
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Surgical outcome, clinical presentations and imaging
characteristics of patients with sphenoid wing
en-plaque meningiomas; A case series
Alireza Tabibkhooei1; Jaber Hatam1*; Meysam Abolmaali2; Mahisa Mokhtari3; Farid Kazemi Gazik1; Saeid Rezaei4; Sarah Mohyeddinipour5
1Skull Base Research Center, Department of Neurosurgery, Iran University of Medical Sciences, Tehran, Iran.
2Shefa Neuroscience Research Center, Khatam Alanbia Hospital, Tehran, Iran.
3Department of Neurology, RasoulAkram Hospital, Iran University of Medical Sciences, Tehran, Iran.
4Eye and Skull Base Research Center, The Five Senses Institute, Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran, Iran.
5Department of Neurosurgery, Research Assistant, Tehran Islamic Azad University of Medical Sciences, Tehran, Iran.
*Corresponding Author : Jaber Hatam, MD
Department of Neurosurgery, Rasoul Akram Hospital, Iran University of Medical Sciences, Tehran 14665-354, Iran.
Tel: +98 935922 1921;
Email: Jaber.hatam@yahoo.com
Received : Aug 19, 2022
Accepted : Sep 12, 2022
Published : Sep 19, 2022
Archived : www.jcimcr.org
Copyright : © Hatam J (2022).
Abstract
Background: En plaque meningioma is a type of tumor that causes infiltrates into the bony tissue and forms a lamellar structure. The symptoms and prognosis are significantly related to the severity of bone involvement and involved areas. Given the limited information from the basic knowledge of these patients, we aimed to determine the characteristics and post-surgical outcomes of patients operated via pterional approach surgery.
Methods: Patients with meningioma en plaque who underwent tumor resection surgery at Rasoul Akram Hospital between 2014 and 2020 were included. The study recorded patient baseline characteristics, tumor laterality, involved areas, symptoms, recurrence, cosmetic satisfaction results, follow-up length, intraoperative bleeding, surgical complications, hospitalization complications, and death. Moreover, the post-surgical outcomes of patients were evaluated during the study.
Results: A total of 22 patients were evaluated. The mean age of patients was 45.6 ± 11.1 years, of which all 22 cases were female. Proptosis, decreased visual acuity and headache were the most common symptoms observed in 19 (86.4%), 17 (77.3%), and 11 (50%) cases, respectively. In preoperative MRI imaging, the most common involved anatomical components were sphenoid wing (100%), superior orbital fissure (95.5%), superior orbital wall (86.4%), dura matter (86.4%), and lateral orbit wall (81.8%). In 2-month follow-up surgery, deterioration of the temporal area was observed in 6 patients, and cerebral infarction was seen in one case.
Conclusion: The pterional approach provides excellent and easy access to the orbit and middle cavity and facilitates tumor resection and optic canal pressure relief among the various surgical procedures.
Keywords: Meningioma enplaque; Sphenoid wing; Proptosis; Pterional approach; Neurosurgical science.
Citation: Tabibkhooei A, Hatam J, Abolmaali M, Mokhtari M, Gazik FK, et al. Surgical outcome, clinical presentations and imaging characteristics of patients with sphenoid wing en-plaque meningiomas; A case series. J Clin Images Med Case Rep. 2022; 3(9): 2059.
Introduction
Meningiomas are one of the most common benign intracranial neoplasms that are morphologically classified into global and flat types [1]. The term “meningioma en masse” and “meningioma en plaque” were first used by Cushing to morphologically classify intracranial meningiomas. The enplaque type is the rarer type which accounts for 2%-9% of all intracranial tumors [2,3].
It is an invasive rare category of meningioma with a feature of pathologic hyperostosis of sphenoid bone [1,4]. The tumor’s adjacency to important structures such as cavernous sinus, Superior Orbital Fissure (SOF), and optic nerve and also its invasive nature would result from its significant damage. Headache, diplopia, visual disturbances, abnormal eye movements, ptosis, and proptosis are the observed symptoms and the latter is the most common symptom [5-9].
