
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Ghost lesions of the central nervous system:
Misleading or revealing the diagnosis?
Mahdi Adouania1,2*; Nadia Ben Ali1,2,3; Mariem Ben Mahmoud1,2,3; Hela Jamoussi1,2,3; Saloua Fray1,2,3;
Mohamed Fredj1,2
1Department of Neurology, Charles Nicolle Hospital, Tunis, Tunisia.
2Research Laboratory LR12SP01, Charles Nicolle Hospital, Tunisia.
3Faculty of Medicine, Tunis El Manar University, Tunis, Tunisia.
*Corresponding Author : Mahdi Adouania
National Institute of Neurology, Mongi-Ben Hamida, Tunis 1007, Tunisia.
Email: mahdi.adouania@gmail.com
Received : Aug 26, 2022
Accepted : Sep 15, 2022
Published : Sep 22, 2022
Archived : www.jcimcr.org
Copyright : © Adouania M (2022).
Abstract
Vanishing lesions of the CNS also known as Ghost lesions can be a radiological feature of various neurological disorders mainly tumoral followed by inflammatory diseases of the CNS. Vasculitis such as Behcet Disease (BD) is considered as a leading cause of demyelinating disorders with ghost lesions on brain MRI. As a result, following a specific clinical approach is pivotal for definitive diagnosis in order to adapt the treatment and assess the outcome. Here, we report 3 cases of ghost lesions on cerebral MRI as a radiological finding in CNS vasculitis: Neurobehcet Disease (NB).
Citation: Adouania M, Ben Ali N, Mahmoud MB, Jamoussi H, Fray S, et al. Ghost lesions of the central nervous system: Misleading or revealing the diagnosis?. J Clin Images Med Case Rep. 2022; 3(9): 2069.
Introduction
Spontaneously disappearing lesions of the CNS, also known as ‘ghost’ lesions, may be a radiological feature of a large spectrum of neurological disorders. Not uncommonly, this scenario is seen in many diseases like Multiple Sclerosis (MS), metastatic or primary brain tumors, infections, and acute disseminated encephalomyelitis [1]. This phenomenon is challenging in daily practice and has not been addressed in depth in the literature. There is no standard definition for vanishing brain lesions, however, it can be defined as reduction or disappearance of a brain lesion spontaneously or after steroid treatment to ≤70% of its size before establishing its definitive diagnosis [2].
Most vanishing lesions of the central nervous system are eventually diagnosed as primary central nervous system lymphoma (PCNSL) or as an inflammatory disease of the CNS [1]. This unusual radiological finding presents diagnostic difficulties and thus leads to confusion in determining treatment options.
The aim of this study is to addresses the management of transient clinico-radiological syndroms of the CNS with spontaneous or after treatment radiological improvement.
Here, we report 3 cases of patients with vanishing lesions on brain MRI in whom difficulty was encountered in the establishment of a diagnosis.
Case descriptions
Case 1 : A 51-year-old female, with medical history of hypertension, diabete and dyslipidemia, admitted to our department in 2014 with an acute onset of weakness affecting the right arm and leg regressive within 3 days followed by a second clinical event: vertigo and swallowing difficulties. Neurological findings were compatible with a right pyramidal syndrom while oral apthosis were found on general examination.
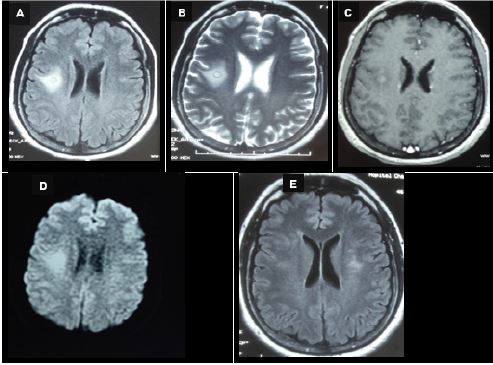
Brain-MRI revealed presence of a large intra-axial mass in the right parietal lobe. It showed hyperintense signals in T2W and FLAIR images and peripheral Gadolinium (Gd) enhancement creating the ‘target lesion‘ (Figure 1). Spectroscopy was not performed.
