
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Spontaneous pregnancy after unprotected pelvic radiotherapy for hodgkin lymphoma: A case report
Feyza Yaşar Daşgın1*; İpek Pınar Aral1,2; Gonca Altınışık İnan1,2; Tarık Kargıoğlu1; Yılmaz Tezcan1,2
1Ankara City Hospital, Radiation Oncology Clinic, Ankara, Turkey.
2Ankara Yıldırım Beyazıt University, Radiation Oncology Clinic, Ankara, Turkey.
*Corresponding Author : Feyza Yaşar Daşgın
Ankara City Hospital, Radiation Oncology Clinic, Ankara, Turkey.
Tel: +90 5058937861;
Email: feyzaysr@gmail.com
Received : Aug 30, 2022
Accepted : Sep 20, 2022
Published : Sep 27, 2022
Archived : www.jcimcr.org
Copyright : © Daşgın FY (2022).
Abstract
Hodgkin lymphoma is a lymphoproliferative malignancy originating from B cells of the immune system and is most commonly seen in adolescents and young adults. Hodgkin Lymphoma treatment is multimodal and includes chemotherapy, radiotherapy and stem cell transplantation. Survival in Hodgkin Lymphoma has increased due to current effective treatments, and late side effects have become more important. Late toxicities seen in Hodgkin Lymphoma survivors are as follows, in order of frequency: Cardiovascular diseases, secondary cancers, endocrine, metabolic, neurological sequelae, and infertility. There are many approaches to maintaining fertility in Hodgkin Lymphoma survivors. Recently, fertility preservation in Hodgkin Lymphoma survivors is one of the most important issues in the long-term management of patients. In this article, we present a 25-year-old female patient with Hodgkin Lymphoma who refused the fertility-preserving approach, had a spontaneous pregnancy in the second month after the completion of her treatment, and had a healthy baby at term. To our knowledge, this is the 6th case in the literature, who underwent pelvic Radiotherapy without preserving fertility and subsequently conceived spontaneously and had a healthy baby at term. As a result; in cases of pelvic Radiotherapy applied without ovarian protection, spontaneous pregnancy and healthy delivery can be observed even after a short time, despite taking the dose that is toxic for ovarian sterilization.
Keywords: Hodgkin lymphoma; Fertility; Spontaneous pregnancy.
Citation: MDaşgın FY, Aral İP, İnan GA, Kargıoğlu T, Tezcan Y. Spontaneous pregnancy after unprotected pelvic radiotherapy for hodgkin lymphoma: A case report. J Clin Images Med Case Rep. 2022; 3(9): 2075.
Introduction
According to GLOBOCAN data, 19 million people were diagnosed with cancer in 2020 and 83,000 of them were Hodgkin Lymphoma (HL) [1]. The mortality/incidence ratio of HL is 23.376/83.087 for 2020 [2]. According to the SEER data of the American Cancer Society between 2011 and 2017, the 5-year relative overall survival is 88% [3]. The incidence in developed countries is bimodal with respect to age distribution, and there is an initial peak in young adults at approximately age 25 years, and a second peak occurring at ages 60 to 70 years [4]. The most common clinical presentation of HL is nontender lymphadenopathy, mostly in the cervical nodal chain, occurring in approximately 70% of cases. Axillary or inguinal adenopathy are less frequently reported, found in approximately 15% and 10% of patients, respectively [5]. With modern treatment strategies, remission is achieved in 80-90% of patients with HL and can be considered as a cure [6]. Due to the increasing number of lymphoma survivors, several long-term toxicities of diverse treatment modalities have come to the attention of hematologists and other physicians who take care of lymphoma survivors, making the follow-up multidisciplinary [7,8]. The main categories of long-term toxicity in populations of HL patients treated in adulthood are, in order of frequency, cardiovascular diseases, secondary cancers, endocrine, metabolic, neurological sequelae and infertility [9,10].
Primary therapy of HL typically includes combined-modality therapy (combining chemotherapy (CT) and RT). Therapeutic methods that are used in antineoplastic treatment cause fertility impairment or sterilization due to permanent damage to reproductive cells. Because of gonadotoxic chemotherapy and radiotherapy, these patients are at higher risk for Premature Ovarian Failure (POF) or hypergonadotropic hypogonadism than people who do not receive these treatments [11].
Gonadal toxicity following cancer therapy mainly involves a decline in the endocrine functions that sustain the production of sex hormones (testosterone and estrogens) and germ cells (ova and sperm) [12,13]. The testis and ovaries are the most radiosensitive tissues. Permanent ovarian impairment can be detected after 5–6 Gy, with higher radiosensitivity related to older patients [12,14]. Pelvic radiotherapy results in ovarian injury and diminished follicle reserve; the extent of damage is largely based on the patient’s age, treatment dose, and the irradiation field. The location of the radiation field impacts the degree of ovarian damage with total body irradiation observed to result in ovarian failure in 90% of patients in long term follow-up. After abdominal radiation, ovarian failure rates may be as high as 97% [14,15]. Spontaneous pregnancy is rarely seen in patients due to high ovarian failure. Almost all of the patients who want to get pregnant in the long term after the cure can become pregnant with medical support. After pregnancy, there are many risks such as premature birth, low birth weight, uterine rupture in patients during pregnancy. Patients with a history of pelvic and abdominal RT should be considered high-risk during their pregnancy.