This type of meningioma does not consist of a unique imaging feature. However, a more infiltrating growth pattern over the durais evident which is most commonly seen along the sphenoid ridge. The typical Magnetic Resonance Imaging (MRI) signal intensity characteristics consist of isointensity to slight hypointensity relative to grey matter and asymmetric thickened sheets of enhancing duracan be seen on the T1-weighted sequence [10]. Preservation of critical functions and also resection of the lesion are two main goals in the management of this disorder [11]. The standard treatment for clinically evident meningiomas is microsurgery. However, the optimal surgical approach, the extent of resection, and the need for orbital reconstruction have still remained as controversial issues.
Despite advances in surgical techniques such as neuro-navigation and modern imaging techniques, sphenoid wing meningiomas are still a severe challenge to neurosurgeons due to their close association with areas such as the orbital cavity cavernous sinus, a group of cranial nerves and blood vessels. The tumor tends to spread to nearby bones. Therefore, interdisciplinary cooperation is essential for complete tumor resection, preservation of vital structures, and reconstruction of critical cranio-orbital structures.In past studies, the goal was total resection [12].
Still, due to the nature of the tumor involvement, which sometimes causes involvement of the cavernous sinus and SOF, subtotal resection has been performed inevitably. This study aims to evaluate the surgical results, recurrences, and pathologies of patients with en plaque meningioma of the sphenoid bone treated with apterional approach.
Material and methods
In this case series, all patients with a definitive diagnosis of sphenoid wing Enplaque meningioma who underwent surgical treatment in Rasoul Akram Hospital between 2014 and 2020 were recruited.
Ethical approval was received from the ethics committee of the Iran University of Medical Sciences (IUMS), (Ethics Code: IR.IUMS.FMD.REC.1398.265). Written consent was also obtained from each patient. Demographic, clinical, and pathological information of 22 eligible patients with definitive diagnosis by imaging methods such as brain Computed Tomography Scan (CT-scan) and brain MRI were collected retrospectively. Patients were asked for additional information and follow-up visits in order to perform related examinations in the neurosurgery clinic.
Clinical manifestations such as proptosis, seizures, confusion, headache, diplopia, drooping eyelids, trigeminal paresthesia, mental confusion, partial facial paralysis, and radiologic features were collected prior to the surgery in the designed forms.
Surgical complications (Cerebrospinal Fluid [CSF] leakage, hydrocephalus, meningitis, infarction, bleeding, cerebral edema, wound dehiscence, Postoperative seizures, Postoperative visual impairment, Postoperative ocular motor muscle paralysis, Postoperative drooping eyelids, Postoperative proptosis, and enophthalmos), Hospital complications (Pulmonary Embolism [PE], Gastro-Intestinal Bleeding [GIB], Urinary Tract Infection [UTI] and pneumonia), Other complications and death were evaluated. The patients were followed up by a brain CT scan and brain MRI two months followed by the surgery. Then, they were continued to observe by a 6 to 12 months interval follow-up.
Inclusion criteria were the definitive diagnosis of sphenoid wing en plaque Meningioma and surgery between 2014 and 2020. Exclusion criteria were: In ability to contact the patient to be invited to follow-up and the patient not to refer to follow-up. Data of all individuals were entered into SPSS Software (SPSS version 22) and were statistically analyzed. Different correlation coefficients or chi-square tests were used depending on the type of variable (qualitative-nominal, qualitative-rank, and quantitative with or without normal distribution based on the Kolmogorov-Smirnov uniform test). The significance level was considered P< 0.05. There was a commitment to the principles of the Helsinki Declaration throughout the study.
Surgical approach
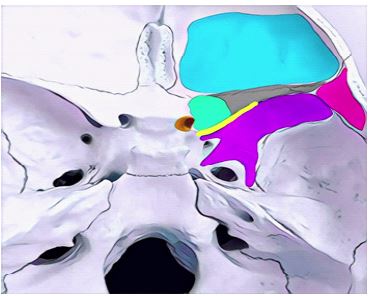
All patients underwent sphenoid meningioma tumor resection using a pterional approach. The patient is positioned supine and the head rotation is adapted to the exact location of the lesion. In a sterile manner, the surgical field was clipped, prepped, and draped. A frontotemporal skin incision is made and to preserve the frontal branch of the 7th cranial nerve beside the superficial temporal artery, temporal muscle dissection is performed interfacially. After deep dissection of the temporalis muscle, a pterional craniotomy is performed for the patient and the sphenoid ridge is removed to allow access to the SOF. Following resection of the involved SOF area, the lateral wall and the roof of the orbit space are removed, and in case of optic canal involvement, the canal roof is also removed and the optic nerve is released (Figures 1,2).
