
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case report of QT prolongation beyond the
recovery phase of COVID 19 infection
Ali Kharazi1; Mohammad Alasti2; Mehrdad Golian3; Hossein Fatemian4; Mohammad Hossein Nikoo5*
1Northern Ontario School of Medicine, 955 Oliver Rd, Thunder Bay, ON P7B 5E1, Canada.
2Monash Heart, Monash Medical Centre, 246 Clayton Road, Clayton, VIC 3168, Canada.
3University of Ottawa Heart Institute, Ottawa, Canada.
4Student Research Committee, Shiraz University of Medical Sciences, Shiraz, Iran.
5Non-communicable Diseases Research Centers, Shiraz, Iran.
*Corresponding Author : Mohammad H Nikoo
Non-communicable Diseases Research Centers, Shiraz, Iran.
Email: hoseinfatemian@yahoo.com
Received : Aug 17, 2022
Accepted : Sep 08, 2022
Published : Sep 15, 2022
Archived : www.jcimcr.org
Copyright : © Nikoo MH (2022).
Keywords: Covid-19; QT prolongation; Cardiac injury; Arrhythmia; Electrocardiogram.
Abbreviations: ECG: Electrocardiogram; QTc: Corrected QT; ER: Emergency Room; mmol/L: Millimole per Litre; μmol/L: Micromole per Litre; mg/L: Milligram per Litre; ng/ml: Nanogram per Millilitre; U/L: Unit per Litre; msec: Millisecond; CBC: Complete Blood Count; AMA: Against Medical Advice.
Citation: Kharazi A, Alasti M, Golian M, Fatemian H, Nikoo MH. A case report of QT prolongation beyond the recovery phase of COVID 19 infection. J Clin Images Med Case Rep. 2022; 3(9): 2055.
Introduction
Covid-19 influence on QT prolongation is mainly caused by antiviral medications. However, there is some evidence of independent effect of disease on QT interval in association with cardiac injury and on the other hand as previously demonstrated, acquired long QT has potential negative impact on the outcome of Covid-19 infection. We are presenting a case of QT prolongation in an ambulatory patient with a pre-existing borderline QT interval who was on no antiviral medications.
Case report
A 48-year-old female patient presented to the hospital in April 2021, with persistent chest pain for 2 days. She has been a frequent visitor to Emergency Room (ER) for 6 years due to severe alcohol use disorder. She denied any suicidal thoughts or drug overdose. She was known to have untreated hepatitis C with fatty liver and no evidence of cirrhosis on a recent ultrasound study. An inquiry from her pharmacy confirmed she was not using Suboxone within last weeks and she had never used Methadone. About two months prior to this admission, a diagnosis of Covid-19 was made on when she was brought to ER with loss of consciousness and possible seizure but with no fever or any respiratory symptoms and of note a near normal ECG (Figure 1A) which was unchanged compared to her ECGs in the past. The troponin level was also unremarkable when Covid test was found positive. She left the hospital Against Medical Advice (AMA), and she never started any antiviral medications.

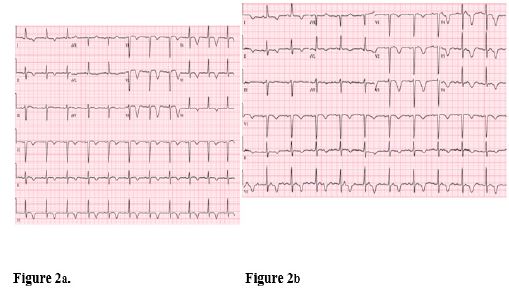
8 weeks later, she presented to the ER with severe which was described by her as a steady pressure over the sternal area with no pleuritic features. She was found to have new deep T wave inversions on precordial leads with a Corrected QT (QTc) interval of about 510 msec (Figure 2a). Her initial Troponin-I was mildly elevated at 0.034 ng/ml. Her blood workup did not show any new changes compared to previous admissions. CBC was unremarkable other than for mild anemia with a hemoglobin of 110 mg/L. Other lab data included Sodium 145 mmol/L, Potassium 3.8 mmol/L, Magnesium 0.67 mmol/L, chloride 114 mmol/L, creatinine 50 μmol/L, random glucose 7 mmol/L, Alanine Amin Transferase 160 U/L and total bilirubin 6 μmol/L. Toxicology showed a blood ethyl alcohol level of 81 mmol/L which was actually lower than her previous admissions and the test was negative for drugs including cocaine and narcotics. Her nasal swab was negative for covid-19 this time.
