
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Long-term durability of improved glycemic control in type 2 diabetes mellitus treated with dasatinib, a second-generation tyrosine kinase inhibitor, for chronic myeloid leukemia:
A report of two cases
Choka Azuma1; Masanori Iwanishi1; Yuji Tezuka1; Yukako Yamamoto1; Jun Ito Kobayashi1; Miki Washiyama1; Osamu Sekine1; Takuya Hino2; Akira Shimatsu1; Takayo Suzuki2; Atsunori Kashiwagi1*
1Department of Diabetes and Endocrinology, Omi Medical Center, 1660, Yabashe-cho, Kusatsu, Shiga 525-8585, Japan.
2Department of Hematology, Omi Medical Center, 1660, Yabashe-cho, Kusatsu, Shiga 525-8585, Japan.
*Corresponding Author : Atsunori Kashiwagi
Department of Diabetes and Endocrinology, Omi Medical Center, 1660, Yabashe-cho, Kusatsu, Shiga 525-8585, Japan.
Phone: (+81) 77-563-8866, Fax: (+81) 77-565-9313;
Email: kashiwagi@seikoukai-sc.or.jp
Received : Aug 22, 2022
Accepted : Sep 08, 2022
Published : Sep 15, 2022
Archived : www.jcimcr.org
Copyright : © Kashiwagi A (2022).
Abstract
Dasatinib, a second-generation tyrosine kinas inhibitoris effective against most cases of imatinib-resistant Chronic Myelogenous Leukemia (CML), and this drug has also shown significant glucose-lowering effects. Here, we report two diabetes patients with sudden onset of CML. In Case 1, dasatinib produced mild but clear improvement of hyperglycemia with the same anti-diabetic regimen together with rapid control of CML. In Case 2, initiation of dasatinib resulted inmarked potentiation of insulin-induced glucose-lowering effects in parallel with rapid improvements of CML. In both cases, this favorable diabetes control was well maintained for 5 years under leukemia management with dasatinib.
Keywords: Chronic myelogenous leukemia; Tyrosine kinase inhibitor; Dasatinib; Glycemic control; Type 2 diabetes mellitus.
Citation: Azuma C, Iwanishi M, Tezuka Y, Yamamoto Y, Kashiwagi A, et al. Long-term durability of improved glycemic control in type 2 diabetes mellitus treated with dasatinib, a second-generation tyrosine kinase inhibitor, for chronic myeloid leukemia: A report of two cases. J Clin Images Med Case Rep. 2022; 3(9): 2054.
Introduction
Chronic myelogenous leukemia (CML) is a myeloproliferative disorder associated with the so-called Philadelphia chromosome and/or the BCR-ABL1 (breakpoint cluster Region-Abelson) fusion gene. Tyrosine Kinase Inhibitors (TKIs) dramatically improve the prognosis of CML [1]. Dasatinib is a second-generation TKI that inhibits multiple family kinases including BCR-ABL, Src family kinases, receptor kinases, and Tec kinases [1]. Although the clinical outcome of CML treatment is markedly improved with the development of TKIs, these drugs have been associated with various adverse effects including metabolic abnormalities [3]. There are several reports that imatinib (a first-generation TKI) [4-6] and dasatinib (second-generation TKI) may ameliorate glycemic control [7-12], but that nilotinib (second-generation TKI) worsens fasting hyperglycemia with aggravation of insulin resistance and abnormal lipid metabolism [13,14]. In addition, there are some controversies regarding the glucose-lowing effects of dasatinib treatment in CML patients with Type 2 Diabetes Mellitus (T2DM). Those cases can show a marked glucose-lowering effect [7,8], a mild improvement of glycemic control [9,10], or conversely, a worsening of hyperglycemia in the chronic phase of dasatinib treatment [11]. Here, we report two T2DM cases with sudden CML onset, in whom both glycemic control and abatement of CML were well maintained through 5 years of dasatinib treatment without any increases in glucose-lowering drug doses.