In cases of inferior orbital fissure involvement, we did not apply for decompression due to the possibility of damage to the neural and vascular elements of the temporal skull base. In the next step, the intradural compartments were resected using a microscope along the anterior clinoid and sphenoid wing. Optic nerve decompression was performed under the view of a microscope. Intramural segments of the tumor with overlying involved dura resected and were repaired with peri cranium autopatch. After ensuring the release of the internal elements of the SOF and the optic canal from the tumor, the roof and the lateral wall of the orbital space are reconstructed with a titanium mesh (Figure 3). Finally, cranioplasty of the frontotemporal areas is performed and the skin incision of the surgical site is repaired.

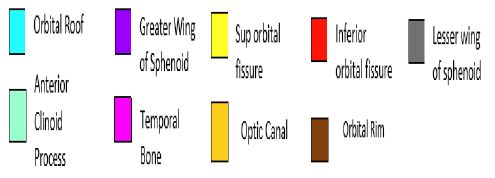
A. lateral wall of orbit (yellow arrow) and frontotemporal region (red arrow),
B. It is noteworthy that all the operations were carried out by a single neurosurgeon and using a single method. Regardless of tumor grade, and extent of tumor progression, no was patient scheduled forpost-surgical radiotherapy.
Results
Demographic results
After excluding 2 patients from the study during follow-up, a total of 22 female patients with sphenoid en plaque meningioma were studied. The mean age of participants in this study was 45.6 ± 11.1 years (range 20-72). Among the studied patients, eight cases had meningioma on the right sphenoid wing (36.4%) and 14 had left sphenoid wing (63.6%). There were 21 patients with grade I tumors (95.5%) and 1 patient with grade II (4.5%).
Medical history
Among the patients, five cases had a history of chronic diseases (22.7%) of which 2 patients with hypertension, 2 patients with anemia, and 1 patient with hypothyroidism. Also, none of the patients had a history of head and neck radiotherapy, head trauma, or hormone therapy, and also no history of brain tumor was observed in first-degree relatives.
Findings prior to surgery
According to the preoperative examinations, the following symptoms and complications were observed among the patients which led to the diagnosis of meningioma en plaque. Among them, 19 patients had proptosis (86.4%), 17 patients had decreased visual acuity (77.3%), 11 patients had headache (50%), 4 patients had ptosis (18.2%), 4 patients presented with blindness (18.2%), 2 patients had vertigo (9.1%), 2 patients had oculomotor nerve paresis (9.1%), 1 patient with facial pain (4.5%), 1 patient with facial numbness (4.5%), and 1 patient with swelling eyes (4.5%) (Table 1).
Table 1: Signs and symptoms in patients with En Plaque Meningioma.
| Presenting sign | No. (%) |
|---|---|
| Proptosis | 19 (86.4) |
| Decreasing visual acuity | 17 (77.3) |
| Headache | 11 (50) |
| Ptosis | 4 (18.2) |
| Blindness | 4 (18.2) |
| Vertigo | 2 (9.1) |
| Ocular muscles paralysis | 2 (9.1) |
| Facial pain | 1 (4.5) |
| Trigeminal paresthesia | 1 (4.5) |
| Eye swelling | 1 (4.5) |
Anatomical locations involved in the tumor
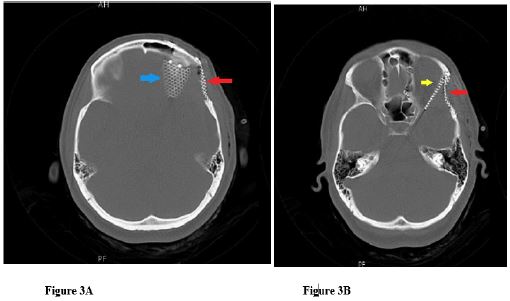
Five anatomical components had the highest rate of involvement by the tumor in the preoperative imaging. Sphenoid wing (100%), SOF (95.5%), orbital roof (86.4%), dura matter (86.4%), and lateral orbital wall (81.8%), respectively (Figures 4,5). The detail of pre-operative involved anatomical structures and post-operative structures infollow-up imaging were showed in Table 2.
