetic rehabilitation and post operative outcome after 3 months of follow-up.
Keywords: Secondary alveolar cleft; Transpositional flap; Aesthetic surgical procedure; Pre-prosthetic procedure.
Abbreviations: SAC: Secondary Alveolar cleft; SABG: Secondary Alveolar Bone Grafting; SCTG: Subepithelial Connective Tissue Graft; FGG: Free Gingival Graft.
Citation: Rane NA, Zingade AN, Ranka R, Kalloli S, Mulasavalgi PV. Aesthetic rehabilitation of secondary alveolar cleft with transpositional flap as a pre prosthetic procedure: A case report of an interdisciplinary approach. J Clin Images Med Case Rep. 2022; 3(9): 2050.
Introduction
Oral clefts occur 1 in 750 live births, and patients born with cleft lip and palate often seek for treatment regarding compromised function as well as aesthetics. Practitioners have strived with various techniques to gain perfection in treating cleft patients, keeping in mind the patients comfort and the post-operative results [1].
Correction of cleft lip is advocated at 3-6 months of age and cleft palate during the growing period at 4-5 years or even at 11-12 years of age [2]. However, Secondary Alveolar Clefts (SAC) prevail in many of these cases, in which rehabilitation with autogenous grafts is advocated only after complete eruption of the permanent canines which allows for stabilization of the alveolus [3]. Although Secondary Alveolar Bone Grafting (SABG) and soft tissue augmentation with Subepithelial Connective Tissue Grafts (SCTG) and Free Gingival Graft (FGG) have been used for treatment of SAC, the related patient morbidity cannot be ignored.
In patients where bone growth and orthodontic treatment is complete, distance between the two segments of the alveolar ridge is minimal and SAC requires ridge repair solely for the reason of aesthetics as well as maintenance, there is no reason why these individuals should undergo an extensive surgical procedure when the function is not compromised. Taking the above facts into consideration, use of Transpositional flap was suggested to achieve coverage of the SAC rather than bone grafting in the two cases discussed in the current article.
Case presentation
Case 1
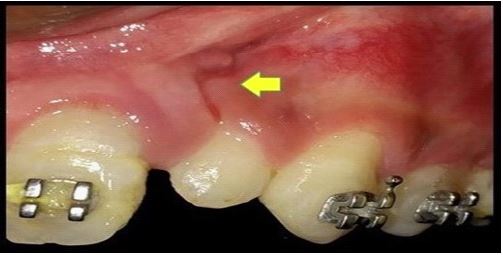
An 18-year-old male was referred to department of periodontics for pre-prosthetic treatment after completion of orthodontic treatment. Patient presented with rotated peg shaped laterals, uneven gingival zeniths and gingival cleft associated with 22 region. Spacing of 2 mm was seen between 21 and 22. Radiographic assessment showed presence of SAC between 21 and 22 (Figure 1). Hence the proposed treatment included correction of the gingival cleft associated with the SAC and gingival zeniths followed by prosthetic rehabilitation. The orthodontic treatment made it possible to align 22 such that the soft tissue associated with the SAC was supported by underlying tooth structure.

b. Radiograph showing presence of secondary alveolar cleft.
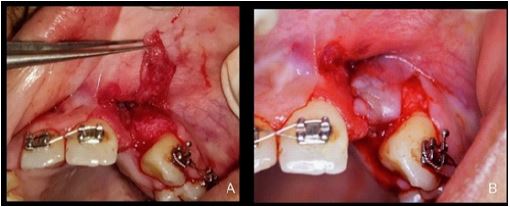
A thorough round of scaling and root planning was followed by the surgical procedure. In order to increase the mobility of the flap and to ensure that the defect was covered completely, the region of the pedicle flap was analysed and the recipient site, which included the tissue 5-6 mm around the defect was de-epithelialized using a 15 c blade up to the line angle of the adjacent mesial tooth (Figure 2). Full thickness parallel vertical incisions at the mesial and distal line angles of the tooth distal to the defect, demarcating extent of the pedicle flap were placed. The vertical incisions extended beyond the mucogingival junction into the labial mucosa. Although Bahatet al [4] advocated use of a full thickness pedicle flap, a partial thickness pedicle flap extending beyond the mucogingival junction, into the labial mucosa was carried out in order to ensure uncompromised blood supply at the donor site. Cut back incision was given on the disto-apical region of the flap at 100 degrees in on displacing the flap to the recipient site. The thickness at the base was 1.5 to 2 mm which included the muscle attachments, thereby increasing the vascular supply to the flap.
The edge of the flap was advanced and sutured with 5-0 Vicryl sutures at least 2 mm away from the defect taking into consideration that the papillary region and was approximated. The initial suture was placed through the advanced papillary end of the flap into the connective tissue bed. The second suture was placed perforating the mid flap region and approximating the flap as horizontal as possible to cover the defect. The remaining sutures were directed to approximate the flap margins over the de-epithelialized recipient bed (Figure 3).
