
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Primary mediastinal large B-cell lymphoma, difficult differentiation from the epithelial neoplasm
Atsushi Uchiyama*; Hiroshi Hirano; Yoshie Wakatsuki; Erika Yoshida; Ayako Kato; Midori Wakiya; Hiromi Serizawa; Akira Okimura; Yumika Ito; Munehide Nakatsugawa
Department of Diagnostic Pathology, Hachioji Medical Center, Tokyo Medical University, Japan.
*Corresponding Author : Atsushi Uchiyama
Department of Diagnostic Pathology, Hachioji Medical Center, Tokyo Medical University, Japan.
Tel: +81-42-665-5611, Fax: +81-42-665-1796;
Email: auchiyam@tokyo-med.ac.jp
Received : Sep 01, 2022
Accepted : Sep 20, 2022
Published : Sep 27, 2022
Archived : www.jcimcr.org
Copyright : © Uchiyama A (2022).
Abstract
Primary Mediastinal Large B-Cell Lymphoma (PMBL) is a rare neoplasm that arises in the mediastinum, and then forms a mass.
A female in 50s noticed malaise of right upper limb and a firm lump in the right clavicular region. After consulting with a nearby doctor, she was introduced to our medical center. Magnetic resonance imaging showed a giant mass (12 x 7 x 6 cm) in the anterior and superior mediastinum with expansion to the right supraclavicular fossa. Microscopic examinations of a biopsy specimen led to a diagnosis of PMBL. Methotrexate with Adriamycin, Cyclophosphamide, Vincristine, Prednisolone and Bleomycin (MACOP-B) chemotherapy was given as well as rituxan. Although CT scanning show a marked reduction in size, the tumor remained and radiation therapy was added. Two years later, the patient was transferred to our medical center, though died due to cardiac arrest. From the initial symptoms to death was approximately three years. Touch smear cytology results showed tumor cells present in loose aggregates, though some clusters had a tight aggregation, suggesting epithelial cells. The tumor cells showed abundant and clear cytoplasm, with round nuclei containing nucleoli, and numerous lymphoglandular bodies were also seen. Cells of tight in tight aggregates expressed CD20, in immunocytochemical results, and an epithelial neoplasm was ruled out.
Although cytomorphology provides limited information, and we consider that a diagnosis of PMBL can be determined basedon the combination of unique clinical presentation, flow cytometry and/or immunocytochemistry findings.
Keywords: Primary mediastinal B-cell lymphoma; Cytological feature; Immunocytochemistry.
Abbreviation: PMBL: Primary Mediastinal Large B-Cell Lymphoma; FCM: Flow Cytometry; DLBCL: Diffuse Large Cell B Cell Lymphoma; Nhls: Non-Hodgkin Lymphomas.
Citation: Uchiyama A, Hirano H, Wakatsuki Y, Yoshida E, Kato A, et al. Primary mediastinal large B-cell lymphoma, difficult differentiation from the epithelial neoplasm. J Clin Images Med Case Rep. 2022; 3(9): 2074.
Introduction
Primary Mediastinal Large B-Cell Lymphoma (PMBL) is a rare neoplasm that arises in the mediastinum and forms a mass, with affected patients, accounting for approximately 2-3% of Non-Hodgkin Lymphoma (NHL) cases [1]. Reported here is a patient diagnosed with.
We experienced PMBL diagnosed by biopsy specimen obtained from the mediastinal tumor, and disclosed the cytological features of PMBL obtained from touch cytology. We try utilities of diagnosis of PMBL by aspiration cytology methods.
Case report
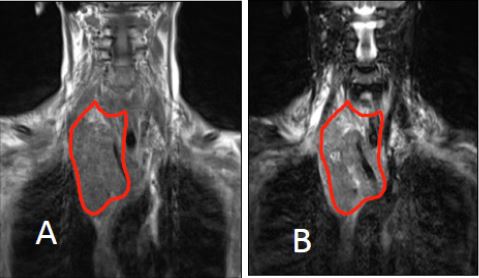
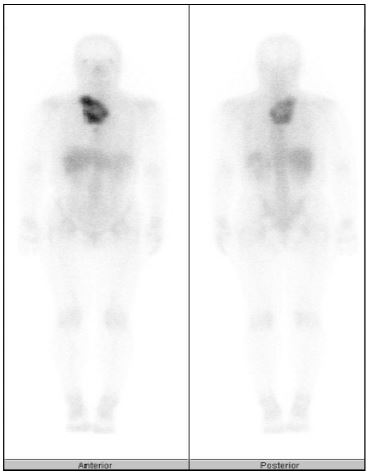
A female in 50s noticed malaise of right upper limb and a firm lump in right clavicular region. She consulted with a nearby doctor, and was introduced to our medical center. Physical examinations showed no obvious abnormal findings. Tumor markers showed aIL-2 receptor level of 434.0 U/ml (normal range 190-650 U/ml). Magnetic Resonance Imaging (MRI) revealed a giant mass in the anterior and superior mediastinum sized 12 x 7 x 6 cm sized, with expansion into the right supraclavicular fossa. T1-weighted MRI showed a low-intensity signal, which was the same intensitysignalseen in T2-weighted MRI images. Vessels revealed a filling defect, and the tumor was considered to be a soft mass (Figures 1A,1B). Accumulation in the giant mass between the anterior and superiorof the right supraclavicular fossa and anterior mediastinum described above was also shown by Gallium scintigraphy (Figure 2). A biopsy specimen was obtained and microscopy examinations led to a diagnosis of PMBL.