Postoperative outcomes and recurrence
Participants were followed-up to evaluate the recurrence rate and assessed in terms of ocular aesthetic results. The mean duration of follow-up was 19.3 ± 11.9 months. All patients were satisfied in terms of postoperative cosmetic status, and only one participant (4.5%) experienced recurrence after the treatment.
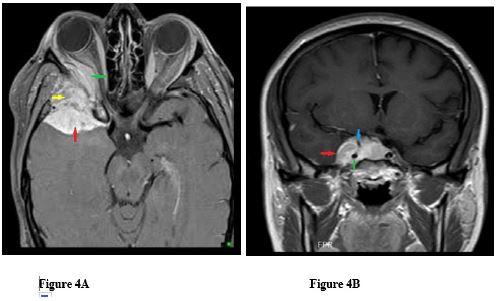
Table 2: Involved anatomical structures seen in pre-op and follow-up imaging.
| Involved anatomic structure | Pre-op, No (%) | 2-month follow-up, No (%) |
|---|---|---|
| Sphenoid wing | 22 (100) | 1 (4.5) |
| Lateral orbital wall | 18 (81.8) | 0 |
| Optic canal | 15 (68.2) | 0 |
| Anterior clinoid process | 13 (59.1) | 12 (54.5) |
| Dura matter | 19 (86.4) | 4 (18.2) |
| Superior orbital wall | 19 (86.4) | 0 |
| Orbital ridge | 0 | 0 |
| Superior orbital fissure | 21 (95.5) | 4 (18.2) |
| Inferior orbital fissure | 15 (68.2) | 14 (63.6) |
| Extraconal orbital space | 16 (72.7) | 3 (13.6) |
| Intraconal orbital space | 1 (4.5) | 0 |
| Cavernous sinus | 10 (45.5) | 10 (45.5) |
| Temporalis muscle | 5 (22.7) | 0 |
| Temporo-basal region | 8 (36.4) | 6 (27.3) |
| Fronto-basal region | 0 | 0 |
| Fronto-temporo-basal region | 12 (54.5) | 7 (31.8) |
Post-operative evaluation for any complications during follow-up showed only one patient (4.5%) suffered from cerebral infarction following surgery and 6 patients (27.3%) had atrophic temporal region. It is noteworthy that cerebral infarction is caused by carotid vasospasm in a patient with tumor involvement in the carotid wall and cavernous sinus. No other complications were seen in our patients during the follow-up time.
It should be noted that the mean volume of bleeding during surgery was 1297.7 ± 580.5 cc.
Our strategy in these surgeries was an effort for extensive resection. Out of 22 patients, 13 cases (59.1%) underwent total resection and 9 (40.9%) had a subtotal resection. Preoperative proptosis was completely improved in 17 patients (77.3%), and partial improvement was seen in five (22.7%).
Of eleven cases with headaches, 5 had a marked reduction in the frequency and severity of headaches. Of the 17 patients who had reduced visual acuity before surgery, 15 recovered. No improvement was seen in 2 patients.
There was only one case with recurrence that occurred 2-year followed by the initial surgery. Cavernous sinus and superior orbital fissure were involved by the tumor in this case and these parts hadn’t resected during the first surgery. The patient underwent a second operation and then, she was scheduled for radiation therapy. In a follow-up 3 years after the second surgery, no new recurrence was observed.
Discussion
This study reviewed 22 cases of meningioma enplaque that had received surgery between 2014 and 2020 in our center. There is a variety of terminologies used historically for this tumor subtype like hyperostosis meningioma, meningioma enplaque, and sphenoid wing meningioma [13].
For the first time, Cushing in 1938 differentiated and named the en plaque meningiomas [14]. Different terminologies and Cushing’s classification make it confusing and hard to have all-inclusive cohort studies [13]. In the present study, all patients were operated on by apterional approach to resect the tumor in a single surgeon manner.
For primary evaluation, CT scan and MRI as diagnostic imaging modalities should be taken into consideration. The first one is for detecting hyperostosis and bone involvement and the second one is for defining any dural or intradural involvement [15].
Similar to the current study, enplaque meningiomas are much more common in the female gender, during the fifth decade of age and tumor WHO grade I [2,16-18]. Accordingly, all of our participants were female and the mean age of them was 45.6 years, and only 1 patient was observed with a grade II tumor.