Upon completion of suturing, light finger pressure was applied through a gauze to reduce bleeding as well as chances of hematoma or dead space formation, followed by placement of periodontal dressing (Coe-pak™, GC). Standard post-operative instructions were given and Tab. Augmentin 625 mg BID for 5 days, Tab. Aceclofenac 100mg BID for 3 days (after which the patient was advised to take analgesics on SOS basis) and Chlorhexidine mouth wash were prescribed. The dressing was removed after 7 days. Patient was recalled after 2 weeks for suture removal and correction of irregular gingival zeniths by gingivectomy procedure, which was followed by prosthetic rehabilitation.
For prosthetic rehabilitation, veneers for central incisors and crowns for lateral incisors and canines were planned. The crowns were prepared with a shoulder finish line to provide sufficient thickness for the ceramic. Incisal overlap preparation was chosen to give the dental technician maximum control over aesthetic characteristics and translucency (Figures 4,5,6).
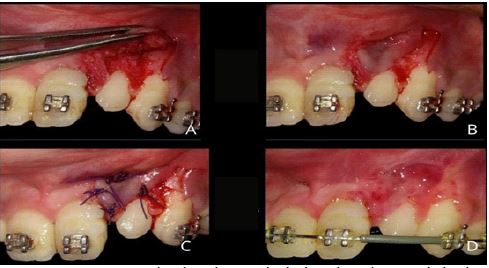
B. Cut back incision given to increase flaps mobility. C. Sutures placed.
D. Two weeks post operative recall.



b. Final result after treatment completion.
Case 2
A 26-year-old female, presenting with a SAC was referred to the department of periodontics after completion of orthodontic treatment for pre-prosthetic correction of unequal gingival zeniths and management of SAC. A conservative approach for management of the same was planned before prosthetic rehabilitation.
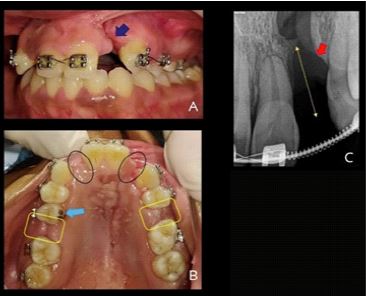
b. Pre-operative photograph showing missing 12,22,25. Spacing between 15-16, 24-26.
c. radiograph showing presence of secondary alveolar cleft.
b. Palatal recipient bed de-epithelialization.
Patient presented with congenitally missing 12 and 22, SAC in region of 22, Rotated 15, spacing between 15-16 and 25-26, unequal gingival zeniths, and occlusal discrepancy on left side (Figure 7). Treatment plan consisted of surgical correction of SAC with Transpositional flap and gingivectomy to correct the zeniths followed by prosthetic rehabilitation for aesthetic as well as occlusal correction.
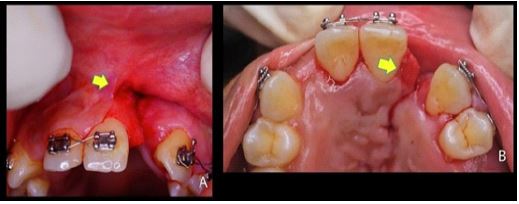
The recipient bed was de-epithelialized extending till the crest of the ridge and up to 3 mm on the palatal aspect (Figure 8). A partial thickness pedicle flap was raised distal to the defect extending beyond the mucogingival junction, followed by cut back incision at the base of the pedicle flap extending into the mucosa (Figure 9). The flap was approximated over the recipient site such that the crest as well as the palatal aspect of the defect were covered. The rest of the pedicle was approximated over the recipient bed and sutured (Figure 10). After application of light digital pressure over the area, surgical pack was placed, and post-operative medication were prescribed. Standard post-operative instructions were given.




b. Post-treatment photograph.
On recall visit, satisfactory healing at the surgical site, with complete closure of the SAC was observed (Figure 11). Correction of gingival zeniths was followed by prosthetic rehabilitation where crowns prepared with a shoulder finish line from 16-26 to provide sufficient thickness for the ceramic. Prosthesis were given as separate units from 13-23, 14-16 and 24-26 (Figure 12,13).
Prosthetic rehabilitation
Tooth Preparation was done using Diamond rotary instruments followed by impression with displacement cord and polyvinyl siloxane material. Shade selection was carried out using Vitapan Classical shade guide followed by immediate temporisation using dual cure composite material.