Solumedrol (1000 mg) was administered with the aim of improvement of superior vena cava syndrome and pleural effusion, after which the patient received Methotrexate, Adriamycin, Cyclophosphamide, Vincristine, Prednisolone And Bleomycin (MACOP-B) therapy as well as Rituxan. Although CT scanning showed a marked reduction in size thereafter, the tumor remained and radiation therapy was added.
Two years later, the patient was transferred to our medical center, though died. An autopsy was not performed, and the cause of death associated with PMBL is unknown. The period of time form initial symptoms to death was approximately three years.
Pathological findings
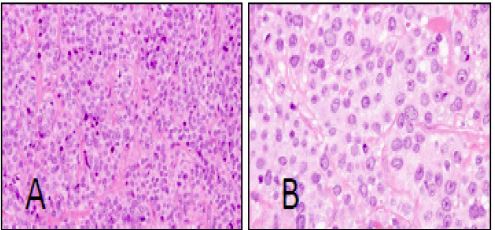
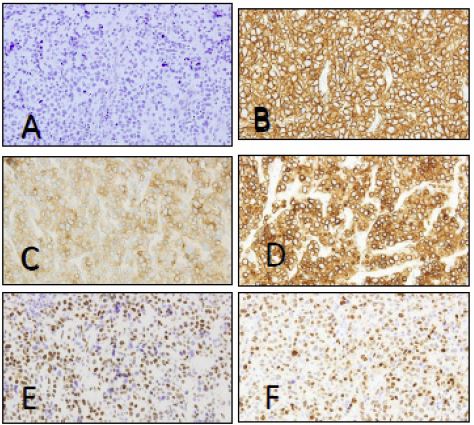
The growth pattern is diffuse and it development is associated with compartmentalizing alveolar fibrosis (Figures 3A,3B). In the present case, the neoplastic cells were medium to large size, with abundant pale cytoplasm, and relatively round or ovoid nuclei (Figure 3A,3B). In addition, cytoplasm showed a ground-grass appearance (Figure 3B). Immunohistochemical findings denied epithelial markers such ascytokeratin (CK)-AE1/AE3 (Figure 4A) in neoplastic cells, though they expressed B-cell lineage antigens such as CD20 (Figure 4B) and CD79a (Figure 4C). In addition, CD30 (Figure 4D), bcl-2 and bcl-6 (Figure 4E), and CD23, and MUM-1 (Figure 4F), as well as CD45 and TRAF-1 were positive. On the other hand, neoplastic cells did not express T-cell lineage antigens such as CD3, CD4, or CD8. In additions, no expression of CD10, CD15, CD56, CD21, cyclin D1, EMA, or CD138 was noted.
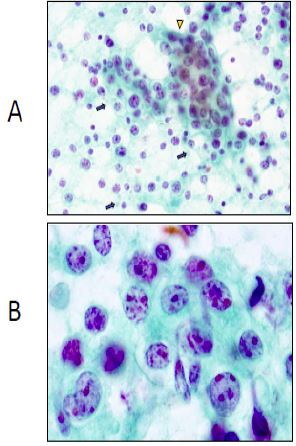
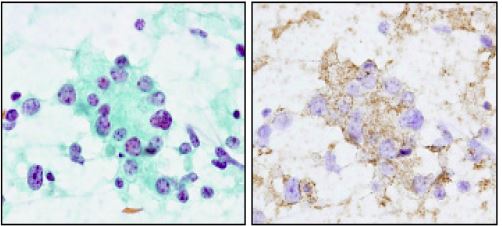
Touch smear cytomorphological results of neoplastic cells showed the presence of tumor cells in loose aggregates, though some clusters had a tight aggregate, which suggested epithelial cells, while Numerous lymphoglandular body were seen (Figure 5A). Furthermore, tumor cells had abundant and clear cytoplasm, and round nuclei with some nucleoli (Figures 5A,5B. Epithelial connectivity was noted, thus an immunocytochemical examination was performed with only CD20 antigen, which revealed CD20 expression in the neoplastic cells (Figure 6).