Routine laboratory tests including renal function tests, plasma glucose level, and serum electrolytes were normal. The search for proteinuria was negative.
Cerebral spinal fluid study showed lymphocytic pleocytosis [80/mm3, 80% lymphocytes] with protein level at 0,54. No Oligoclonal Bands (OCB’s) were detected in the CSF.
Initial testing for infectious etiologies was negative, including bacterial culture, polymerase chain reaction for tuberculosis, HIV and syphilis serologies.
Testing for autoimmune etiologies was also unrevealing including antinuclear antibodies and aquaporin-4 antibody (NMO-IgG).
HLA phenotype testing was compatible with HLA B51.
The Visual-Evoked Cortical Potential (VEP) study has showed delayed P-100 latency demyelinating optic neuritis.
The diagnosis of neurobehcet disease was retained according to the International Criteria Of Behcet Disease (ICBD) 2014. The patient was treated with intravenous methylprednisolone (1 g/day) during 5 days followed by oral prednisolone (1 mg/ kg/day) with progressive tapering. Clincial follow-up showed a complete recovery of the right limb paresis. A 10 months follow- up brain MRI showed regression of the right parietal lobe lesion with appearance of a new leftparietal one (Figure 1).
Case 2: A 36-year-old male, with medical history of psoriasis, presented to our department in 2010 with acute onset of holocranial headache without blurring vision or nausea/vomiting followed by onset of generalized epileptic seizures. Neurological examination was normal. Her fundoscopic examination showed no signs of papillar edema. General examination was normal.
Routine laboratory tests including blood test, renal function tests, plasma glucose level, and serum electrolytes were normal. The search for proteinuria was negative.
Cerebral spinal fluid study showed normal cellular composition with protein level at 0,54. No Oligoclonal Bands (OCB’s) were detected in the CSF.
Initial testing for infectious etiologies was negative, including bacterial culture, polymerase chain reaction for tuberculotuberculosis, HIV and syphilis serologies. Testing for autoimmune etiologies was also unrevealing including antinuclear antibodies and aquaporin-4 antibody (NMO-IgG).
Electroencephalography (EEG) showed backround slowing in right frontal region.
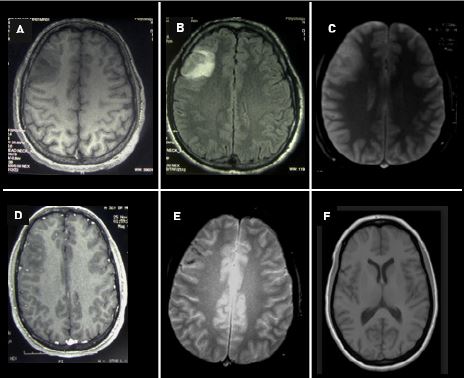
Brain MRI revealed right frontal cortical-subcortical lesion with no mass effect. It showed hypointense signals in T1images and hyperintense signals in T2W/Flair images with mild heterogenous gadolinium enhancement (Figure 2).
At this stage, differential diagnosis suggested for our patient were: An hemorragic tumor, an hemorragic stroke, a giant aneurysm and mainly inflammatory pseudo-tumoral brain lesion or ‘tumor-Like Lesions’.
Steretoaxic biopsy was therefore suggested for definitive diagnosis but was delayed for technical issues.
The decision was to review the initial brain MRI. Findings of linear cortical hypointensity ‘cord sign’ of the right frontal lobe on T2-weighted Gradient-Echo MRI Sequences (GRE) supported the diagnosis of isolated cortical vein thrombosis revealed by acute encephalitis-like presentation.