Lithium disilicate glass-ceramic (IPS e.max Press; Ivoclar Vivadent) laminate veneers and crowns were fabricated with the heat press technique and veneered with a layering ceramic (IPS e.max Ceram) to improve the appearance of the incisal edge. Veneers and crowns were both placed on teeth to evaluate the adaptation and colour followed by bonding of the restorations. Gingival and proximal excesses cement was removed followed by light polymerization with a light-emitting diode device (Radii-cal; SDI Ltd) for 60 seconds at the buccal, mesial, distal, and palatal aspects of each tooth. Restorations were then checked for occlusal interferences.
Discussion
Treatment of SAC is an integral component of the contemporary rehabilitation of patients with cleft lip and palate [5]. The options range from autogenous bone grafting to soft tissue augmentation depending on the availability of bone and connective tissue bed around it.
From an early introduction to recent times, several studies have shown that autogenous grafts is most preferred method for SAC grafting, as it not only supplies living, immunocompatible bone cells essential for osteogenesis, but also becomes fully integrated with the underlying bone [6,7]. Donor sites such as iliac crest, calvarium, mandibular symphysis and tibia are available for acquiring autogenous bone graft, of which iliac crest is considered as the gold standard due to its accessibility, ease to harvest, presence of abundant cancellous bone, and the fact that the defect is both well covered and not prone to pathological fracture [6-17]. However, the donor site also exhibits high morbidity with chronic pain, disability, haemorrhage, visible scar, contour deformity and sensory loss [18-21]. Also factors such as age, influence the final surgical outcome, since a greater failure rate has been observed with increasing age [22,23].
Agrawal et al [24] described treatment of SAC with combined use of sub-epithelial connective tissue graft and free gingival graft as an alternative to autogenous bone grafts for SABG with SAC. This helped to provide with necessary bulk to the tissue. As with any free gingival graft, although the initial colour matching may not be precise, long-term follow-up can show desirable aesthetics. However, patient morbidity related to secondary surgical site cannot be ignored.
Keeping in mind that in both the cases, an adequate connective tissue bed was available for tissue approximation, and the need for autogenous graft could be replaced with soft tissue augmentation procedures, Transpositional flap was carried out in order to cover the defect so that adequate coverage of the SAC and greater colour matching can be achieved. Both the cases showed desirable results at 1 week, 3 weeks 1 month and 3 months and 6 months post-operative recall. However, in Case 1, after 3 months, the patient exhibited papillary recession. This could be attributed to post-surgical shrinkage of tissue [25] and can be corrected in future with connective tissue graft papilla reconstruction procedure. However the patient decided to wait and watch. No changes were observed in Case 2 after 3 months.
Ceramic restorations offer a predictable and successful restoration with an estimated survival of more than 10 years [26]. In the presented situation for Case 1, veneers were planned for the central incisors keeping in mind the principle of dominance when it comes to smile designing. Therefore, minimum reduction of the central incisors was done. Due to the presence of inadequate crown structure on the lateral incisors, crowns were planned as veneers of excessive thickness would result in fracture of the ceramic. Also, crowns on canines and laterals would aid in compensation of the unequal distribution of space on both sides and give balance and symmetry to the smile. In Case 2, correction of spacing between the premolars and the molars on either side as well as correction of occlusion were added concerns along with giving the patient an aesthetic smile. Hence, crowns extending from 13-23, 14-16 and 24-26 were planned.
The dental preparations were restricted to the enamel when it came to veneers to acquire improved bonding. The restorative material for crowns and veneers used was a heat-pressed glass ceramic. For aesthetic veneers, leucite-reinforced and lithium disilicate glass ceramics are commonly selected because of their optical properties and good adhesion to tooth structure. They have a higher crystalline content than other ceramics and are less porous which provides adequate resistance to support anterior and lateral guidance. Because of the relatively low refractive index of leucite and lithium disilicate, even with a relatively high crystalline content, these materials are still sufficiently translucent to restore the incisal edge [27].
Conclusion
Transpositional flap can be considered as an option when rehabilitating SAC, when adequate soft tissue bed is present. The procedure not only reduces patient morbidity and gives aesthetic results, but also makes surgical rehabilitation an economical option for the patient. The final success of functional and/or aesthetic treatments is only achieved when the patient is well informed and motivated to maintain oral health. Patient contribution by oral hygiene maintenance and periodic control by the dentist is essential to the long-term success of the rehabilitation.
Acknowledgements: The author wishes to acknowledge Dr. Parthiban and Dr. Rahul Nachinolekar, Department of Orthodontics at KAHER’s V.K Institute of Dental Sciences for the orthodontic Rehabilitation of the patients.
References
- Sadove AM, Van Aalst JA, Culp JA. Cleft palate repair: art and issues. Clin plast surg. 2004; 31: 231-241.
- Sommerlad BC. Management of cleft lip and palate. Current Paediatrics. 1994; 4: 189-195.
