
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Unusually elevated CA19.9 with adnexal mass: Does it lead to some conclusions or confusion?
MD Ray*; Pallabika Mandal
All India Institute of Medical Sciences, New Delhi, India.
*Corresponding Author : MD Ray
Addtional Professor, Department of Surgical Oncology, AIIMS, New Delhi, India.
Tel: 91-971-677-2975;
Email: drmajormdrayaiimsdelhi@aiims.edu
Received : Aug 26, 2022
Accepted : Sep 15, 2022
Published : Sep 22, 2022
Archived : www.jcimcr.org
Copyright : © Ray MD (2022).
Abstract
Elevated level of CA19.9 is usually associated with malignancies of the hepatobiliary and the pancreatic system. It not only helps to diagnose the malignancy, but also ever high levels can indicate advanced or metastatic diseases [1].
However in rare instances elevated CA19.9 has been found in patients with adnexal masses. This is not only uncommon but also confounding, while trying to ascertain the nature of the ovarian mass and to determine the optimal surgical management in young and premenopausal patients.
We would like to report three such cases who had presented with ovarian mass and very high levels of CA 19.9 which led us to diagnostic dilemma and much confusion.
Citation: Ray MD, Mandal P. Unusually elevated CA19.9 with adnexal mass: Does it lead to some conclusions or confusion?. J Clin Images Med Case Rep. 2022; 3(9): 2067.
Background
When young patient presents with a larger adnexal mass, there can be dilemma regarding whether the mass is benign or malignant. It becomes important to determine the extent of surgery and many a times fertility preservation is of upmost importance specially in young patient.
Usually younger patient with an adnexal mass undergoes test for germ cell markers: SerumAFP, BHCG, and LDH. But we find many authors also get serum CA 125 and CA19.9 done as routine.
Unusually high serum CA19.9 in such a patient is a diagnostic challenge. There are instances where elevated CA19.9 has been associated with teratoma of ovary or cystadenoma of ovary in limited literature.
We had three such patients who had similar clinical picture but different final histopathology report.
Case one
25-year-old unmarried girl presented with pain the lower abdomen for 2 weeks. She had no menstrual irregularities. UlUltrasound report showed bulky left ovary with a cystic lesion of size 10x8 cm and moderate free fluid in the pelvis. MRI pelvis showed a complex cystic lesion of left ovary with solid component along left lateral margin. Right ovary was seen separately and found normal. For a complex cyst usually, all related tumor markers are advised. In this girl Serum Ca 125 was 1999 U/ml (highly elevated), serum CA19.9 >1200 U/ml (Highly elevated), Serumh CG< 1.2 (normal), Serum AFP 3.99 (normal), Serum LDH 387 (normal). The Serum CA19.9 was so elevated that it was not understood as hepatobiliary system was normal and resulted in confusion regarding the nature of the cyst. She was planned for fertility preserving staging laparotomy and intraoperative frozen section. Exploratory laparotomy was done. Large well circumscribed lesion was arising from and replacing the entire left ovary. Left salphingo0-opherectomy was done and frozen section showed negative for malignancy likely adenofibroma. The final histopathology report confirmed adenofibroma.
Case two
23 year old unmarried lady presented with sudden onset pain in the lower abdomen for which she was investigated at a private centre and referred to us. She had regular menstrual history. Ultrasound showed a 7.5 x 6.3 cm right adnexal mass.


CECT abdomen showed 8 x 6 cm multi septate loculated thick walled complex pelvic cystic lesion. It also showed mild ascites and omental fat stranding. Serum Ca 125 932 U/ml (highly elevated), Serum CA 19.9-21209.20 U/ml (highly elevated), serum hCG< 1.2 (normal), serum AFP 1.29 ng/ml (normal) and serum LDH 175 U/l (normal). This case almost mirrored the previous case and they had presented almost simultaneously. She was planned for exploratory laparotomy and frozen section. Intraoperatively dense adhesions were present between the sigmoid colon, rectum, omentum and the uterine wall. Left ovarian chocolate cyst was present. Left ovarian cystectomy was done. Final histopathology report showed endometriotic cyst.
Case three
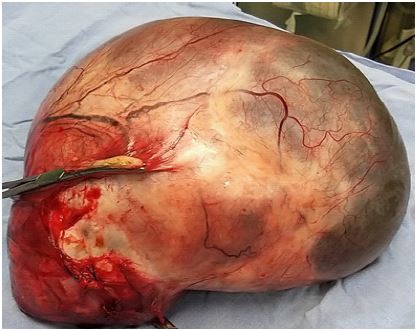
21 year old unmarried lady presented gradual onset pain in the abdomen associated with lower abdominal swelling. She had normal menstrual history. She was referred from a private centre where she was primarily investigated. USG showed a large cystic lesion which occupied the entire pelvis, Bilateral paracolic gutters going up to the epigastrium. Organ of origin could not be ascertained but right ovary was not separately seen. CECT showed a 30 x 25 cm cystic lesion with no soft tissue component. Organ of origin was indefinite and differential diagnoses were pancreatic cyst, mesenteric cyst or ovarian cyst. Serum CEA was 3.53 (normal), Serum CA125 45.93 (slightly elevated) and CA19.9 was 1138.25 (highly elevated). She was planned for exploratory laparotomy and fertility preserving procedure. Intraoperatively, 25 x 25 cm large cystic mass was seen arising from the right ovary. Right salphingo oophorectomy was done. Frozen section showed no malignancy. Final histopathology report showed mucinous cystadenoma.