Treatment with anticoagulants was not initiated giving the isolated cortical vein thrombosis.
The patient was seizure free on clinical follow-up. However, general examination showed oral and genital ulcers in addition to pseudofolliculitis.
A 6 month follow-up brain MRI showed complete regression of the right frontal lesion (Figure 2).
The final diagnosis retained was a neurobehcet disease according to the 2014 ICBD criteria.
Case 3: A 40-year-old female, with no past medical history, admitted to our department for a rapidely progressive hemiparesis of the right upper and lower limbs. Neurological findings were compatible with a right pyramidal syndrom. Multiple oral ulcers were found on general examination.
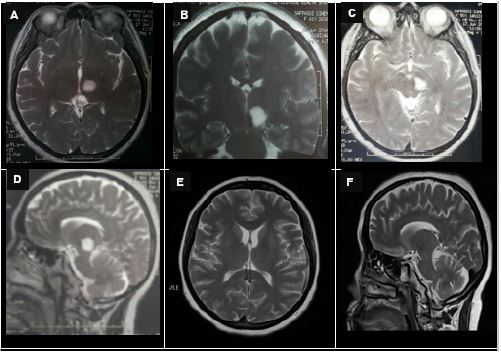
Brain-MRI revealed presence of a large well-limited pedonculo-thalamic left lesion. It showed hyperintense signals in T2W and FLAIR images with gadolinium (Gd) enhancement. Hyperintense image on Diffusion-Weighted MRI (DWI) with no restriction of ADC. MR spectroscopic study was normal (Figure 3).
Differential diagnosis suggested were mainly inflammatory CNS disorders (Multiple sclerosis, neurolupus, neurobehcet etc). Tumoral and infectious etiologies were also suggested.
Ophthalmologic examination showed retinal vasculitis.
Routine laboratory tests including blood test, renal function tests, plasma glucose level, and serum electrolytes were normal. The search for proteinuria was negative.
Cerebral Spinal Fluid (CSF) study showed normal cellular composition with normal protein level. Oligoclonal Bands (OCB’s) were detected in the CSF with a type 3 pattern.
Initial testing for infectious etiologies was negative, including bacterial culture, polymerase chain reaction for tuberculosis, HIV and syphilis serologies.
Testing for autoimmune etiologies was also unrevealing including antinuclear antibodies and aquaporin-4 antibody (NMO-IgG).
HLA phenotype testing was compatible with HLA B51.
The Visual-Evoked Cortical Potential (VEP) study showed bilateral axonal optic neuritis.
The final diagnosis retained was a neurobehcet disaese according to the 2014 ICBD criteria.
The patient was treated with intravenous methylprednisolone (1 g/day) during 5 days followed by oral prednisolone (1 mg/kg/day) with progressive tapering. Clinical follow-up showed a complete recovery of the right limb paresis. A 12 months follow-up brain MRI showed regression of the pedonculo-thalamic lesion (Figure 3).
Discussion
Behcet Disease (BD) is a systemic vasculitis which involves the central nervous system in up to 50 % of cases [3]. Neurological symptoms are often correlated with radiological findings. Currently the most used diagnostic criteria for Behçet Disease (BD) is the International Criteria for Behçet’s Disease (ICBD) [4]. NBD can be separated into two main forms: parenchymal and extraparenchymal (cerebrovascular) presentations. The parenchymal CNS involvement occurs up to 70% with manifestations including: Brainstem symptoms, cerebral symptoms, myelopathy, optic neuropathy, multifocal symptoms [5].
The extraparenchymal form occurs in up to 35% of cases [6]. Clinical manifestations may include: Acute meningeal syndrome, intracranial hypertension (pseudo-tumor cerebri) and cerebral venous thrombosis with cortical vein thrombosis as inaugural feature in 8-16% [5].
MRI has a major role not only in asserting the diagnosis ofneurobehçet disease but also in understanding its physiopathology, giving the difficulties to obtain histopathological studies [6].