- Boyne PJ, Sands NR. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg. 1972; 30: 87–92.
- Bahat O, Handlesman M, Gordon J. The transpositional flap in mucogingival surgery. Int J Periodontics Restorative Dent. 1990; 10: 473-483.
- Bergland O, Semb G, Abyholm FE. Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J. 1986; 23: 175-205.
- Sadove AM, Nelson CL, Eppley BL, Nguyen B. An evaluation of calvarial and iliac donor sites in alveolar cleft grafting. Cleft Palate J. 1990; 27: 225–228.
- Cho Lee GY, García Díez EM, Nunes RA, Martí Pagès C, Sieira Gil R, et al. Review of secondary alveolar cleft repair. Ann Maxillofac Surg. 2013; 3: 46-50.
- Boyne PJ, Sands NR. Secondary bone grafting of residual alveolar and palatal clefts. J Oral Surg. 1972; 30: 87–92.
- Canady JW, Zeitler DP, Thompson SA, Nicholas CD. Suitability of the iliac crest as a site for harvest of autogenous bone grafts. Cleft Palate Craniofac J. 1993; 30: 579–581.
- Cohen M. Harvesting iliac bone graft: Decreasing the morbidity. Cleft Palate Craniofac J. 2000; 37: 599.
- Enemark H, Jensen J, Bosch C. Mandibular bone graft material for reconstruction of alveolar clefts defects: Long-term results. Cleft Palate Craniofac J. 2001; 38: 155–163.
- Enemark H, Sindet Pedersen S, Bungaard M. Long term results after secondary bone grafting of alveolar clefts. J Oral Maxillofac Surg. 1987; 45: 913–919.
- Eufinger H, Leppanen H. Iliac crest donor site morbidity following open and closed methods of bone harvest for alveolar cleft osteoplasty. J Craniomaxillofac Surg. 2000; 28: 31–38.
- Sindet Pedersen S, Enemark H. Mandibular bone grafts for reconstruction of alveolar clefts. J Oral Maxillofac Surg. 1988; 46: 533–537.
- Sindet Pedersen S, Enemark H. Reconstruction of alveolar clefts with mandibular or iliac crest bone grafts: a comparative study. J Oral Maxillofac Surg. 1990; 48: 554–558.
- Stoelinga PJ, Haers PE, Leenen RJ, Soubry RJ, Blijdorp PA, Schoenaers JH, et al. Late management of secondarily grafted clefts. Int J Oral Maxillofac Surg. 1990; 19: 97–102.
- Cohen M, Figueroa AA, Haviv Y, Schafer ME, Aduss H, et al. Iliac versus cranial bone for secondary grafting of residual alveolar clefts. Plast Reconstr Surg. 1991; 87: 423–427.
- De la Torre JI, Tenenhaus M, Gallagher PM, Sachs SA. Harvesting iliac bone graft: Decreasing the morbidity. Cleft Palate Craniofac J. 1999; 36: 388–390.
- La Rossa D, Buchman S, Rothkopf DM, Mayro R, Randall P, et al. A comparison of iliac and cranial bone in secondary grafting of alveolar clefts. Plast Reconstr Surg. 1995; 96: 789–797.
- Laurie SW, Kaban LB, Mulliken JB, Murray JE. Donor-site morbidity after harvesting rib and iliac bone. Plast Reconstr Surg. 1984; 73: 933–938.
- Harsha BC, Turvey TA, Powers SK. Use of autogenous cranial bone grafts in maxillofacial surgery: a preliminary report. J Oral Maxillofac Surg. 1986; 44: 11–15.
- Jia YL, James DR, Mars M. Bilateral alveolar bone grafting: A report of 55 consecutively- treated patients. Eur J Orthod. 1998; 20: 299–307.
- Sindet-Pedersen S, Enemark H. Comparative study of secondary and late secondary bone-grafting in patients with residual cleft defects. Short-term evaluation. Int J Oral Surg. 1985; 14: 389–398.
- Agrawal A, Yeltiwar RK. Periodontal plastic surgery for management of cleft alveolar ridge: A case report. Int J Periodontics Restorative Dent. 2012; 32: 103-109.
- Pippi R. Post-Surgical Clinical Monitoring of Soft Tissue Wound Healing in Periodontal and Implant Surgery. Int. J. Med. Sci. 2017; 14: 721-728.
- Beier US, Kapferer I, Dumfahrt H. Clinical long-term evaluation and failure characteristics of 1,335 all-ceramic restorations. The Int J Prosthodont. 2012; 25: 70-78.
- Ritzberger C, Apel E, Höland W, Peschke A, Rheinberger V, et al. Properties and clinical application of three types of dental glass-ceramics and ceramics for CAD-CAM technologies. Materials (Basel). 2010; 3: 3700-3713.