Case reports
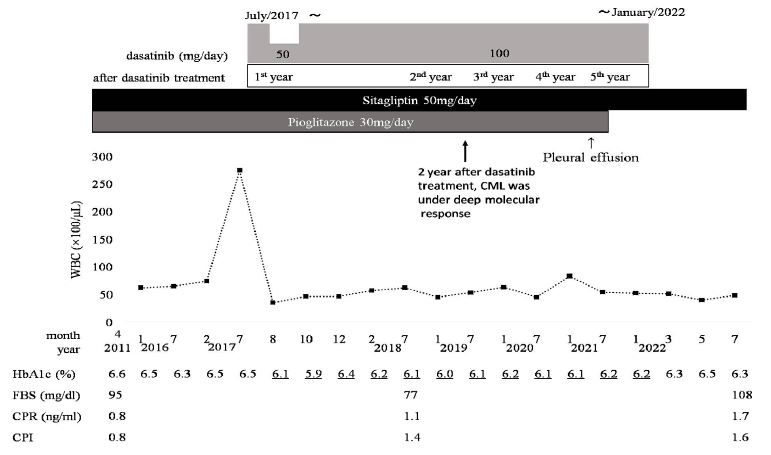
Case 1: A 55-year-old Japanese man with T2DM had maintained glycated hemoglobin (HbA1c) levels around 6.5% for 12 years using two daily oral hypoglycemic agents (50 mg sitagliptin and 30 mg pioglitazone). In early May, 2017, his White Blood Cell (WBC) count was found to be increased to 22,900/ μL with concomitant increases in the percentage of basophils and absolute numbers of undifferentiated myelocytes and myeloblasts while his blood chemistry showed elevated LDH and uric acid levels. The patient was normal weight (BMI 21.8 kg/m2) without any abnormal signs orsymptoms. A diagnosis of CML was made based on the presence of Philadelphia chromosome under FISH observation and excessive BCR-ABL mRNA as determined by RT-PCR. His clinical course is shown in Figure 1. Soon after beginning the administration of dasatinib (100 mg, once daily), his WBC counts rapidly normalized to yield a complete hematological response, and his HbA1c levels promptly deceased to around 6.1% with administration of both sitagliptin (100 mg/day) and pioglitazone (30 mg/day). At 2 years after initiation of dasatinib treatment, the CML status achieved a deep molecular response, namely BCR-ABL1IS=0.0013(MR4.5DMR) [15]. At this time, the C-Peptide Index (CPI), a marker of insulin secretory capacity, had increased to 1.4 from its pre-dasatinib level of 0.8. Furthermore, his HbA1c levels were maintained well under the same treatment for at least 5 years, despite the eventual discontinuation of pioglitazone due to increased risk for fluid retention starting July 2021. On January, 2022, the dasatinib treatment was also discontinued due to uncontrollable pleural fluid retention, a major side effect of TKIs. As a result, his HbA1c slightly rose to 6.3~6.5% during the following 6 months with a similar CPI level (1.6). However, the deep molecular response status of his CML was continuously maintained for 6 more months without the dasatinib treatment.
