
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
The rebound effect of teriflunomide: Case report
Esra Derya Dinc Polat; Ibrahim Acir*; Vildan Yayla
Neurology Department, Bakırköy Dr. Sadi Konuk Training and Research Hospital, Istanbul, Turkey.
*Corresponding Author : Ibrahim Acir
Neurology Department, Başakşehir Çam and Sakura City Hospital, Istanbul, Turkey.
Tel: +90-544-449-8678;
Email: iacir33@gmail.com
Received : Nov 06, 2021
Accepted : Sep 13, 2022
Published : Sep 20, 2022
Archived : www.jcimcr.org
Copyright : © Acir I (2022).
Abstract
Teriflunomide is one of the first-line treatment in Multiple Sclerosis (MS). Cessation of medications can cause increased MS-related disease activity which has been characterized as rebound syndrome (RS). Rebound syndrome is not an expected syndrome when the drug is discontinued especially in first-line treatments. Teriflunomide therapy was discontinued in a twenty-five years old female patient due to pregnancy who was diagnosed with Relapsing-Remitting MS (RRMS). In the patient, clinical symptoms and radiological worsening were seen the 20th week after the cessation. We aimed to discuss through this case that immune system-modifying therapies can cause rebound syndrome, regardless of the mechanism.
Citation: Polat EDD, Acir I, Yayla V. The rebound effect of teriflunomide: Case report. J Clin Images Med Case Rep. 2022; 3(9): 2062.
Introduction
Disease-modifying therapies (DMT) are frequently used in the treatment of Multiple Sclerosis (MS). Teriflunomide, one of the DMTs, effects on T and B cell proliferation by inhibiting the dihydroorotate dehydrogenase enzyme [1,2]. Liver enzyme elevation, hair loss, diarrhea, nausea, headache and teratogenic effects can be seen while teriflunomide therapy [3]. Although it can be used more easily than injectable treatments, patients may stop using the drug due to side effects or possible pregnancy. Rebound syndrome (RS) can be seen in patients with multiple sclerosis if the disease-modifying therapies were discontinued. RS is also defined as the return of the disease activity after 2-6 months of drug cessation [4,5]. We aimed to present the case of a 25-year-old woman with Relapsing-Remitting MS, who developed a severe clinical and radiological symptoms 5 months after discontinuing teriflunomide due to pregnancy.
Case report
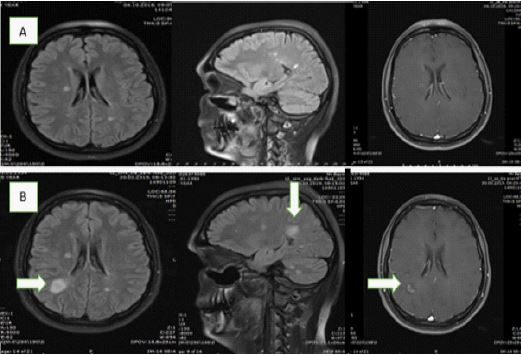
Twenty-five years old female who was diagnosed with RRMS for 6 years was firstly treated with interferon-beta 1a (subcutaneous) 44 micrograms three times per week. Due to the relative side effects of the injection therapy, the patient’s therapy was switched to teriflunomide in the second year of her treatment and has been followed up for 4 years without attack. The patient mentioned that she was considering pregnancy while she was under the teriflunomide treatment so teriflunomide was discontinued in the patient, and rapid elimination process was initiated. After rapid elimination, the drug level was observed below 0.02 mg/L and it was explained that she would be suitable for fertilization 1.5 months later. She applied to the outpatient clinic with the complaint of blurred vision at the 20th week after stopping the teriflunomide therapy. Furthermore it was 8 weeks after the drug level dropped below 0.01 mg/L. Optic neuritis attack was diagnosed in the patient who did not have the motor and sensory deficits in her neurological examination. Increased T2 hyperintense demyelinating plaques with contrast enhancement were detected in cranial Magnetic Resonance Imaging (MRI) scans compared to previous MRIs. (Figure 1). Due to the severe clinical progressing and radiological worsening, serological tests were applied for ruling out infectious or inflammatory disorders. It was considered as RS and pulse steroid therapy was given for five days. Then, glatiramer acetate treatment was started, which was thought to be more suitable for the patient in terms of teratogenicity during pregnancy.
