
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Left leg swelling: A case of May-Thurner syndrome
Sangya Sharma1; Brian Monaco2*; Neeraj Singh2
1Edward Via College of Osteopathic Medicine, Blacksburg, Virginia, USA.
2Department of Internal Medicine, Willis Knighton Health System, USA.
*Corresponding Author : Brian Monaco, MD,
Internal Medicine, Willis Knighton Health System, Shreveport, LA-71103, USA.
Phone: (318) 629-3099;
Email: Bmonacomdim@gmail.com
Received : Aug 26, 2022
Accepted : Sep 16, 2022
Published : Sep 23, 2022
Archived : www.jcimcr.org
Copyright : © Monaco B (2022).
Abstract
May-Thurner Syndrome is a left common iliac vein thrombosis caused due to its compression by right common iliac artery, an anatomical variant that is underreported. We report the case of a 52 year old female who presented with left leg swelling and was diagnosed with May-Thurner Syndrome. She underwent an iliac vein thrombectomy and was discharged on life-long anticoagulants.
Keywords: May-Thurner; Deep vein thrombosis; Rightcommon iliac artery; Left common iliac vein; Apixaban.
Abbreviations: MTS: May Thurner Syndrome.
Citation: Sharma S, Monaco B, Singh N. Left leg swelling: A case of May-Thurner syndrome. J Clin Images Med Case Rep. 2022; 3(9): 2070.
Case presentation
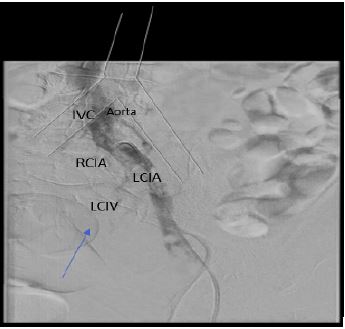
A 52 year old presented with complaints of left leg pain and swelling of four days duration. The examination findings were normal except mild tenderness of left leg without erythema. Venous duplex ultrasound of the left leg revealed deep vein thrombosis extending to proximal left common femoral vein. CT scan of the abdomen and pelvis with IV contrast (Figure 1) also confirmed deep vein thrombosis involving the left common iliac vein. There was compression of left iliac vein by right common iliac artery. This finding was described with May-Thurner Syndrome, or Iliac Vein Compression syndrome, which likely contributed to the patient’s left leg deep vein thrombosis.
The patient had elevated D-dimer levels and factor VIII activity assay. She was started on enoxaparin 30 mg subcutaneously every 12 hours. She underwent a balloon thrombectomy (Figure 2) with stent placement and had subsequent resolution of swelling in the affected leg. The patient was discharged with plans to continue lifelong Apixaban 5 mg BID to prevent future recurrence.

Discussion
May Thurner Syndrome is defined as extrinsic venous compression by the arterial system against bony structures in the iliocaval venous territory, most commonly of the left common iliac vein by the right common iliac artery [3]. It develops in individuals with an anatomic variant in which the right common iliac artery overlies and compresses the left common iliac vein against the lumbar spine [2]. Clinical phases of MTS include a prolonged asymptomatic period of left iliac vein compression followed by the gradual development of an intraluminal venous fibrous band (ie, spur), which can subsequently progress to an acute unilateral left iliofemoral DVT [5].
Prevalence of MTS is unknown for certain and is likely underestimated, largely because most individuals with this anatomic anomaly remain asymptomatic [3]. Among symptomatic patients, MTS has been estimated to be the underlying etiology in 2 to 5 percent of patients [3]. A greater than 70% compression of the iliac vein is needed to cause DVT in MTS [4]. MTS is more common in females than in males and occurs most frequently between the second and fourth decades of life [4]. Research suggests that a female’s pelvis exhibits more of an accentuation of the lumbar lordosis that pushes the lower lumbar vertebrae anteriorly, thereby compressing the left common iliac vein against the right common iliac artery [5].
Duplex ultrasound is used initially for diagnostic purposes for patients with MTS with thrombosis [1]. For MTS without thrombosis, noninvasive venous imaging such as CT or MR venography should be used for diagnosis and intervention of the deep leg veins [1].
Treatment recommendations differ between thrombotic and nonthrombotic MTS [3]. For nonthrombotic MTS with no or mild symptoms, treatment is conservative such as compression stockings [1]. For nonthrombotic MTS with moderate to severe symptoms, treatment is angioplasty and stenting of affected segment [3]. For thrombotic MTS with no contraindications to lytic therapy, such as in this case, treatment begins with full therapeutic anticoagulation [3].
Medical treatment with anticoagulation alone is associated with suboptimal outcomes in those with MTS. With successful treatment of MTS, rates of post-thrombotic syndrome are less than 10 percent [3]. Without treatment, post-thrombotic syndrome is associated to occur in 80 to 90 percent of patients [3].
Conclusion
In conclusion, May-Thurner Syndrome is an uncommon and undiagnosed cause of DVT resulting from Iliac vein compression. Clinical symptoms and physical signs do not always correlate with imaging results. Endovascular therapy, a minimally invasive approach to treating venous lesions, is an effective treatment option for this condition, followed by long term anticoagulation.
References
- Mangla A, Hamad H. May Thurner Syndrome. [Updated 2022 May 14]. In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554377/
- Sharafi S, Farsad K. Variant May Thurner syndrome: Compression of the left common iliac vein by the ipsilateral internal iliac artery. Radiol Case Rep. 2018; 13: 419-423.
- Mousa AY, Abu Rahma AF. May-Thurner syndrome: Update and review. Ann Vasc Surg. 2013; 27: 984–995.
- Baloch ZQ, Hussain M, Ayyaz M, Dagli N, Abbas SA, et al. May-Thurner Syndrome Presenting as Acute Unexplained Deep Venous Thrombosis. Ann Vasc Surg. 2018; 53: 266.e1-266.e3.
- Harbin MM, Lutsey PL. May-Thurner syndrome: History of understanding and need for defining population prevalence. J Thromb Haemost. 2020; 18: 534-542. https://doi.org/10.1111/jth.14707