The most common symptoms and clinical signs of meningioma enplaque result from hyperostosis and its compression effects on the critical adjacent structures. Proptosis as the most common symptom seen in these patients has aesthetic importance and negatively affects quality of life and cosmetic appearance. Moreover, diplopia and visual disturbances, headache, and trigeminal paresthesia are other seen signs and symptoms [19,20].
Most of our patients presented with proptosis (86.4%) and other symptoms and complications like decreased visual acuity, headache, blindness, facial pain, and numbness, oculomotor muscle paralysis, and swelling eyes were observed.
Grade IIenplaque meningiomas are rarely reported in the literature with different follow-up outcomes. Honey bul et al. reported a case that underwent surgery and radiotherapy and eventually died due to disease progression [21]. Two other grade II cases were reported by Kiyofuji et al. one of them had suffered a second recurrence [13]. Samadian et al. reported a 4% prevalence of patients with grade II tumors in a single center study [16].
So far, frontotemporal, transzygomatic, and pterional surgical approaches with or without adjuvant chemotherapy or radiotherapy are used [16]. In the current study, all the patients underwent sphenoid meningioma tumor resection using a pterional approach.
Despite the fact that radical resection may lower the rate of reoccurrence, the risk of post-operative morbidities should not be ignored [18,22]. Our post-operative evaluation showed no major complications except for 1 patient who suffered from cerebral infarction following surgery and 6 patients (27.3%) with an atrophic temporal region.
Different rates of recurrence have been reported after surgery in the studies. Elder et al. in a review showed a higher rate of recurrence in cases with orbital and cavernous sinus involvement [17]. Samadian et al. reported reoccurrence in 12% of cases, in which one-third of them were grade II [16].
As we can see, three anatomical components had the highest rates of tumor involvement in the follow-up imaging comparing with preoperative imaging. Which, remnant tumor structures are seen in inferior orbital fissure (63.6 %), anterior clinoid process (54.5 %), and cavernous sinus (45.5%) in the 2-month follow-up imaging.
None of our patients had post operative radiation. With respect to the previous studies, there is no consensus for using postoperative radiotherapy in meningioma enplaque. Some studies suggest radiation therapy after resection while others believe there is no benefit in it [22,23]. All of our patients were satisfied in terms of postoperative cosmetic status and then, only one patient (4.5%) had recurrence after treatment.
Historically Orbital Reconstruction has been important in preventing enophthalmos after orbital wall resection. in this study, we used titanium mesh, which has been effective both cosmetically and in preventing the mentioned complications. And after the operation, we did not have any mumps from enophthalmos or exophthalmos (which can be caused by inability of proper orbital reconstruction and iatrogenic).
Given the low recurrence rate even in cases of cavernous sinus involvement, this study suggests that exceeding the cavernous sinus area is not worth the cost of morbidity, and even given the low grade of the vast majority of these tumors, the. Tumor residues do not require further action other than the follow-up, although larger-scale studies are needed to prove this fact statistically. According to the rarity of this tumor, perhaps, for the time being, it is enough to suffice with previous studies and opinions of experienced authors in this field.
Conclusion
The aim of the spheno orbital en plaque meningioma surgery is to utmost tumor removal in the safest condition with the minimum complication to improve clinical outcomes and reduce the recurrence rate. Among the various surgical procedures, the Pterional approach provides excellent and easy access to the orbit and the middle cranial fossa and facilitates the removal of the tumor and removing the pressure on the opticcanal.
References
- Bondy M, Lee Ligon B. Epidemiology and etiology of intracranial meningiomas: A review. Journal of neuro-oncology. 1996; 29: 197-205.
- Amirjamshidi A, Abbasioun K, Amiri RS, Ardalan A, Hashemi SMR, et al. Lateral orbitotomy approach for removing hyperostosing en plaque sphenoid wing meningiomas. Description of surgical strategy and analysis of findings in a series of 88 patients with long-term follow up. Surgical Neurology International. 2015; 6.
- Kim KS, Rogers LF, Goldblatt D. CT features of hyperostosing meningioma en plaque. American journal of neuroradiology. 1987; 8: 853-859.
- Leake D, Gunnlaugsson C, Urban J, Marentette L. Reconstruction after resection of sphenoid wing meningiomas. Archives of Facial Plastic Surgery. 2005.