Discussion and Conclusion
Teriflunomide acts by reducing the number of activated T and B cells, and also by reducing proinflammatory cytokines [6]. Teriflunomide is used in the first-line treatment of MS, and rebound syndrome is rarely seen after drug discontinuation in first-line drug treatments. As new disease-modifying drugs (DMT) become available in the treatment of MS, medication discontinuation is often made for medication switches. In the washout periods, RS can be seen and disease reactivation usually occurs between 1-6 months following drug cessation [7,8]. In our case, the contrast-enhancing lesion has been seen after the 20th week of teriflunomide discontinuation because of the pregnancy. The time from drug withdrawal to the rebound syndrome was similar to the cases that have been reported in the literature [7]. However, there is a rapid restoration of cellular immunity following the cessation of the drug, the exact mechanism of RS in teriflunomide has not been known. The fact that rebound syndrome is also seen in teriflunomide such as natalizumab, fingolimod [9]. It is interesting in terms of showing that different mechanisms of medications may also cause RS. Additionally, it can be considered that drugs that reconstruct the immune system can cause RS independently of the mechanism.
The patient whose teriflunomide treatment had to be discontinued was seen severe clinical symptoms and MRI worsening after drug discontinuation and it is important that has been thought the first-line treatment interruption also causes RS. We wanted to point out that drugs that change the immune system structure, regardless of the mechanism, can cause RS. In addition, we wanted to emphasize that close following-up of patients should be continued in cases who teriflunomide should be discontinued.
References
- Hafler DA. Multiple sclerosis. J Clin Invest. 2004; 113: 788-94.Teriflunomide and Its Mechanism of Action in Multiple Sclerosis
- Liblau RS, Gonzalez-Dunia D, Wiendl H, et al. Neurons astargets for T cells in the nervous system. Trends Neurosci. 2013.
- Bar-Or A, Pachner A, Menguy-Vacheron F, Kaplan J, Wiendl H. Teriflunomide and its mechanism of action in multiple sclerosis. Drugs. 2014; 74[6]: 659-674. doi:10.1007/s40265-014-0212-x
- R.G. Beran, Y. Hegazi, R.S. Schwartz, D.J. Cordato, Rebound exacerbation multiple sclerosis following cessation of oral treatment, Mult. Scler. Relat. Dis. 2013; 2: 252-255.
- JB Havla, HL Pellkofer, I Meinl, LA Gerdes, R Hohlfeld, T Kümpfel. Rebound of disease activity after withdrawal of fingolimod [FTY720] treatment. Arch. Neurol. 2012; 69: 262-264.
- Scott LJ. Teriflunomide: A Review in Relapsing–Remitting Multiple Sclerosis. Drugs. 2019; 79: 875-886. https://doi.org/10.1007/s40265-019-01135-8.
- Fuerte-Hortigón A, López Ruiz R, Hiraldo J, et al. Rebound after discontinuation of teriflunomide in patients with multiple sclerosis: 2 case reports. Mult Scler Relat Disord. 2020; 41: 102017. doi:10.1016/j.msard.2020.102017.
- SE Hatcher, E Waubant, B Nourbakhsh, E Crabtree-Hartman, JS Graves. Rebound syndrome in patients with multiple sclerosis after cessation of fingolimod treatment, JAMA Neurol. 2016; 73: 790-794.
- Barry B, Erwin AA, Stevens J, Tornatore C. Fingolimod Rebound: A Review of the Clinical Experience and Management Considerations. Neurol Ther. 2019;8[2]:241-250. doi:10.1007/s40120-019-00160-9.