
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
A hyperplastic growth of lip
Bhumika Gumber1; Vikender Singh Yadav2*; Kanika Makker2; Deepika Mishra3; Subramony Bhagavatheeswaran1
1Department of Periodontics, Post Graduate Institute of Dental Sciences, Rohtak, India.
2Division of Periodontics, Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
3Department of Oral Pathology and Microbiology, Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India.
*Corresponding Author : Vikender Singh Yadav
Associate Professor, Division of Periodontics, Centre for Dental Education and Research, All India Institute of Medical Sciences, New Delhi, India 110029.
Email: vikenderyadav@gmail.com
Received : Aug 22, 2022
Accepted : Sep 09, 2022
Published : Sep 16, 2022
Archived : www.jcimcr.org
Copyright : © Yadav VS (2022).
Citation: Gumber B, Yadav VS, Makker K, Mishra D, Bhagavatheeswaran S. A hyperplastic growth of lip. J Clin Images Med Case Rep. 2022; 3(9): 2058.
Case report
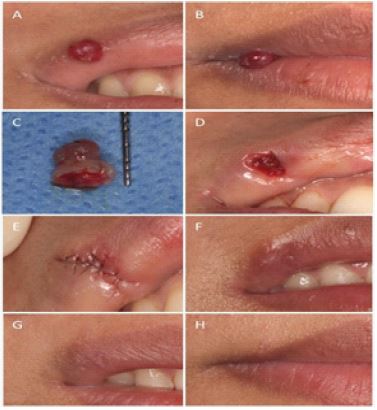
A 25- year-old systemically healthy female patient reported with an aesthetic complaint due to a growth in the corner of right upper lip present for 2 months. Clinical examination revealed a solitary spherical-shaped bright red fibrous overgrowth measuring 4 x 4 mm involving the mucocutaneous line of upper lip (Figure 1A & B). On palpation, it was non tender, smooth in texture, and soft in consistency. Based on the signs and symptoms, a provisional diagnosis of fibroma was made with a differential diagnosis of pyogenic granuloma.
After obtaining written informed consent, the lesion was excised in toto with 1 mm of healthy margin by performing two elliptical incisions (Figure 1C). The biopsied tissue was fixed in 10% formalin and sent for histopathological examination. Double-layered microsurgical suturing was done with 7-0 polyglactin suture (Figure 1D) followed by superficial suturing of the wound margins (Figure 1E). Postoperative instructions were given and analgesics were prescribed, as and when required. Healing was uneventful and sutures were removed at 10 days follow-up (Figure 1F). A good cosmetic outcome and high patient satisfaction was achieved at 3 months (Figure 1G & H).
Discussion
Fibroepithelial Polyp (FEP) or fibroma is a common non-neoplastic reactive lesion of theoral cavity. Although its aetiology is unknown, it can be congenital, infectious, inflammatory, or traumatic in origin. It clinically presents as a painless sessile or pedunculated growth. It can have firm and resilient, or soft and spongy consistency [1]. FEPs are non-malignant and have low recurrence rates. It is a commonly reported lesion on buccal mucosa and gingiva, but involvement of the lip is rare [2,3]. To the best of our knowledge this is a rare case reporting the occurrence of FEP on the lip.
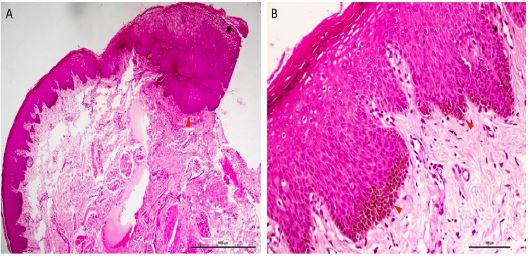
Histologically, the present lesion showed ortho-keratinised stratified squamous epithelium continuing into hyperplastic para-keratinised stratified squamous epithelium with basilar hyperplasia and elongated rete ridges. Underlying connective tissue showed mild inflammation (Figure 2). Based on the histological picture, the case was diagnosed as FEP/ fibroma.
Lips are highly visible facial structures which are exposed to various internal and external stimuli, resulting in the development of diverse lesions. The diagnosis of these lesions can be difficult, often warranting the need for biopsy. Excisional biopsy of the suspected orofacial lesion can be most challenging because it may result in deformity, especially those involving vermilion border of the lip. Patient satisfaction and self-reported aesthetics have become significant patient reported outcome measures. Utmost surgical precision is required for good cosmetic outcome. Early healing and good aesthetics with minimal scarring of the healed tissues can be better achieved by primary closure of the wound using microsurgical technique as compared to conventional suturing [4].
In the present case report double-layered microsurgical suturing was performed. The deeper layer was first sutured to minimize tension at the wound edge and reduce the dead space followed by superficial suturing of the wound margins to achieve primary closure [5]. The healing was uneventful with highly aesthetic outcome at 3 months follow up.
Conflict of interest statement: The authors declare no conflict of interest.
References
- Yeatts D, Burns JC. Common oral mucosal lesions in adults. American Family Physician. 1991; 44: 2043–2050.
- Monteiro LS, Albuquerque R, Paiva A, de la Peña Moral J, Amaral JB, et al. A comparative analysis of oral and maxillofacial pathology over a 16-year period, in the north of Portugal. International Dental Journal. 2017; 67: 38–45.
- Sengüven B, Bariş E, Yildirim B, Shuibat A, ÖzerYücel Ö, Museyibov F, et al. Oral mucosal lesions: A retrospective review of one institution’s 13-year experience. Turkish Journal of Medical Sciences. 2015; 45: 241–245.
- Yadav VS, Salaria SK, Bhatia A, Yadav R. Periodontal microsurgery: Reaching new heights of precision. Journal of Indian Society of Periodontology. 2018; 22: 5–11.
- Lloyd JD, Marque MJ, Kacprowicz RF. Closure techniques. Emergency Medicine Clinics of North America. 2007; 25: 73–81.