The patient was transferred to cardiology unit where no arrhythmias were noticed during her stay. A high-quality echocardiogram showed normal left ventricular systolic function with no regional wall motion abnormalities and ejection fraction of 60%. No structural heart abnormalities were reported. Her troponin level peaked at 0.066 ng/ml next day and started to drop later. According to persisting chest pain and marked repolarization abnormalities, coronary artery angiography was performed which showed normal coronary arteries and left ventricular size and contractility. As stress related cardiomyopathy was suggested by enormous ECG changes, a repeat echo was requested which did not support this impression. The patient left the hospital the day after as AMA. We could reach out her pharmacy to start her on Nadolol 80 mg daily.
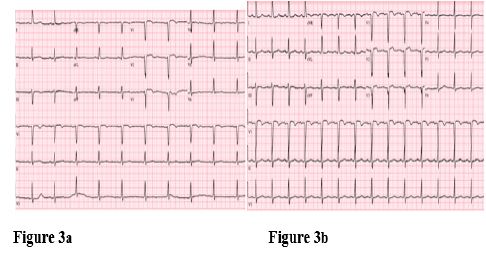
We were able to follow up her by tracking her next admissions to ER with alcohol related issues. The troponin level returned to normal in 4 days with no increments afterwards. QTc increased to 530 msec on day 5 (Figure 2b) and was around 510 msec on day 9. Then it gradually decreased to 490 msec on day 16 and dropped to 447 on day 22 (Figure 3a) although there were still precordial T wave inversions. The ECG eventually improved to her baseline in about 2 months (Figure 3b). Almost all her referrals to ER were related to alcohol intoxication with no records of syncope.
A review of patient’s ECGs since 2010 revealed the QTc varied in the range of 445 to 475 msec with no T wave inversions although even when the QTc was in the normal range, there was always subtle repolarization abnormality which were best identifiable on lead V5. There was no record of significant QT prolongation on her multiple admissions including one ICU admission due to viral pneumonia. Accordingly, her QT interval and T waves has been never affected by the level of serum alcohol despite its known influence on repolarization. Therefore, her recent Covid infection could be considered the only explanation of the delayed dramatic ECG changes which had never been noticed along with her prior even worse alcohol toxifications, infections and other medical issues. However, the delayed presentation of ECG changes when the Covid test had turned negative was arguable.
Discussion
Cardiac involvement is well known to be both prevalent and prognostically significant in the course of Covid-19 disease [1]. Myocardial injury is particularly common among hospitalized patients and is believed to be secondary to cytokine storm and consequent vascular injury, plaque instability and coagulopathy. Meanwhile, direct injury with resulting fulminant myocarditis could be a less likely contributing cause in some patients [1].
Cardiac injury over the course of Covid-19 might be incidentally found by elevated cardiac markers or it can be associated with chest pain and ECG abnormalities [2]. An extreme type of cardiac injury was described by a case series of New York city hospitals which reported 18 hospitalized patients with Covid-19 and ST-segment elevation along with increased troponin levels. Only 8 of these patients received an angiographic diagnosis of Myocardial Infarction (MI). Their report showed a poor prognosis of ST segment elevation with covid-19 as 4 patients with MI and 9 patients with non-coronary myocardial injury died in the hospital. In the light of other studies, cardiac involvement in Covid-19 have other manifestations aside from fulminant heart failure including conduction impairment, arrhythmias and acquired long QT which has received the most attention [2].
Although QT prolongation with Covid-19 has been noted more as a link to antiviral therapies, it can also be a possible consequence of cardiac injury even in subclinical cases as it was shown that patients with QT prolongation are more likely to have other ECG abnormalities and elevated troponin [3]. Besides, acquired long QT syndrome is known to company other types of cardiac injury such as acute ischemia, stress related cardiomyopathy and maybe more relevantly myocarditis which has a worse outcome in association with QT prolongation. Notably though, true myocarditis, although reported, has not been found as a common cause of cardiac injury in Covid-19 by biopsy-based studies [1]. Despite seemingly to be a reasonable hypothesis, there is still no evidence of independent influence of Covid-19 on QT interval. So far, almost all the reported cases of acquired long QT with Covid-19 come from hospitalized patients on antiviral treatment. However, an increased risk of out of hospital sudden death was suggested by Lombardia Cardiac Arrest Registry which not only reported 58% increase in the incidence of Sudden Cardiac Death (SCD) following the outbreak but also a highly likely association of these deaths to Covid-19 as about 74% of victims were diagnosed or suspected of having the disease prior to death [4]. The possible contribution of QT prolongation in this regard was not investigated.
