
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A rare case of left-ventricular assist-device fungal obstruction
Mariusz K Szymanski1; Mats T Vervoorn2*; Aryan Vink3; Martinus IJF Oerlemans1; Linda W van Laake1; Monica Gianoli2
1Department of Cardiology, University Medical Center Utrecht, Utrecht, The Netherlands.
2Department of Cardiothoracic Surgery, University Medical Center Utrecht, Utrecht, The Netherlands.
3Department of Pathology, University Medical Center Utrecht, Utrecht, The Netherlands.
*Corresponding Author : Mats T Vervoorn, MD
University Medical Centrer Utrecht, Postbus 85500, 3508 GA Utrecht, The Netherlands.
Email: M.t.vervoorn-4@umcutrecht.nl
Received : Aug 24, 2022
Accepted : Sep 12, 2022
Published : Sep 19, 2022
Archived : www.jcimcr.org
Copyright : © Vervoorn MT (2022).
Keywords: Left ventricle assist device; Fungal infection; Cannula obstruction.
Citation: Szymanski MK, Vervoorn MT, Vink A, Oerlemans MIJF, van Laake LW, et al. A rare case of left-ventricular assist-device fungal obstruction. J Clin Images Med Case Rep. 2022; 3(9): 2061.
Introduction
Left Ventricular Assist Devices (LVADs) have become an established therapy in end-stage heart failure patients as a bridge to transplant, a bridge to candidacy or as destination therapy, resulting in improved prognosis in this group of patients. However, LVAD patients often suffer from complications, which can result in severe morbidity and mortality. One of the most common complications is device-related infections. Although the introduction of third generation centrifugal pumps has improved clinical outcome of these patients [1,2], device-related infections remain an important problem and can lead to serious complications, including pump dysfunction. Whereas most infections are caused by various bacterial species, fungal infections have also been described [3-6]. We present a rare case of inflow and outflow cannula obstruction due to a fungal infectious thrombus in a patient with a HeartMate 3™ (HM3) (Abbott, Chicaco, Il, USA), necessitating pump replacement.
Case description
A 48-year old male with dilated cardiomyopathy due to atruncating mutation in thetitin (TTN) gene, underwent an HM3 LVAD implantation as a bridge to transplant. Throat and rectal swabs collected routinely at admission to the Intensive Care Unit directly after LVAD implantation showed growth of a Candida species, whereas blood cultures were negative and beta-D-glucan was not detected in the patient’s serum. Six days after the implantation the cultures from the tip of the Swan-Ganz catheter and blood cultures were collected and showed growth of Candida albicans. The patient was treated with a combination of various antifungal agents (fluconazole, flucytosine, amphotericin, anidulafunginum), resulting in negative blood cultures 5 days after the start of treatment. There were no signs of fungal endophalmitis. The further post-operative period was uncomplicated and the patient was discharged home3 weeks after implantation, under suppression therapy of anidulafunginum 200 mg od. Multiple blood cultures collected during the first month of follow-up showed no growth of fungal species, but were positive for Enterococcus faecalis and vancomycine was administered for 7 days. During the following weeks there were several episodes of low flow with multiple Pulsatility Index (PI) events reported as well as one episode of vasovagal syncope without evidence of pump dysfunction orarrhythmias, all resolving spontaneously.