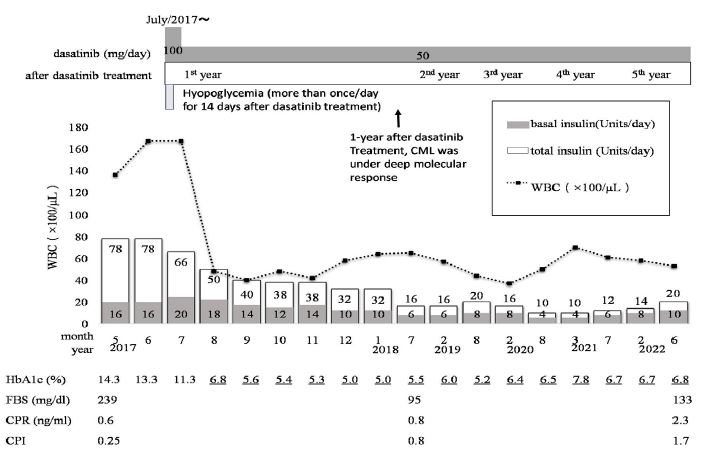
Case 2: A 48-year-old Japanese man with lean T2DM (BMI 20.5 kg/m2) had been diagnosed with diabetes 15 years prior. However, he had not been seen in clinic nor received treatment for the last three years. In early June 2017, his diabetes control had deteriorated to HbA1c of 14.3% with advanced diabetic nephropathy (Stage 3), simple diabetic retinopathy, and peripheral neuropathy. At the same time, a high WBC count (13,590/ μL), with high levels of basophils (8%) and immature myelocytes (1.0%) and high platelets (668,000/μL) were seen on his Complete Blood Cell counts (CBC). Further genetic investigation confirmed a diagnosis of CML. His hyperglycemia (HbA1c 14.3%, casual blood glucose 605 mg/dL) was immediately treated by intensive insulin therapy (16 units insulin glargine and 62 units ultrarapid insulin; total insulin dose 78 units/day). He was referred to our hospital for control of both CML and hyperglycemia. His clinical course is shown in Figure 2. The patient was immediately started on dasatinib (100 mg once daily) for CML control. Dasatinib was reduced to 50 mg/day one month later because of moderate fluid retention in both legs. Soon after the initiation of the dasatinib treatment, the patient developed frequent symptomatic hypoglycemia by initiation of the same dose of insulin used in the previous hospital, and insulin was titrated down. After 3 months of treatment, the total insulin dose had decreased to 38 units/day based on an HbA1c of 5.4%, and was further reduced to 16 units/day at 1 year based on a mean HbA1c of 5.5%. His WBC count quickly decreased to 4,800/μl after 1-month dasatinib treatment and was well maintained thereafter. At 1 year after initiation of dasatinib treatment, his CML achieved a deep molecular response status, namely BCR-ABL1IS=0.0009 (MR5.0 DMR) [15]. His CPI was increased to 0.8 at 1 year after initiation of treatment compared to a CPI of 0.25 before treatment. Both control of CML and diabetes in case 2 were also well maintained for 5 years with the same dose of dasatinib (50 mg/day). In early July 2022, his HbA1c (6.8%) and CPI level (1.7) were well maintained despite of insulin glargine 10 units once daily and ultra rapid insulin 10 units (total insulin dose 20 units/day), which was slightly increased because of a slight increase in HbA1c (7.8%) at March 2021.
Discussion
TKIs have dramatically improved the prognosis of CML, such that patients with CML on long-term TKI therapy now have a similar life expectancy to the general population [1]. Despite the overall favorable prognosis from TKIs, adverse events are also common in this treatment. Compared to imatinib, the second-generation TKIs have been reported to be potentially associated with harmful pulmonary, gastrointestinal, and metabolic complications in the chronic phase of CML therapy [1-3,16]. It has been pointed out that major determinants of adverse events of TKIs depend on drug type, age, ethnicity, and treatment duration [12]. In both of our cases, dasatinib therapy was selected from among many TKIs for treatment of CML mostly because of its having fewer negative impacts on patients with pre-existing medical conditions such as diabetes and cardiovascular disease [17]. Dasatinib, a second-generation TKI, is effective against most imatinib-resistant cases of CML, and this drug has a potential glucose-lowering effect, which of course held promise for our patients. However, there are some controversies regarding the potentiation of glucose-lowering effects of dasatinib. For example, a marked glucose-lowering effect [7,8], a mild improvement of glycemic control [9,10], and worsening of hyperglycemia in the chronic phase of CML treatment with dasatinib [11] have all been reported. Here we report two Japanese T2DM patients with sudden onset of CML, who showed mild and marked enhancements of glucose-lowering effects after dasatinib treatment, respectively.