- Gaillard S, Pellerin P, Dehellemmes P, Pertuzon B, Lejeune J, Christiaens JL. Strategy of craniofacial reconstruction after resection of spheno-orbital” en plaque” meningiomas. Plastic and reconstructive surgery. 1997; 100: 1113-1120.
- Bikmaz K, Mrak R, Al-Mefty O. Management of bone-invasive, hyperostotic sphenoid wing meningiomas. Journal of neurosurgery. 2007; 107: 905-912.
- Oya S, Sade B, Lee JH. Sphenoorbital meningioma: Surgical technique and outcome. Journal of neurosurgery. 2011; 114: 1241-1249.
- Ringel F, Cedzich C, Schramm J. Microsurgical technique and results of a series of 63 spheno-orbital meningiomas. Operative Neurosurgery. 2007; 60: ONS-214-ONS-222.
- Terrier LM, Bernard F, Fournier HD, Morandi X, Velut S, Hénaux PL, et al. Spheno-orbital meningiomas surgery: Multicenter management study for complex extensive tumors. World neurosurgery. 2018; 112: e145-e156.
- Watts J, Box G, Galvin A, Brotchie P, Trost N, Sutherland T, et al. Magnetic resonance imaging of meningiomas: A pictorial review. Insights Imaging. 2014; 5: 113-122. 10.1007/s13244-013-0302-4
- Rogers L, Barani I, Chamberlain M, Kaley TJ, McDermott M, Raizer J, et al. Meningiomas: Knowledge base, treatment outcomes, and uncertainties. A RANO review. Journal of neurosurgery. 2015; 122: 4-23.
- Schneider M, Potthoff AL, Borger V, Hadjiathanasiou A, Schäfer N, Güresir Á, et al. Outcome of tumor-associated proptosis in patients with spheno-orbital meningioma: Single-center experience and systematic review of the literature. Frontiers in Oncology. 2020: 1931.
- Kiyofuji S, Casabella AM, Graffeo CS, Perry A, Garrity JA, et al. Sphenoorbital meningioma: A unique skull base tumor. Surgical technique and results. Journal of Neurosurgery. 2019; 133: 1044-1051.
- Cushing H, Eisenhardt L. Meningiomas: Their Classification, Regional Behavior, Life History, and Surgical End Results: Springfield. Ill: CharlesC Thomas. 1938: 785.
- Simas NM, Farias JP. Sphenoid wing en plaque meningiomas: Surgical results and recurrence rates. Surgical neurology international. 2013; 4.
- Samadian M, Sharifi G, Mousavinejad SA, Amin AA, Ebrahimzadeh K, Tavassol HH, et al. Surgical Outcomes of Sphenoorbital En Plaque Meningioma: A 10-Year Experience in 57 Consecutive Cases. World Neurosurgery. 2020; 144: e576-e581.
- Elder TA, Yokoi H, Chugh AJ, Lagman C, Wu O, et al. En Plaque Meningiomas: A Narrative Review. Journal of Neurological Surgery Part B: Skull Base. 2021; 82: e33-e44.
- Schick U, Bleyen J, Bani A, Hassler W: Management of meningiomas en plaque of the sphenoid wing. Journal of neurosurgery. 2006; 104: 208-214.
- Cannon PS, Rutherford SA, Richardson PL, King A, Leatherbarrow B, et al. The surgical management and outcomes for spheno-orbital meningiomas: A 7-year review of multi-disciplinary practice. Orbit. 2009; 28: 371-376.
- De Jesús O, Toledo MiM. Surgical management of meningioma en plaque of the sphenoid ridge. Surgical neurology. 2001; 55: 265-269.
- Honeybul S, Neil Dwyer G, Lang D, Evans B, Ellison D, et al. Sphenoid wing meningioma en plaque: A clinical review. Acta neurochirurgica. 2001; 143: 749-758.
- Mirone G, Chibbaro S, Schiabello L, Tola S, George B, et al. En plaque sphenoid wing meningiomas: Recurrence factors and surgical strategy in a series of 71 patients. Operative Neurosurgery. 2009; 65: ons100-ons109.
- Maroon JC, Kennerdell JS, Vidovich DV, Abla A, Sternau L, et al. Recurrent spheno-orbital meningioma. Journal of neurosurgery. 1994; 80: 202-208.