In the parenchymal form of NBD, the lesions are usually multiple small foci of high intensity on T2 weighted sequences without predilection for the periventricular regions [8]. The lesions interests mainly the white matter (70%), the brainstem (60%), the basal ganglia and the thalamus (40%). However, the most suggestive brain MRI lesion in NBD is the mesocephalo-diancephalic junction [6].
Long-term brain MRI follow-up in NBD is pivotal to assess the outcome of the disease both spontaneously and under treatment. The radiological evolution of brain lesions in NBD can be heterogenous as reported by various studies and descriped in our case series. It is estimated that 39% of the initial lesions will disappear while 35% will become smaller and 26% remain unchanged [9].
This indicates that a normal MRI cannot exclude a previous neurological event in Behcet disease [9].
The radiological reversibility of brain MRI lesions in NBD, as illustrated in our case series, may reflect different physiopathological mecanisms. In parenchymal presentation of NBD, it can be secondary to a reversible breakdown in blood-brain barrier probably related to inflammation rather than gliosis or infarction [7].
However, in non parenchymal presentation, it can be explained by the importance of vasogenic edema that will disappear on follow-up MR images without sequelae [10].
Conclusion
Vanishing MRI lesions of the CNS may lead to misdiagnosis of several neurological disorders. The prognosis for patients with these diseases relies to a significant extent on the clinical approach adapted by the clinician. In fact, an early and definitive diagnosis is the key to successful outcomes.
Declarations
Statement of authors’ contribution: All authors contributed equally to the study conception and\or study design and\or data collection and\or data analysis and\or results interpretations and\or manuscript writing and\or manuscript correction and\or proof Reading and\ or manuscript submission.
All authors have agreed to this final version of the paperbeing submitted to journal of clinical images and medical case reports.
Declaration of conflicting interests: The Author(s) declare(s) that there is no conflict of interest.
Funding acknowledgement: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Financial benefits to the authors: None.
References
- Hunt MA, Jahnke K, Murillo TP, Neuwelt EA. Distinguishing primary central nervous system lymphoma from other central nervous system diseases: A neurosurgical perspective on diagnostic dilemmas and approaches. Neurosurg Focus. 2006; 21: E3.
- Hamed SA, Mekkawy MA, Abozaid H. Differential diagnosis of a vanishing brain space occupying lesion in a child. World J Clin Cases. 2015; 3: 956-964.
- Siva A, Altintas A, Saip S. Behçet’s syndrome and the nervous system. Curr Opin Neurol. 2004; 17: 347-357.
- International Team for the Revision of the International Criteria for Behçet’s Disease (ITR-ICBD). The International Criteria for Behçet’s Disease (ICBD): A collaborative study of 27 countries on the sensitivity and specificity of the new criteria. J Eur Acad Dermatol Venereol. 2014; 28: 338-347.
- Kalra S, et al. A. Diagnosis and management of Neuro-Behçet’s disease: International consensus recommendations. J Neurol. 2014; 261: 1662-1676.
- Mohamed C, Najib K, Essaadouni L. Radiological findings in Behçet disease. Pan Afr Med J. 2015; 20: 51.
- Patel DV, Neuman MJ, Hier DB. Reversibility of CT and MR findings in neuro-Behçet disease. J Comput Assist Tomogr. 1989; 13: 669-673.
- Afshin Borhani Haghighi, Sirous Sarhadi, Siamak Farahangiz. MRI findings of neuro-Behcet’s disease. Clin Rheumatol. 2011; 30: 765-770.
- Gerber S, et al. Long-term MR follow-up of cerebral lesions in neuro-Behçet’s disease. Neuroradiology. 1998; 38: 761–768.
- Vuolo L, et al. L. Reversibility of brain lesions in a case of Neuro-Behçet’s disease studied by MR diffusion. Neurol Sci. 2010; 31: 213-215.