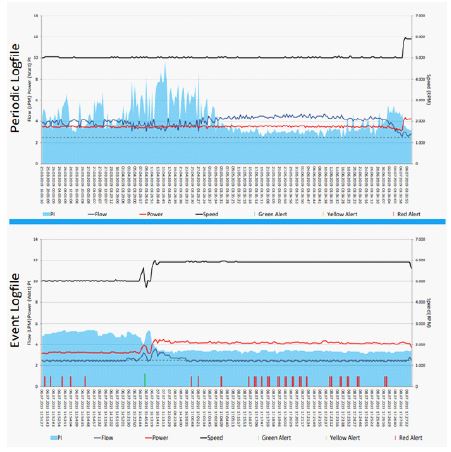
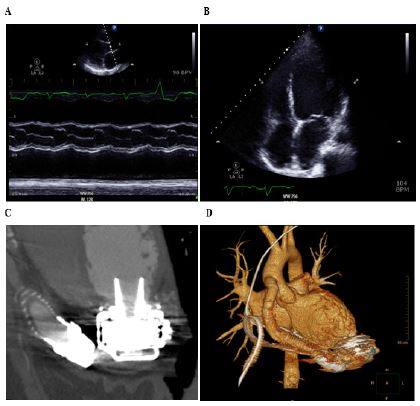
Four months after the implantation the patient was re-admitted because of persistent episodes of low flow. LVAD data analysis revealed a gradual decrease in flow and PI values, with a short increase and subsequent normalization of power values (Figure 1A). Transthoracic echocardiography (Figure 2A and B) showed minimal increase in the left ventriclediameter (75 mm vs 70 mm 1 month after implantation) and the aortic valve fully opening with every beat (mean opening time 0.21 sec), whereas previous echocardiograms showed minimal aortic valve opening (mean opening time of 0,09 sec every third beat). There were no signs of right ventricular failure.Increasing of the RPM had no effect on unloading of the left ventricle and led to only short-lasting increases in flow (Figure 1B). Computed Tomography (CT) scan showed no obstruction in the visualized parts of the inflow cannula and the outflow graft (Figure 2C and D). On transesophageal echocardiogram a suspicion of a mobile structure in the inflow cannula was raised. Due to persistent episodes of low flow an urgent HM3 pump and outflow graft replacement was performed. Examination of the explanted LVAD showed a thrombus-like structure in the inflow cannula and proximal part of the outflow cannula (Figure 3), with no further obstruction in the more distal part of the outflow graft.
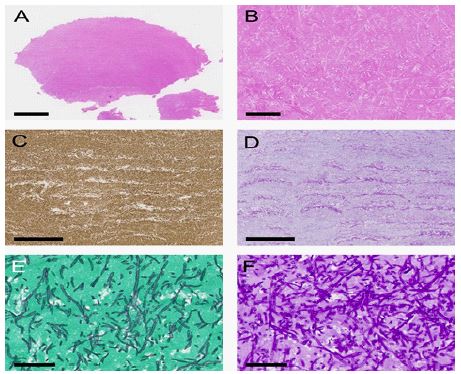
Histology showed a thrombus with abundant presence of pseudohyphae and molecular examination confirmed Candida albicans (Figure 2). Postoperatively the patient received vancomycine and several anti-fungal agents (posaconazol and subsequently isavoconazol), followed by long-termtreatment with fluconazole. Blood cultures collected postoperatively showed no growth of Candida species and beta-D-glucan was not detected in the patient’s serum. The patient recovered quickly, is currently being followed in the out-patient clinic and has not experienced any adverse events since the pump replacement (25 months until now).

Discussion
We present a case of a HM3 pump dysfunction due to obstruction caused by fungal infectious thrombus formation, necessitating pump replacement 4 months after implantation. Fungal LVAD endocarditis has been described before in patients receiving prior generation LVADs, resulting in either pump replacement, (urgent) heart transplantation or death [3-6].
In our case, the patient was colonized with Candida albicans prior to LVAD implantation, as indicated by rectal and nasal swab, and developed asymptomatic fungemia shortly after implantation, which was successfully treated with (suppressive) antifungal therapy. Nevertheless, the patient developed a fungal LVAD endocarditis with infectious thrombus formation, warranting pump replacement. Surprisingly, both CT scan and transthoracic echocardiography were limited in their ability to detect the significant signs of infectious pump thrombosis in our patient and invasive transesophageal echocardiography was warranted before the suspicion was raised. The definitive diagnosis was established from species identification within the obstructive mass following explantation of the device. Importantly, these findings indicate that fungal infectious thrombus formation in an LVAD could present with only discrete and minor changes in echocardiographic findings and LVAD data, as was the case in our patient. Therefore, it should be stressed that clinical diagnosis of fungal LVAD endocarditis with infectious thrombus formation should be considered, regardless of imaging results,in patients with nonspecific signs, symptoms and VAD-related issues, and that tissue specimens from the device should always be collected at the time of surgery for histopathological examination and definitive diagnosis.
