
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Orthopedic surgery case load and regional anesthesia
practice trend at a tertiary care hospital during first
wave of covid-19 pandemic
Azhar Rehman1*; Kapeel Dev2; Rizwan Haroon Rashid1; Faisal Shamim1
1Aga Khan University Karachi, Pakistan.
2The Kidney Centre Karachi, Pakistan.
*Corresponding Author : Azhar Rehman
Aga Khan University Karachi, Pakistan.
Phone: 03002260187;
Email: azhar.rehman@aku.edu
Received : Aug 29, 2022
Accepted : Sep 19, 2022
Published : Sep 26, 2022
Archived : www.jcimcr.org
Copyright : © Rehman A (2022).
Abstract
Objective: The aim of our study was to evaluate regional anesthesia practice trend in orthopedic surgeries during first three months of pandemic, April-June 2020 and compared with corresponding duration before it started. Tracheal intubation is considered one of the high-risk aerosols generating procedure and potential to transmit infection 6.6 times higher among those who are directly involved in airway management. The evidence for patient, surgical, institutional, and environmental benefits provided by regional anaesthesia is growing and are greatest when general anaesthesia can be avoided.
Methods: This was a retrospective cohort and included all adult patients, who underwent orthopedic surgical procedures from 1st January 2020 to 30th June 2020, at Aga Khan University Hospital. Procedures done under general anesthesia, regional anesthesia, patients who had central neuraxial and peripheral nerve blocks performed for anesthesia and/or analgesia were included.
Results: We found a marginal increase in ultrasound guided nerve blocks placed solely for anaesthesia purpose 43% (n=10) during covid as compare to pre covid 17% (n=7) but overall regional anesthesia practice did not increase during COVID and is not coherent with all the international guidelines that are recommending use of regional anaesthesia techniques as much as possible for better patients and physicians’ outcome and safety.
Conclusion and recommendation: Still, we are way behind when we compare peripheral nerve block practices from the institutes of developed countries. For better patients’ outcome institutions across the country, where the facility of peripheral nerve block is available and anesthetists are well trained, should use regional anesthesia/analgesia techniques as much as they can during the COVID pandemic as per evidence-based recommendations for patients and health care providers safety.
Keywords: Orthopedic procedures; Regional anesthesia; Covid-19.
Citation: Rehman A, Dev K, Rashid RH, Shamim F, et al. Orthopedic surgery case load and regional anesthesia practice trend at a tertiary care hospital during first wave of covid-19 pandemic. J Clin Images Med Case Rep. 2022; 3(9): 2072.
Introduction
Coronavirus Disease 19 (COVID-19) has presented challenges to healthcare systems around the world and will continue to do so for months and perhaps years. This disease has wide spectrum of presentation ranging from asymptomatic to severe form and associated with high risk of infection and transmission. Health care workers (HCWs) are at increased risk of contracting corona virus comprises 20-30% of total infected patients with COVID-19 [1].
General Anaesthesia (GA) involve Aerosol Generating Procedure (AGPs) and upholds the greatest risk of transmission infection [2]. A systematic review assessing infection risks to HCWs ranked AGPs in descending order of risk as tracheal intubation, tracheostomy or emergency Front-Of-Neck airway (FONA), Non-Invasive Ventilation (NIV) and mask ventilation [3]. Risk of infection is 6.6 times higher among those who are directly involved in intubation technique [4]. Tracheal intubation for a corona positive patient should be ideally performed in a negative pressure room which may not be available in all places or situations [5].
Most anaesthesia societies published guidelines on employing Regional Anaesthesia (RA) techniques for patients with COVID-19. These guidelines encourage anaesthetist to perform nerve blocks whenever possible to avoid risk of transmission [4-6]. It offers many obvious solutions to the particular problems posed by these patients and patient will receive safe successful anaesthesia with superior analgesia and decrease postoperative surgical complications [7]. Beneficial effects of RA in orthopedics surgeries on various outcomes areextended in patients with COVID-19 disease for particular individuals, demographics and resource [8,9]. Stuart Wade et al noted considerable change in anaesthesia practice toward RA as primary mode of anaesthesia for procedures which were routinely done under general anaesthesia before COVID-19 pandemic [10]. The aim of our study was to evaluate regional anaesthesia practice trendin orthopedic surgeries during the first three months of COVID-19 pandemic.
Methods
Institutional approval was taken from ethical review committee (2020-5493-13977) to undertake this service evaluation. This retrospective cohort included all adult patients underwent orthopedic surgical procedures at Aga Khan University Hospital. The procedures done under general anaesthesia, regional anaesthesia and monitored anaesthesia care were included. All patients have gone through nasal swab for PCR testing as per institutional policy.