All the three patients had normalization of the elevated Sr CA19.9 within 6 months of surgery. 16.2 Units/ml, 39.7 Units/ml and 19.3 Units/ml respectively
Discussion
CA19.9 antigen was first reported by Koprowski et al. in 1981. It is a sialylated Lewis A antigen, which is associated with mucins in gastrointestinal adenocarcinomas [1].
Cho and Kyung concluded that CA19.9 was much more elevated in mucinous borderline and malignant tumours than in benign tumours [2]. In contrast, other studies have suggested that levels of CA19.9 are not correlated with histological subtype (i.e., benign, borderline, and malignant) or tumour stage.
Elevation of CA19.9 was also reported in some cases of mature cystic teratoma [3].
There have been multiple case reports where elevation CA19.9 is associated with torsion of benign ovarian cysts. The primary histology of these cysts has been teratoma [2], adenofibroma [3] and mucinous cyst adenoma [5]. However in our series there was no torsion in any of these patients and no history of acute pain.
There are certain reports that have associated elevated adenofibroma with elevated serum CA19.9 and some are associated with torsion.
There have been a lot of reports for elevated CA19.9 in benign ovarian cyst however Kelly et al showed that preoperative CA19.9 levels cannot predict whether a suspected ovarian mucinous tumour is benign, borderline or malignant. Markedly elevated CA19.9 levels (>1000 U/ml) may be found in benign mucinous neoplasms as well as in borderline and malignant tumours [6].
In general serum CA19.9 can be elevated slightly in endometriosis and many reports are seen, however the very high levels (>1000) as seen in the second case has been rarely reported [7].
As per as CA 125 (normal range: 0-35 U/ml) is concerned, in first two cases it was significantly elevated. A part from ovarian, fallopian, endometrial and primary peritoneal cancers CA 125 may increase in many benign diseases like endometriosis, pelvic inflammatory disease, ovarian cyst etc. But highly elevated serum CA 125 leads to confusion rather than conclusion like two cases in our centre.
Conclusion
CA19.9 is not a good marker for malignancy in case of adnexal mass in a premenopausal patient. Its elevation neither predicts malignancy nor indicates any particular histology. It however does add to the diagnostic dilemma of the clinician and patient’s distress though in hepatobiliary malignancies its higher elevation indicates poor prognosis.
Thereby CA 19.9 should not be tested as routine along with Ca 125 or germ cell tumor markers specially in younger patient with adnexal mass. Significantly elevated Ca 125 along with CA 19.9 in benign cases lead to confusion rather conclusion.
Declarations
Conflicts of interest: There is written consent from the patients.
Conflicts of interest: None.
References
- Maisey NR, Norman AR, Hill A, Massey A, Oates J, Cunningham D, et al. CA19-9 as a prognostic factor in inoperable pancreatic cancer: The implication for clinical trials. Br J Cancer. 2005; 93: 740–743.
- Cho HY, Kyung MS. Serum CA19-9 as a predictor of malignancy in primary ovarian mucinous tumors: A matched case-control study. Med Sci Monit Int Med J Exp Clin Res. 2014; 20: 1334–1339.
- Yesilyurt H, Seckin B, Aktulay A, Ozyer S. Age-stratified analysis of tumor markers and tumor characteristics in adolescents and young women with mature cystic teratoma. J Chin Med Assoc JCMA. 2018; 81: 499–5
- Suh DS, Moon SH, Kim SC, Joo JK, Park WY, Kim KH. Significant simultaneous changes in serum CA19-9 and CA125 due to prolonged torsion of mature cystic teratoma of the ovary. World J Surg Oncol [Internet]. 2014 Nov 22 [cited 2020 Jul 31]; 12. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4247622/
- Chuang CC, Chang DY, Chen RJ, Cheng WF, Chow SN, et al. Torsion of an ovarian borderline tumor with extreme serum tumor markers: a case report. Zhonghua Yi Xue Za Zhi Chin Med J Free China Ed. 1995; 55: 278–282.
- Kelly PJ, Archbold P, Price JH, Cardwell C, Mc Cluggage WG. Serum CA19.9 levels are commonly elevated in primary ovarian mucinous tumours but cannot be used to predict the histological subtype. J Clin Pathol. 2010; 63: 169–173.
- Takemori: Ovarian chocolate cyst with markedly elevated... - Google Scholar [Internet]. [cited 2020 Jul 31].