Previous case series on fungal LVAD infections indicate that Candida species are the most common pathogens isolated and that these infections are associated with an increased mortality [4,5]. They commonly present with outflow graft obstruction and pump thrombosis, as was the case in our patient. Clinical presentation is often nonspecific, with signs and symptoms such as weight loss, fever and fungemia [5]. In general, clinical manifestation of fungal infections are uncommon in immunocompetent patients. When they do occur, it is often in the setting of immunocompromised patients. Although usually immunocompetent, there is evidence that LVAD implantation itself may result in progressive defects in cell-mediated immunity and increased risk of opportunistic infections, making these patients more susceptible to fungal infections when compared to the general population [4,5].
Given the increased mortality, it is important to note that fungal LVAD infections are difficult to treat and aggressive treatment should be initiated as soon as suspicion is raised. We believe that, in accordance with what is reported in the literature, a multi-modality approach combining both pharmacological and surgical treatment, including pump replacement or high-urgency transplantation listing, should be considered at an early stage.
Currently, there is no evidence that routine use of anti-fungal prophylaxis decreases the risk of fungal infection, even in colonized patients [4]. Furthermore, the International Society for Heart and Lung Transplantation does not recommend the routine use of the anti-fungal prophylaxis in the 2015 guidelines [7]. However, prospective multicenter studies are lacking and our experience suggests that perioperative anti-fungal prophylaxis in patients colonized with Candida species prior to LVAD implantation could be of clinical benefit if initiated at an earlier stage. In our case, rectal and nasal swabs suggest that the patient was colonized prior to implantation and perioperative seeding of the fungus to the newly implanted LVAD could have already occurred before initiation of postoperative eradication therapy six days after implantation. We can theorize that earlier knowledge of colonization and initiation of preoperative fungal eradicative therapy might have resulted in a different clinical course, although this remains speculative. The fact that these patients might be more susceptible to opportunistic infections, may be an additional argument in favor of prophylactic antifungal therapy to prevent fungal LVAD endocarditis.
Conclusion
In conclusion, our case reports illustrates that Candida colonization can lead to fungal LVAD endocarditis and cause serious pump dysfunction, necessitating pump replacement. Even in the presence of clinically significant obstruction, imaging techniques can be limited for diagnosis. The combination of clinical image, LVAD data and imaging is necessary to establish the right diagnosis and treatment. Candida LVAD endocarditis constitutes a serious clinical problem and requires early detection and aggressive treatment, often both pharmacological and surgical. Routine screening for colonization among LVAD recipients should be performedand prophylaxis or aggressive treatment of the colonized patients, even in the absence of symptoms or signs of systemic infection, should be considered.
Declarations
Conflict of interest: M.Szymanski, M. Gianoli, A. Vink, M. Oerlemans, N. de Jonge have no conflicts of interest to declare.
Funding statement: L. van Laake’s employer (University Medical Center Utrecht) receives the fee’s for her consultancy work for Abbott.
References
- Mehra MR, Uriel N, Naka Y, et al. A Fully Magnetically Levitated Left Ventricular Assist Device-Final Report. N Engl J Med. Published online 2019.
- Kormos RL, Cowger J, Pagani FD, et al. The Society of Thoracic Surgeons Intermacs Database Annual Report: Evolving Indications, Outcomes, and Scientific Partnerships. Ann Thorac Surg. Published online 2019.
- Weitzel N, Puskas F, Cleveland J, Levi ME, Seres T, et al. Left ventricular assist device outflow cannula obstruction by the rare environmental fungus Myceliophthora thermophila. Anesth Analg. Published online 2009.
- Aslam S, Hernandez M, Thornby J, Zeluff B, Darouiche RO, et al. Risk factors and outcomes of fungal Ventricular Assist device infections. Clin Infect Dis. Published online 2010.
- Nurozler F, Argenziano M, Oz MC, Naka Y. Fungal left ventricular assist device endocarditis. Ann Thorac Surg. Published online 2001.
- Maly J, Szarszoi O, Dorazilova Z, et al. Case report: A typical fungal obstruction of the left ventricular assist device outflow cannula. J Cardiothorac Surg. Published online 2014.
- Husain S, Sole A, Alexander BD, et al. The 2015 International Society for Heart and Lung Transplantation Guidelines for the management of fungal infections in mechanical circulatory support and cardiothoracic organ transplant recipients: Executive summary. J Hear Lung Transplant. Published online 2016.