A snapshot search from operating room database was conducted for all orthopedics surgeries done in equal duration of pre COVID and COVID pandemic days. The total number of days from 1st April to 30th June 2020 termed as ‘COVID duration’. The corresponding number of days from 1st January to 31st March 2020 termed as ‘pre COVID duration’. File notes, anesthetic charts and peripheral nerve block form of all patients having regional anaesthesia in the form of central and peripheral nerve blocks within study timeline were reviewed. The type of block, purpose (anaesthesia or analgesia), mode of approach (landmark, peripheral nerve stimulator and or ultrasound), nerve block complications including failure and conversion to GA and type of sedation (if used) were noted. Dual entries were removed associated with inadequate documentation. The data was collected on a specially designed form and entered into SPSS 20.0. Mean and standard deviation are computed of age while frequency and percentage were measured for gender, surgical procedure, peripheral nerve block, intraoperative co- analgesia, post-op pain medications. To determine any statistical significance between the pre COVID and COVID, a Z-test for comparing two proportions was usedat a p-value ≤5% level of significance.
Results
A total of 282 urgent or emergent orthopedic cases performed in operating rooms over first three months of pandemic. During the corresponding period of previous three months, 597 procedures were done.
Table 1: Anaesthesia details in pre COVID and COVID time.
| Anaesthetic technique | Pre COVID (1st January to 31st March 2020 | COVID (1st April to 30th June 2020) | p-value |
|---|---|---|---|
| General Anaesthesia | 553 (92.6%) | 233 (90%) | 0.222 |
| Spinal Anaesthesia | 44 (7.4%) | 26 (10%) | 0.703 |
| Peripheral Nerve Blocks Upper Limb Lower Limb |
41 (64.06%) 17 (41.6%) 24 (58.53%) |
23 (35.94%) 12 (52.17%) 11 (47.82%) |
0.030 0.575 0.555 |
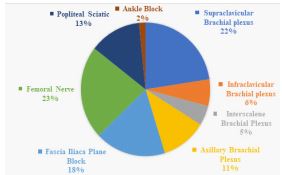
Table 1 shows type of anaesthesia used in these cases during pre COVID and COVID total six months duration. Regional anaesthesia including central and peripheral nerve blocks were performed in 49 patients during three months duration after start of pandemic, while 85 patients received nerve block in pre COVID three months duration. All the peripheral nerve blocksduring pandemic period were performed in operating rooms mainly by consultant anaesthesiologist 39 (80%) and senior residents 10 (20%). The patients aged between 10 to 82 years with mean (standard deviation) 44.5 (20.2). There were 23 (47%) females and 26 (53%) males. All peripheral nerve blocks were performed under ultrasound guidance with aseptic technique with no failed block. The indications for Ultrasound Guided Regional Anaesthesia (USGRA) techniques have been summarized in (Figure 1).
Nerve blocks that were the sole anaesthetic technique for a surgical procedureis termed anaesthesia indication and those were more performed during COVID as compare to pre COVID era (43% n= 10 vs 17% n=7). Blocks that were placed only for pain management categorized as analgesia indication, which were significantly higher in pre COVID time (83% n=34 vs 57% n=13). Resultdoes not show over all any statistically significant difference in the placement of nerve blocks during pre COVID and COVID. Types of different neve blocks illustrated in (Figure 2).
Some patients received more than one nerve block and most frequent were femoral and sciatic block for lower limb surgeries. Nerve blocks were performed for surgical procedures such as, open reduction and internal fixation of radius, ulna, humerus, incision and drainage of hand abscess, shoulder arthroscopy, release of carpal tunnel, total hip replacement, dynamic hip screw placement, intramedullary nailing of femur and tibia.

Discussion
In this single centered study, we do not find any increase in regional anaesthesia practice during the first three months of COVID although we have observed a slight increase in number of ultrasound guided nerve blocks employed solely as anaesthetic technique for surgical procedures but it was statistically insignificant. A number of studies have been published during COVID-19 pandemic regarding peripheral nerve blocks practice [1-3]. Almost all the studies have recommended regional anesthesia [11,12] whenever possible because general anesthesia is associated with aerosol generation hence putting the patient and healthcare providers at risk of getting infected. In another study [6] it was identified that major reason for not doing peripheral nerve blocks is lack of expertise in performing blocks which needs training followed by learning curve to become skillful, but in our set up almost one third of the attendings are comfortable in doing the nerve blocks.
The first three months of COVID have seen the greatest number of coronavirus cases on the rise in Pakistan and a strict lock down had been imposed to reduce the spread of disease. This resulted in postponement of all elective surgical procedures at in our institute. In Orthopedic specialty, trauma and fracture cases were continued coming to hospital. The life-threatening emergent surgeries were performed in specifically dedicated negative pressure operating room with a minimum of 12 air changes per hour.