There have been a handful case reports of hospitalized patients whose prolonged QT intervals were not correlated or were out of proportion to antiviral treatments where QT prolongation could be attributed to hypoxemia and severe illness [5,6]. To our best knowledge, we are presenting the first case of QT prolongation in an ambulatory Covid-19 infected patient on no antiviral medication. We were able to track her ECGs over past 6 years, and according to the range of QT intervals which was usually borderline with the longest QTc of 465 msec and subtle repolarization abnormalities, it was reasonable to presume she had an underlying genetic concealed or alcohol related long QT abnormality. Nevertheless, her ECGs were never markedly abnormal prior to COVID 19 infection despite variable alcohol levels and similar electrolyte levels. Noteworthy, during a previous stay in ICU due to pneumonia, her QTc stayed below 460 msec in association of serum K level of 3.1 mmol/L.
In our case, QT prolongation and T wave inversions developed along with chest pain about 8 weeks after receiving a positive Covid test when the Covid test had turned negative. This delayed presentation keeps with an autoimmune mechanism similar to post viral myocarditis rather than direct viral invasion of myocytes or cytokine storm during acute phase of infection. In a Cohort study of 100 German patients who were recently recovered from Covid-19, a follow up cardiac MRI after a median 71 days of initial test, revealed ongoing cardiac inflammation along with elevated troponin-T levels [7]. Noteworthy, most of these patients were non-hospitalized patients with initial mild symptoms. However, the lag time until troponin elevation was not addressed. The novel finding in our case was short period of active cardiac injury but ongoing prolonged QT which lasted about 2 months. Persisting QT prolongation in our patient despite resolved cardiac injury might be in concordance with the role of autoantibodies against cardiac electrical channels. The involvement of autoantibodies in repolarization abnormalities has been demonstrated by growing evidence [8]. These findings may warrant further research to elucidate the contribution of autoantibodies to cardiac arrhythmias in Covid-19 patients.
Conclusion
Our case represents a patient with baseline borderline long QT who developed pronounced QT prolongation 8 weeks after a positive Covid test with a non-critical condition. The QT prolongation could not be explained by antiviral medication, cardiac ischemia, Takotsubo cardiomyopathy, direct viral invasion, alcohol intoxication or any contributing factor other than a transient late cardiac injury after Covid infection. This may imply that patients with borderline long QT or those with long QT syndrome are at higher risk of aggravated QT prolongation or torsade even in milder forms of the disease with potential late presentation. This hypothesis might partly explain the increased incidence of SCD in Lobbardia registry [5]. Until clinical studies demonstrate such a possible correlation, it seems prudent to monitor patients with baseline repolarization abnormalities and recent Covid positive test with serial ECGs and closer follow up. The role of autoantibodies in QT prolongation in these patients is also an exciting subject of research.
References
- Shi S, Qin M, Shen B, et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 2020; 5: 802-810.
- Sripal Bangalore, Atul Sharma, Alexander Slotwine, et al. ST-Segment Elevation in Patients with Covid-19 — A Case Series. N Engl J Med. 2020; 382; 25.
- Khalid Changal, David Paternite, Sean Mack, et al. Coronavirus disease 2019 (COVID‑19) and QTc prolongation. BMC Cardiovasc Disord. 2021; 21: 158. https://doi.org/10.1186/s12872-021-01963-1.
- Enrico Baldi, Giuseppe M Sechi, Claudio Mare, et al. Out-of-Hospital Cardiac Arrest during the Covid-19 Outbreak in Italy. N ENGL J MED. 2020; 383; 5. nejm.org.
- Jose´ Luis Merino, Marcel Martinez Cossiani, Angel Iniesta Carlos Escobar, Juan R Rey, Sergio Castrejón Castrejón. COVID-19 and QT interval prolongation: More than just drug toxicity?. Europace. 2020; 22: 1479.
- Anupama BK, Soumya Adhikari, Debanik Chaudhuri. Prolonged QT Interval in a Patient with Coronavirus Disease-2019: Beyond Hydroxychloroquine and Azithromycin. J Investig Med High Impact Case Rep. 2020; 8: 2324709620948407.
- Valentina O Puntmann, M Ludovica Carerj, Imke Wieters, et al. Outcomes of Cardiovascular Magnetic Resonance Imaging in Patients Recently Recovered From Coronavirus Disease 2019 (COVID-19). JAMA Cardiol. 2020; 5: 1265-1273.
- Pietro Enea Lazzerini, Pier Leopoldo Capecchi, Franco Laghi Pasini. Long QT syndrome: An emerging role for inflammation and immunity. Front. Cardiovasc. Med. 2020; 2: 26.