
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Acute Carpal Tunnel syndrome from post-traumatic
pseudoaneurysm of the radial artery
John T Murphy*; Samuel B Hilton; Jeffery C Martin; Daniel E Krenk
Orthopedic Surgery Department, East Tennessee State University, USA.
*Corresponding Author : John Thomas Murphy
Orthopedic Surgery Department, East Tennessee State University, Johnson City, TN, USA.
Email: murphyjt@etsu.edu
Received : Aug 15, 2022
Accepted : Sep 08, 2022
Published : Sep 15, 2022
Archived : www.jcimcr.org
Copyright : © Murphy JT (2022).
Abstract
Introduction: Pseudoaneurysms are a well described complication of peripheral arteries. They often develop post-traumatically and/or iatrogenically. Prompt recognition with appropriate management is paramount in preventing limb-threatening complications.
Case report: We describe a case of acute Carpal Tunnel Syndrome (CTS) in a 66yo female after development of a pulsatile mass of her distal volar incision, 4 weeks status-post open reduction internal fixation of a comminuted distal radius fracture. Ultrasonography confirmed a 3 x 4 x 2 cm pseudoaneurysm of the radial artery. Emergent ligation of radial artery with pseudoaneurysm excision was performed, followed by urgent open carpal tunnel release.
Conclusion: Surgeons must maintain a high index of suspicion for pseudoaneurysms of peripheral arteries in patients with recent history of trauma and/or surgery of the area.
Citation: Murphy JT, Hilton SB, Martin JC, Krenk DE. Acute Carpal Tunnel syndrome from post-traumatic pseudoaneurysm of the radial artery. J Clin Images Med Case Rep. 2022; 3(9): 2053.
Introduction
An arterial pseudoaneurysm (false aneurysm), is caused by damage to the arterial wall resulting in a paravascular collection of blood, contained only by organized clot. This contrasts with a ‘true’ aneurysm which is a dilatation of a vessel involving all three layers (intima, media, adventitia) [1]. A pseudoaneurysmis characterized by turbulent blood flow and a neck that communicates with the parent vessel and typically will not close spontaneously once past a certain size. The formation of a peripheral pseudoaneurysm carries a risk of compression neuropathy, infection, thrombus formation or rupture [1-3].
Iatrogenic pseudoaneurysm of the radial artery is well-described and most often associated with arterial catheterization procedures [4]. Post-traumatic cases of radial artery pseudoaneurysms have also been described [6-8] although the incidence is unknown.
Here, we report a case of acute carpal tunnel syndrome from radial artery pseudoaneurysm in a posttraumatic case of an open distal radius fracture treated with dorsal spanning external fixator and subsequently open reduction internal fixation using a volar rim plate.
Case report
A 66-year-old female presented to our emergency department after a ground-level fall onto an outstretched right hand, tripping over a car jack. On exam, the patient was found to have a type I open, intra-articular distal radius fracture with 100% dorsal displacement and 90 degrees of dorsal angulation (Figure 1). The patient complained of paresthesias in the median nerve distribution on presentation, however this resolved after closed reduction in the emergency department. Due to the open nature of the injury, she underwent irrigation & debridement with placement of a dorsal spanning external fixator on the day of presentation (Figure 2). Four days later, she returned to the operating room for repeat incision and drainage and external fixator removal with open reduction internal fixa-tion of the distal radius fracture (Figures 3,4). A Synthes volar rim plate was used and the associated ulna fracture was treated conservatively.



The patient presented for her 2-week post-op visit complaining of pain and mildnumbness of the median nerve distribution since her surgery. Carpal tunnel release was discussed but the patient was adamant these paresthesias were overall improving since discharge. Her dorsal sutures were removed but the volar sutures left in place. No mass was noted, and patient was placed back into a splint with two pounds lifting restriction. She returned one week later for a wound check. At this visit, the numbness was confined to her volar thumb and index finger and her pain had improved significantly. There were no signs of infection. Remaining sutures were removed and 1 cm area of pulsatile swelling was noted at the distal, radial aspect of her volar incision. An ultrasound was ordered for patients’ right upper extremity to evaluate mass further. Seven days after this visit, patient had an ultrasound which revealed a 3 x 4 x 2 cm pseudoaneurysm of the radial artery. Bidirectional flow was noted and paresthesias in her median distribution had worsened.