A case with mild glucose-lowering effects of dasatinib: In Case 1, dasatinib showed mild glucose-lowering effects. Before treatment, the patient’s HbA1c was 6.6%, compared to an HbA1c of 6.1% at 1 month after dasatinib initiation; this response was comparable to that in a previous report [10] in which dasatinib treatment reduced HbA1c from 6.2% to 5.8% one month after treatment. We compared the CPI before and after dasatinib treatment to evaluate the drug’s effect specifically on insulin secretion. CPI increased from 0.8 prior to treatment to 1.4 after dasatinib treatment. In addition, both CML and glucose were well controlled for 5 years with relatively constant dosages of the two drugs. Ultimately, however, the dasatinib treatment had to be discontinued due to uncontrollable fluid retention. Six months later, a slight increase in HbA1c levels (6.3%) was seen with a further increase in CPI (1.6) under the deep molecular response of CML. This slight increase in HbA1c levels could be explained by a slight increase in postprandial hyperglycemia, since it was reported that HbA1c levels are more closely associated with postprandial glucose levels than with fasting glucose levels at HbA1c less than 7.3% [18]. In this patient, pioglitazone had to be discontinued due to a risk for further deterioration of fluid retention. This change might have led to a slight worsening of postprandial hyperglycemia.
Improvements in glycemic control occur by many mechanisms, as is evidenced by the many classes of drugs used to control hyperglycemia. In general, the improvement might come from improved secretion of insulin by the pancreatic β-cells, or improved insulin resistance (or both). In our case here, the improvement was at least accompanied by improved insulin secretion, as evidenced by the increased CPI. Two Homeostatic Model Assessment (HOMA) measures are used to distinguish between these mechanisms, and in one of the previous reports on diabetic CML patients [10], dasatinib showed an a mild improvement of insulin resistance (HOMA-IR) from 1.96 to 1.05 (normal, < 1.0, abnormal, ≥2.5) without a significant change in secretion (HOMA-β) from 48 to 43 (normal, 50~100) soon after dasatinib treatment [19]. The same study showed increases in patients’ plasma adiponectin and leptin levels after dasatinib treatment, supporting an increase in insulin sensitivity. Another study has also demonstrated increases in plasma adiponect in levels with imatinib treatment in T2DM patients with CML [20].
A case of marked potentiation of glucose-lowering effects of dasatinib: Our case 2 and two cases in previous reports [7,8] showed similar clinical characteristics: namely, dramatic worsening of glycemic control in the progression of CML. Food intakes of these patients were not affected by the CML progression and dasatinib treatment in our case 2 or in a previous Japanese case [7] reported by Ono et al. The aggravated diabetic conditions were treated with intensive insulin treatment including multiple bolus injections before every meal and one shot of baseline insulin injection. Our case initially required total 78 units insulin/day. Soon after initiation of dasatinib treatment, both our case and Ono’s showed rapid hematologic responses with normalization of basophilia and WBC counts. In parallel with the hematological response, poor glycemic control was quickly ameliorated with a marked potentiation of glucose-lowering effects, as demonstrated by frequent symptomatic hypoglycemia requiring down-titration of the insulin dose. Our case improved insulin secretion, as demonstrated by an improvement in CPI from 0.25 before treatment to 0.8 at 1 year after dasatinib initiation. The total insulin dose of our case was decreased to 20 units/day with HbA1c at 6.8% and CPI at 1.7 after 5 years of dasatinib. Similarly, in Ono’s case [7], CPI increased from 0.3 before treatment to 1.42 at 6 weeks after dasatinib initiation, and insulin injection was not required for glycemic control at 5 weeks after initiation because of a rapid improvement of insulin secretory response compared to our case. In our case, insulin secretory activity was preserved for 5 years during simultaneous treatment with anti-diabetic agents and dasatinib for CML. It has been reported that Src inhibitors reduce production of Reactive Oxygen Species (ROS) resulting in increased ATP levels and then improvement of insulin secretory function [21]. Dasatinib inhibits multiple family kinases including BCR-ABL, Src family kinases, receptor kinases, and TEC kinases [3]. Thus, one potential mechanism for the improvement of insulin secretion by dasatinib treatment for CML, in addition to strict diabetes control, which itself is known to improve β-cell function [22], is an inhibition of Src kinases in pancreatic β-cells [21,23,24]. However, this is just one possibility; another is the improvement of insulin signaling [10]. In the off-set action of TKIs, it has also been reported that c-kit stimulates insulin secretion [25] and that PDGFβ stimulates hepatic insulin sensitivity [26], and either of these common kinase activities could be responsible for TKI-related glucose-lowering effects [27]. The wide variation of TKIs’ effects on glucose regulation found in imatinib, dasatinib and nilotinib suggests the possibility of other target molecules that may improve glycemic control in T2DM patients. A retrospective cohort study of Mayo clinic patients hypothesized that the antidiabetic effects of dasatinib compared to imatinib are due to its senolytic properties [28]. The durability of the improved glucose-lowering effects of dasatinib in our 2 cases of T2DM patients with CML without any stepping-up of hypoglycemic drugs over time, appears to be due, at least in part, to continuously maintained insulin secretory capacity for 5 years.