Discussion
The WHO classifies PMBL, as a rare subtype of Diffuse Large Cell B Cell Lymphoma (DLBCL), which is seen in approximately 2-3% of NHL case [1]. These tumors arise in the thymus and usually affect young adults, predominantly females, and displays a unique combination of clinical, histological, immunologic, and cytogenetic features. Clinically, a PMBL is commonly presented as a rapidly enlarging mass in the anterior and superior mediastinum that infiltrates surrounding structures and causes symptoms of compression. Superior vena cava syndrome is presented approximately 30% of the affected cases. The present patient had a similar clinical course.
In histological findings, a PMBL shows varying cell and nuclear sizes, and a clear cytoplasm, with occasional compartmentalizing fibrosis or sclerosis [2,3]. Histological features of the present case were consistent with PMBL are similar to those of DLBCL, as PMBL is a subtype. Those tumors also expresses the characteristic B-lineage surface markers, such as CD20 and CD79a. On the other hand, expressions of surface and cytoplasmic immunoglobulin as well as CD21 are often absent [2], while CD30 expression is weak and in homogenous [1]. The present immunohistochemical results are consistent with those of previously reported PMBL cases [2].
Using cytomorphological findings, PMBL can be classified into three categories (I-III) [2]. In the category I type, cells are two to three times as larger than lymphocytes and resemble marginal zone B cells. The cytoplasm is clear with faint staining and forms a narrow rim with a distinct outer border, while nuclei are medium-sized and vesicular, with small nucleoli. In category II (most cases), the malignant cells are five to six times larger than normal lymphocytes and comparable to large monocytoid B cells. The cytoplasm is abundant and pale, and nuclei are vesicular with nucleoli present. Category III, cases are enormous, 15-20 times the size of normal lymphocytes and have no counterpart in benign lymphoid tissue. Cytoplasm is abundant and clear with variable nuclei. Hydropic change of the cytoplasm, initially termed clear cell morphology, is most prominent in formalin-fixed tissue sample [2]. Cytomorphology findings for the present case seems to partially indicate category II, with immunocytological results considered to be consistent with those of DLBCL. Unfortunately, we were not able to perform immunocytological analysis except for CD20. Histological features of PMBL are known to be similar to those of epithelial neoplasm, thus animmunochemistry examination is important for excluding that in a malignant form. The presents confirm that findings indicating CD20 expression are important.
Dong et al reported cytology and Flow Cytometry (FCM) results that provided information to correctly diagnose and subclassify 77% of lymphomas based on the REAL/WHO classification, with subsequent good tissue findings also presented [4]. In a similar report presented by Mourad et al., cytologic diagnostic accuracy was found to be best for small lymphocytic lymphoma, lymphoplasmacytic lymphoma, Burkitt’s lymphoma, mantle cell lymphoma, and plasmacytoma (100%), while it was intermediate for diffuse large B-cell lymphoma (62%), and poor for marginal-zone lymphoma (33%). In addition, Hoda et al. reported a case of PMBL for which a diagnosis could be obtained by fine-needle aspiration of the tumor with immunocytochemical typing by FCM [6].
Cytomorphology provides only information and diagnosis of PBML with findings from that alone is difficult, we consider that the most reliable PMBL diagnosis is from combination of a unique clinical presentations, along with FCM and/or immunocytochemistry findings.
References
- Gaulard P, Kovrigina AM, Harris NL, Jaffe ES, Pileri SA, Moller P, et al. Primary mediastinal (thymic) large B-cell lymphoma. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. WHO Classification of tumours of Haematopoietic and Lymphoid Tissues. International Agency for Research on Cancer. Lyon, France, 2017.
- PaulliM, Strater J, Gianelli U, Rousset MT, Gambacorta M, et al. Mediastinal B-cell lymphoma: A study of its histomorphologic spectrum based on 109 cases. Hum Pathol. 1999; 30: 178-187.
- Besien K, Kelta M, Bahaguna P. Primary mediastinal B-cell lymphoma: A review of pathology and management. J Clin Oncol. 2001; 19: 855-864.
- Dong HY, Harris NL, Preffer FI, Pitman MB. Fine-needle aspiration biopsy in the diagnosis and classification of primary and recurrent lymphoma: A retrospective analysis of the utility of cytomorphology and flow cytometry. Mod Pathol. 2001; 14: 472-481.
- Mourad WA, Tulbah A, Shoukri M, Dayel FA, Akhtar M, Ali MA, et al. Primary diagnosis and REAL/WHO classification of non-Hodgkin’s lymphoma by fine-needle aspiration: Cytomorphologic and immunophenotypic approach. Diagn Cytopathol. 2003; 28: 191-195.
- Hoda RS, Picklesimer L, Green KM, Self S. Fine-needle aspiration of a primary mediastinal large B-cell lymphoma: A case report with cytologic, histologic, and flow cytometric considerations. Diagn Cytopathol. 2005; 32: 370-373.