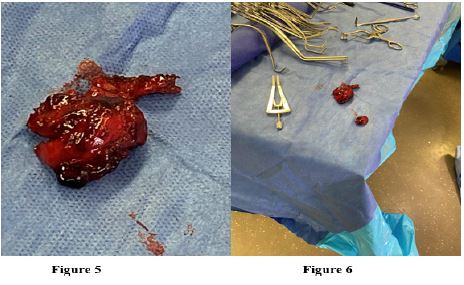
That same day, patient was taken to the operating room emergently for planned excision of pseudoaneurysm with end-to-end anastomosis of the radial artery. However, after excision of the pseudoaneurysm (Figures 5,6) the defect created was too large for direct primary repair. Instead, the patients’ radial artery was ligated with 3.0 silk ties. Doppler signals confirmed adequate blood flow to the hand after the ligation. At this point, under the same anesthesia, the orthopedic surgeon who fixed patients distal radius fracture performed an open carpal tunnel release.
Patient was subsequently discharged home on post-operative day 1 after the vascular excision and open carpal tunnel release. Her median nerve symptoms immediately resolved, and she has went on to heal the distal radius fracture without complication. Her hand remained well-perfused despite the radial artery ligation.
Discussion
Post-traumatic pseudoaneurysm of the radial arteryisa rare but potentially devastating complication. It is described most commonly in vascular literature after a catheterization procedure with a reported incidence of 1% [15]. In the orthopedic setting, it has been described to have occurred after open reduction internal fixation of a midshaft radius fracture, open reduction internal fixation of a distal radius fracture, forearm hardware removal and after conserva-tive therapy of trapezium & pisiform fractures [8,11,12,14]. To our knowledge, there has never been a case of acute carpal tunnel syndrome described as a result of mass effect from a post-traumatic pseudoaneurysm of the radial artery. There is however, cases described of acute carpal tunnel syndrome resulting after radial artery cannulation [9] and after radial line placement (with associated volar forearm compartment syndrome) [10].
In 2001, Chung et al. reported 1.5% of all emergency department presentations are due to hand/wrist fractures, of which 44% are fractures of the radius/ulna [13]. Given this incidence, it is prudent for the orthopedic surgeon to possess the clinical wherewithal to promptly recognize a post-traumatic pseudoaneurysm of the radial artery. A peripheral pseudoaneurysm will typically appear as a painful mass several days to months after the traumatic insult. The mass is usually pulsatile, although not universally. In the setting of small pseudoaneurysms, the mass may not be pulsatile or even palpable. This would leave the only presenting symptom as the subjective pain reported by the patient. Depending on size and location of the pseudoaneurysm, paresthesias may result from nerve compression. Mural thrombi formation at the pseudoaneurysm site can cause embolization distally with digital ischemia. Spontaneous rupture of a pseudoaneurysm has been described with associated overlying skin erosion [16] although this is a rare complication. Most uncomplicated cases can be diagnosed with ultrasonography. The Allen Test can be used to evaluate artery patency with the option of an magnetic resonance imaging if there is concern regarding collateral circulation and palmar arch function.
Small, asymptomatic pseudoaneurysms can be managed conservatively with observation, compression therapy or anticoagulation interruption. Ultrasound guided thrombin injection to treat post-catheterization pseudoaneurysm of the femoral artery has a 90% success rate [17]. However, this intervention is not accepted in the upper extremity due to risk of distal ischemia from embolization [18,19]. Symptomatic pseudoaneurysms over 10 mm in diameter are indicated for surgical intervention. If collateral circulation to the hand is insufficient, blood flow must be maintained. After excision of the pseudoaneurysm, end-to-end repair is used if the defect created is amenable to it. Venous graft interposition is used for larger defects where a primary anastomosis cannot be performed [20,21]. Finally, a ligation of the artery can be performed where a large defect is created, and adequate collateral circulation has been confirmed [20]. This was the case in our patient whose pseudoaneurysm measured 2.9 x 2.3 cm and collateral circulation was confirmed distally. Excision with ligation is also recommended in polytrauma patients with multiple other injuries, patients who cannot tolerate a prolonged procedure and in infected (mycotic) pseudoaneurysms [14].