Conclusion
In conclusion, hyperglycemia in our T2DM patients with CML was well controlled with the same maintenance dose of dasatinib (either 50 mg or 100 mg, once daily) for at least 5 years without any stepping-up of hypoglycemic agents over time. It is very important to perform careful follow-up with assessments of both the clinical courses of CML and glucose control in diabetes patients who are prescribed TKIs for concomitant leukemic disease.
Declarations
Acknowledgements: Our two patients gave us their informed consent for the publication of anonymized data from their medical records.
Competing interests: AK has acted as a medical consultant for Sunstar, Inc. and the Omi Medical Center where the AK belongs, is funded by Sunstar, Inc. The remaining authors have no competing interests to disclose.
Copyright transfer: The authors have agreed that the copy right for this article is transferred to the Journal of Clinical Images and Medical Case Reports (JCIMCR), if and when the article is accepted for publication.
References
- Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2018 update on diagnosis, therapy, and monitoring. Am J Hematol. 2018; 93: 442-459.
- Aguilera DG, Tsimberidou AM. Dasatinib in chronic myeloid leukemia: A review. Therapeutics and Clinical Risk Management. 2009; 5: 281–289.
- Nekoukar Z, Moghimi M, Salehifar E. A narrative review on adverse effects of dasatinib with a focus on pharmacotherapy of dasatinib-induced pulmonary toxicities. Blood Res. 2021; 56: 229-242.
- Breccia M, Muscaritoli M, Aversa Z, et al. Imatinib mesylate may improve fasting blood glucose in diabetic Ph+ choronicmyelogeneous leukemia pattients responsive to treatment. J Clin Oncol. 2004; 156: 4653-4655.
- Veneri D, Franchini M, Bonora E. Imatinib and regression of type 2 diabetes. New Engl J Med. 2005; 352: 1049-1050.
- Gómez Sámano1 MA, Baquerizo Burgos JE, Coronel Coronel MF, et al. Effect of imatinib on plasma glucose concentration in subjects with chronic myeloid leukemia and gastrointestinal stromal tumor. BMC Endocrine Disorders. 2018; 18: 77. https://doi.org/10.1186/s12902-018-0303-x
- Ono K, Suzushima H, Watanabe Y, et al. Rapid amelioration of hyperglycemia facilitated by dasatinib in a chronic myeloid leukemia patient with type 2 diabetes mellitus. Intern Med. 2012; 52: 2763-2766.
- Lundholm MD, Charnogursky GA. Dasatinib-induced hypoglycemia in a patient with acute lymphoblastic leukemia. Clin Case Rep. 2020; 8: 1238-1240.
- Breccia M, Muscaritoli M, Cannella L, et al. Fasting glucose improvement under dasatinib treatment in an accelerated phase chronic myeloid leukemia patient unresponsive to imatinib and nilotinib. Leuk Res. 2008; 32: 1626-1628.
- Iizuka K, Niwa H, Kato T, et al. Dasatinib improves insulin sensitivity and affects lipid metabolism in a patient with chronic myeloid leukemic. BMJ Case Rep. 2016.
- Yu L, Liu J, Huang X, Jiang Q. Adverse effects of dasatinib on glucose-lipid metabolism in patients with chronic myeloid leukaemia in the chronic phase. Sci Rep. 2019; 9: 17601. | https://doi.org/10.1038/s41598-019-54033-0
- Iurlo A, Orsi E, Cattaneo D, et al. Effects of first- and second-generation tyrosine kinase inhibitor therapy on glucose and lipid metabolism in chronic myeloid leukemia patients: a real clinical problem? Oncotarget. 2015; 6: 33944-33951.