A joint statement on practice recommendations have been published on peripheral nerve blocks and neuraxial anesthesia during this pandemic of covid-19 by the European Society of Regional Anesthesia, American Society of Anesthesiology [13] and Pain Therapy and American Society of Regional Anesthesia and Pain Medicine in whichthey explained different practical perspectives with regard to use of RA in COVID-19 patients and indeed owing of these recommendations will not only help anesthesiologists to protect themselves from further exposure to coronavirus but also acceptance of this new management planwill help improving patients’ safety and perioperative care [14].
Conclusion
Regional anesthesia is a very useful management technique of anaesthesiologist while managing the patients coming for emergency and elective procedures affected with COVID. Regional anaesthesia should be well planned and executed with exactitude to for the best possible result in COVID-19 patients [15] and this will change outcome benefit not only for the patients but also benefit the team managing perioperatively. There is also need to do an audit to find out the reason for decrease number of peripheral nerve blocks performed during COVID, although this is the safest technique not only for patients but also for healthcare providers.
Conflict of interest: None.
Funding: None.
References
- Shelly L Burrer, Marie A de Perio, Michelle M Hughes, David T Kuhar, Sara E Luckhaupt, Clinton J. McDaniel, et al. Characteristics of Health Care Personnel with COVID-19. Morb Mortal Wkly Rep. 2020; 69: 477–481.
- Cook TM, El Boghdadly K, Mc Guire B, Mc Narry AF, Patel A, Higgs A, et al. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetist. Anaesthesia. 2020; 75: 785–799.
- Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol Generating Procedures and Risk of Transmission of Acute Respiratory Infections to Healthcare Workers: A Systematic Review. PLoS ONE. 2012; 7: e35797.
- Uppal V, Sondekoppam RV, Landau R, El-Boghdadly K, Narouze S, et al. Neuraxial anaesthesia and peripheral nerve blocks during the COVID-19 pandemic: A literature review and practice recommendations. Anaesthesia. 2020; 75: 1350-1363.
- Wax RS, Christian MD. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can J Anesth. 2020; 67: 568–576.
- Sondekoppam RV, Lobo CA, Kolli S, Kalagara HKP. Practice Recommendations on Neuraxial Anesthesia and Peripheral Nerve Blocks during the COVID-19 Pandemic. 2020; 1–5.
- Warren J, Sundaram K, Anis H, Kamath AF, Mont MA, Higuera CA, et al. Spinal Anesthesia Is Associated With Decreased Complications After Total Knee and Hip Arthroplasty. J Am Acad Orthop Surg. 2020; 28: e213–e221.
- Singleton MN, Soffin EM. Daring discourse: Are we ready to recommend neuraxial anesthesia and peripheral nerve blocks during the COVID-19 pandemic? A pro-con. Reg Anesth Pain Med. 2020; 0: 1–4.
- Hassan SA, Sheikh FN, Jamal S, Ezeh JK, Akhtar A, et al. Coronavirus (COVID-19): A Review of Clinical Features, Diagnosis, and Treatment. Cureus. 2020; 12.
- Wade S, Nair G, Ayeni HA, Ayeni HA, Pawa A, et al. A Cohort Study of Emergency Surgery Caseload and Regional Anesthesia Provision at a Tertiary UK Hospital During the Initial COVID-19 Pandemic. Cureus. 2020; 12: e8781.
- Cappelleri G, Fanelli A, Ghisi D, Russo G, Giorgi A, Torrano V, et al. The Role of Regional Anesthesia During the SARS-CoV2 Pandemic: Appraisal of Clinical, Pharmacological and Organizational Aspects. Front. Pharmacol. 2021; 12: 574091.
- Karasu D, Kilicarslan N, Ozgunay SE, Gurbuz H. Our anesthesia experiences in COVID-19 positive patients delivering by cesarean section: A retrospective single-center cohort study. J Obstet Gynaecol Res. 2021; 47: 2659-2665.
- https://www.asahq.org/about-asa/newsroom/news-releases/2022/02/asa-and-apsf-joint-statement-on-elective-surgery-procedures-and-anesthesia-for-patients-after-covid-19-infection.
- Altiparmak B, Korkmaz Toker M, Uysal AI, et al. Regional anesthesia in patients with suspected COVID-19 infection. Regional Anesthesia & Pain Medicine. 2021; 46: 91-92.
- Whizar Lugo VM, Iñiguez López KL, Castorena Arellano G. Regional Anesthesia in Times of COVID-19. In: Whizar-Lugo VM, Saucillo-Osuna JR, Castorena Arellano G, editors. Topics in Regional Anesthesia [Internet]. London: Intech Open; 2022 [cited 2022 Aug 29].