Conclusion
Pseudoaneurysms form as a result of injury to the arterial wall and present as a painful, pulsatile mass. Iatrogenic injury is an important cause of peripheral pseudoaneurysms. Clinically, a high index of suspicion by surgeons can assure prompt recognition, appropriate diagnostic imaging and referral to a vascular surgeon. Furthermore, meticulous care and protection of peripheral arteries must be universally maintained.
References
- Cozzi DA, Morini F, Casati A, et al. Radial artery pseudoaneurysm successfully treated by compression bandage. Arch of Diseases in Childhood. 2003; 88: 65-166.
- Alerhand S, Apakama D, Nevel A, et al. Radial artery pseudoaneurysm diagnosed by point-of-care ultra-sound five days after transradial catheterization: A case report. World J Emerg Med. 2018; 9: 223-226.
- Ratschiller T, Müller H, Schachner T, Zierer A. Pseudoaneurysm of the Radial Artery After a Bicycle Fall. Vasc Endovascular Surg. 2018; 52: 395-397.
- Esposito G, Marone E, De Dominicis D, Tshomba Y, Chiesa R, et al. Hand and wrist arterial aneurysms. Annals of Vascular Surgery. 2006; 20: 512–517
- Journal of Hand Surgery. 2017; 42: 295-298.
- Nieddu ME. Post-traumatic aneurysm of the radial artery: A case report. J Ultrasound. 2012; 15: 174-175
- Narsete EM. Traumatic Aneurysm of the Radial Artery: A report of three cases. Am J Surgery. 1964; 108: 424-427.
- Dahapute A, Gala R, Sanjay B, Virani S, et al. Radial Artery Pseudoaneurysm in a Post-Operative Case of Midshaft Radius Fracture. J of Orthopedic Case Reports. 2017; 7: 3-5.
- Martin S., Sharrock N., et al. Acute Exacerbation of Carpal Tunnel Syndrome after Radial Artery Cannu-lation. J of Hand Surgery. 1993; 18: 455-458.
- Kokosis G, Blueschke G, Blanton M, et al. Acute Carpal Tunnel Syndrome secondary to Iatrogenic Hem-orrhage. A case report. Hand (NY). 2011; 6: 206-208.
- Fung BK, Ip WY. Pseudoaneurysm of the radial artery after plate removal. Hong Kong J Ortho Surg. 2001; 5: 138–140.
- Dao KD, Venn-Watson E, et al. Radial artery pseudoaneurysm complication from use of AO/ASIF volar distal radius plate: A case report. J Hand Surg Am. 2001; 26: 448–453.
- Chung KC, Spilson SV. The Frequency and Epidemiology of Hand & Forearm Fractures in the United States. J Hand Surg Am. 2001; 26: 908–915
- Ratschiller T, Muller H, et al. Pseudoaneurysm of the Radial Artery after a Bicycle Fall. Vasc and Endo-vascular Surgery. 2018; 52: 395–397
- Uhlemann M, Mobius-Winkler S, Mende M, et al. The Leipzig prospective vascular ultrasound registry in radial artery catheterization: Impact of sheath size on vascular complications. JACC Cardiovasc Interv. 2012; 5: 36-43
- Dey S, Baruah A, Mohanta PK. Ruptured pseudoaneurysm of the radial artery. BMJ Case Report 2009.
- Webber GW, Jang J, Gustavson S, Olin JW. Contemporary management of postcatheterization pseudoan-eurysms. Circulation. 2007; 115: 2666-2674.
- Herold J, Brucks S, Boenigk H, et al. Ultrasound guided thrombin injection of pseudoaneurysm of the ra-dial artery after percutaneous coronary intervention. VASA. 2011; 40: 78-81.
- D’Achille A, Sebben RA, Davies RP. Percutaneous ultrasoundguided thrombin injection for coagulation of post-traumatic pseudoaneurysms. Australas Radiol. 2001; 45: 218-221.
- Esposito G, Marone EM, De Dominicis D, Tshomba Y, Chiesa R, et al. Hand and wrist arterial aneurysms. Ann Vasc Surg. 2006; 20: 512-517.
- Turowski GA, Amjadi N, Sterling A, Thomson JG. Aneurysm of the radial artery following blunt trauma to the wrist. Ann Plast Surg. 1997; 38: 527-530.