
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
A case of respiratory tract infection from Bordetella hinzii
in an immunocompetent patient
Sangya Sharma1; Kamal Masri2*
1Edward Via College of Osteopathic Medicine, Blacksburg, Virginia, USA.
2Department of Pulmonary Disease/Critical Care Medicine, Willis Knighton Health System, USA.
*Corresponding Author : Kamal Masri, MD
Pulmonary Disease/Critical Care Medicine, Willis Knighton Health System, Shreveport, Louisiana, USA.
Phone: (318) 212- 8159;
Email: kmasrimd@gmail.com
Received : Aug 26, 2022
Accepted : Sep 16, 2022
Published : Sep 23, 2022
Archived : www.jcimcr.org
Copyright : © Masri K (2022).
Abstract
Bordetella hinzii is a primarily zoonotic organism and rarely affects immunocompetent individuals. We report the case of a healthy 45 year old male who presented with chronic cough and dyspnea and was diagnosed with Bordetella hinzii infection of the lower lungs from imaging and bronchoscopy. He was then discharged on a course of antibiotic treatment.
Keywords: Bordetella pertussis; Bordetella hinzii; Immunocompromised.
Citation: Sharma S, Masri K. A case of respiratory tract infection from Bordetella hinzii in an immunocompetent patient. J Clin Images Med Case Rep. 2022; 3(9): 2071.
Case presentation
A healthy 45 year old male presented with an ongoing history of cough and shortness of breath for four months. He had a history of recurrent sinusitis and seasonal allergies. He was placed on multiple course of oral antibiotics and steroids with partial improvement in his symptoms.
His overall labs and urinalysis were unremarkable. Immunology/serology were negative for Aspergillus, Cryptococcus, Coccidiocides, and Histoplasma antibodies. Histoplasma antigen was negative in both serum and urine. His expectorant was negative for any acid-fast bacilli.
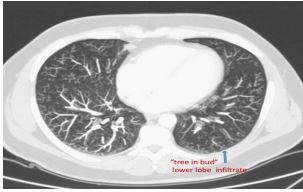
The patient’s chest x-ray and CT angiography were unremarkable. The CT scan of the lung with contrast (Figure 1) showed bronchial wall thickening and tree-in-bud infiltrate predominantly involving the lower lobes, hinting at possible malignancy or atypical infection.
The patient subsequently underwent ultrasound-guided bronchoscopy. Findings included thick endobronchial mucus with diffuse inflammation of the airway. Bronchioalveolar lavage (Figure 2) was performed in the right upper lobe apical segment and sent for cell count and bacterial/viral/fungal analyses. There were no malignant cells, but sample cultures were positive for Bordetella hinzii. The patient was administered IV piperacillin/tazobactam and discharged after 2 days with PO amoxicillin/clavulanate 6.5 mg BID for 10 days.
Discussion
B. hinziiis a species of gram-negative coccobacilli that exhibit weaker virulence than B. pertussis because of the reduced activity of the Adenylate Cyclase Toxin (ACT) [1]. This is due to decreased binding affinity of B. hinziito calmodulin, the eukaryotic activator of the B. pertussis ACT and due to the lack of the cyaC gene needed to acylate the ACT [1]. Additionally, B. hinzii is frequently resistant to many antimicrobial drugs, including β-lactams, cephalosporins, and quinolones [2]. Reported isolates have been susceptible to piperacillin/tazobactam, ceftazidime, tigecycline, and meropenem [2].

The presence of a novel beta-lactamase gene in B. hinzii makes it less susceptible to amoxicillin [3]. In this case, amoxicillin/clavulanate was prescribed for outpatient use. However, the choice of antimicrobial drugs and treatment duration have not been standardized [4].
The Bordetella species can be subdivided into classical and non classical subspecies. The classical subspecies include Bordetella bronchiseptica, Bordetella pertussis, and Bordetella parapertussis [3]. The nonclassical species include Bordetella hinzii, among many others [4]. Classical bordetellae cause disease of the respiratory tract of their natural hosts, whereas nonclassical species may also cause wound infections and bacteremia [4]. Bordetella hinzii is known to cause respiratory disease in poultry and rodents [4]. It has been associated with infections in immunocompromised humans, including bacteremia, septicemia, respiratory disease, and chronic cholangitis [4].
In the United States as of November 2021, there have been 18 reported cases of B. hinzii primarily in patients with cystic fibrosis, HIV/AIDS, and those undergoing immunosuppressant therapy [3]. Humans may become infected by aerosols from the avian reservoirs and may develop pulmonary infection long after exposure [4]. Survival in the digestive tract is another specificity of B. hinzii among the Bordetella species [4]. Studies have shown positive culture results from rectal swab samples of those infected [4]. Thus, this pathogen is likely to be transmitted by the oral route, possibly after ingestion of contaminated poultry products or swallowing of respiratory secretions [4]. Recent studies have shown that soil may also serve as an environmental niche for this pathogen [5].
Summary
Bordetella hinzii is an uncommon cause of pulmonary infections in immunocompetent patients. The infection does not prefer a particular location of the lungs. Its mode of transmission is through droplets or ingestion. It is primarily a zoonotic infection, most commonly caused by rodent and/or avian exposure. Lung infection has not been reported in healthy individuals such as the patient in this case report.
References
- Donato GM, Hsia HLJ, Green CS, Hewlett EL. Adenylate Cyclase Toxin (ACT) from Bordetella hinzii: characterization and differences from ACT of Bordetella pertussis. J Bacteriol. 2005; 187: 7579-7588.
- B hinzii Pneumonia and Bacteremia in a SARS-CoV-2 Patient. Medscape. Accessed August 7, 2022. https://www.medscape.com/viewarticle/961650
- Gregory S, Gregory IS, Fleckenstein J. Three Cases of Bordetella hinzii, United States. Published online 2021: 7.
- Fabre A, Dupin C, Bénézit F, et al. Opportunistic Pulmonary Bordetella hinzii Infection after Avian Exposure - 2015; 21: Emerging Infectious Diseases journal - CDC.
- Hamidou Soumana I, Linz B, Harvill ET. Environmental Origin of the Genus Bordetella. Front Microbiol. 2017; 8: 28.