- Racil Z, Koritakova E, Sacha T, et al. Insulin resistance is an underlying mechanism of impaired glucose metabolism during nilotinib therapy. Am J Hematol. 2018; 93: E342-E345.
- Spatafora L, Golemiec B, Thabane L, et al. Glycemic control in patients treated with tyrosine kinase inhibitors for chronic myeloid leukemia: A systemic review. Blood. 2018; 132: 4273.
- Beccarani M, Deininger MW, Rosti G, et al. European Leukemia Net recommendations for the management of chronic myeloid leukemia: 2013. Blood. 2013; 122: 872-884.
- Ross DM, Arthur C, Burbury K. Chronic myeloid leukemia and tyrosine kinase inhibitor therapy: Assessment and management of cardiovascular risk factors. Intern Med J. 2018; 48: 5-13.
- Cortes JE, Saglio G, Kantarjian HM, et al. Final 5-year study results of DASISION: The dasatinib versus imatinib study in treatment- naïve chronic myeloid leukemia patientstrial. J Clin Oncol. 2016; 34: 2333-2340.
- Monnier L, Lapinski E, Collete C. Contributions of fasting and postprandial plasma glucose increments to the overall diurnal hyperglycemia of type 2 diabetic patients: Variations with increasing levels of HbA1c. Diabetes Care. 2003; 26: 881–885.
- Ahuja V, Kadowaki T, Evans RW, et al. Comparison of HOMA-IR, HOMA-β% and disposition index between US white men and Japanese men in Japan: the ERA JUMP study. Diabetologia. 2015; 58: 265–271.
- Fitter S, Vandyke K, Schultz CG, et al. Plasma adiponectin levels are markedly elevated in imatinib-treated Chronic Myeloid Leukemia (CML) patients: A mechanism for improved insulin sensitivity in type 2 diabetic CML patients? J Clin Endocrinol Metab. 2010; 95: 3763-3767.
- Kominato R, Fujimoto S, Mukai E, et al. Src activation generates reactive oxygen species and impairs metabolism-secretion coupling in diabetic Goto-Kakizaki and Ouabain-treated rat pancreatic islets. Diabetologia. 2008; 51: 1226-1235.
- Weng J, Li Y, Xu W, et al. Effect of intensive insulin therapy on β-cell function and glycaemic control in patients with newly diagnosed type 2 diabetes: A multicentre randomised parallel-group trial. Lancet. 2006; 371: 1753-1760.
- Sato H, Nagashima K, Ogura M, et al. Src regulates insulin secretion and glucose metabolism by influencing subcellular localization of glucokinase in pancreatic β-cells. J Diabetes Investig. 2016; 7: 171–178.
- Cheng H, Straub SG, Sharp GWG. Inhibitory role of Src family tyrosine kinases on Ca2+-dependent insulin release. AJP Endocrinology and Metabolism. 2007; 292: E845-E852.
- Feng ZC, Li, J, Turco BA, et al. Critical role of c-kit in beta cell function: Increased insulin secretion and protection against diabetes in a mouse model. Diabetologia. 2012; 55: 2214-2225.
- Raines SM, Richards OC, Schneider LR, et al. Loss of PDGF-B activity increases hepatic vascular permeability and enhances insulin sensitivity. Am J Physiol Metab. 2011; 301: E517-E526.
- Agostino NM, Chinchilli VM, Lynch CJ. et al. Effect of the tyrosine kinase inhibitors (sunitinib, sorafenib, dasatinib, and imatinib) on blood glucose levels in diabetic and nondiabetic patients in general clinical practice. J Oncol Pharm Pract. 2011; 17: 197-202.
- Salaami O, Kuo CL, Drake MT, et al. Antidiabetic effects of senolytic agent dasatinib. Mayo Clin Proc. 2021; 96: 3021-3029.