In this case report, a patient with a diagnosis of Hodgkin lymphoma who received pelvic radiotherapy without ovarian protection and who spontaneously became pregnant in the 5th month after RT and had a term and healthy baby will be shared. This case report is interesting in that ovarian preservation is not performed, the patient conceived spontaneously shortly after RT and gives birth to a healthy baby. To our knowledge, this is the 6th case in the literature, who underwent pelvic RT without preserving fertility and subsequently conceived spontaneously and had a healthy baby at term.
Review of literature
We searched the Pub Med database (National Library of Medicine, http:// www. ncbi.nlm.nih.gov) between january 1984 to June 2022, using the following search: pelvic radiotherapy, spontaneous pregnancy, case report. Case reports involving ovarian preservation or any fertility-preserving approach were excluded. Cases who had definite data on radiation dose and fractionation, did not apply any fertility-preserving approach, and spontaneously conceived and delivered healthy babies after pelvic RT were included in the literature review. As a result of this research; 5 articles submitted to the literature and 5 cases (not included our case) were identified (Table 1).
Table 1: Cases who had definite data on radiation dose and fractionation, did not apply any fertility-preserving approach, and spontaneously conceived and delivered healthy babies after pelvic RT were explained in the table. The primary diseases of the patients, the radiotherapy doses and fraction numbers applied, the doses taken by the ovaries and the uterus, the age of the patients during Radiotherapy, the age of the patients at the time of pregnancy, the birth week of the babies and the last health status of the babies are explained in the table.
Case report
A 25-year-old woman who hasn’t had any disease before was admitted to the hospital with a complaint of swelling in the axilla in March 2020. Biopsy was performed from the lymph node in the axilla and the result was Hodgkin lymphoma, nodular sclerosis subtype. According to FDG-PET at the time of diagnosis, there were conglomerated lymphadenopathies in both jugular chains, in both supraclavicular and infraclavicular areas, and in both axillae in the neck. There were also mediastinal, left hilar, and left parasternal lymph nodes showing higher FDG uptake. In addition, there is diffuse higher FDG uptake in the bone marrow and spleen. The disease was considered stage IV at the time of diagnosis.
The AVD (Adriamycin, Vinblastine, Dacarbazine) protocol was applied to the patient. The patient received 5 cycles of AVD regimen between 19 March 2020 and 2 October 2020. According to FDG-PET after chemotherapy, there is a lower level of FDG uptake in the neck at right level 2 and in the bilateral axillary region compared to the time of diagnosis. There is involvement of bilateral inguinal lymph nodes (Figure 1).
The patient was evaluated with a Deauville score of 5 and it was decided to give adjuvant radiotherapy. Before radiotherapy was planned, the patient was informed about the risks of infertilization and was referred to the relevant branch for fertilization preservation. However, the patient declared that she did not want to apply these fertility preservation methods and accepted radiotherapy despite all the risks. She had 2 children, a girl and a boy, before the HL diagnosis.
Radiotherapy treatment was planned between 24 February, 2021 and 25 March, 2021 in Ankara City Hospital radiation oncology clinic. A total of 36 Gy radiotherapy was applied to the patient’s bilateral neck level 2,3,4 and upper mediastinum, bilateral axilla, and bilateral inguinal lymph node regions from a daily 180 cGy dose schedule in 20 fractions (Figure 2, Figure 3).
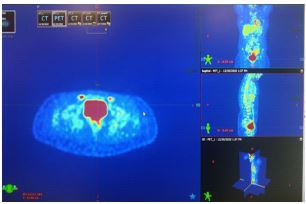
Table 1: Review of the literature.
| Case | Primary | RT doses/fraksiyon number | Ovary/uterus doses | Age of RT | Age of pregnancy | Baby born week | Baby last status |
|---|---|---|---|---|---|---|---|
| 1 [44] | Giant cell tumors- pelvic L5/S1 | 50.4 Gy/ 5.5 w 2D | ovaries doses > 4Gy | 15y | 24y | 31w, 3d | The baby's birth weight was 1.38 kg and it was healthy and discharged at 12 weeks-of-life, and has been well to date. |
| 2 [41] | Anal Cancer | 50 Gy/25 frx | Left ovary Dmax: 29.59Gy, mean dose: 4.21Gy Right ovary Dmax: 31.58Gy, mean dose: 31.12Gy |
25y | 25y (She got pregnant in the first year after RT. Hormone replacement therapy was administered. Pregnancy 3 months after stopping HRT) | 39 w | Healthy baby |
| 3 [45] | Anal Cancer | 50.4 Gy/ (30.6 Gy/17 frx [phase 1], 19.8 Gy/11 frx [phase 2]) |
Left ovary mean dose: 1Gy, Right ovary mean dose:31.5 Gy, The uterus mean dose was 34.5 Gy |
26y | 31y | preterm | Healthy |
| 4 [42] | Rectal cancer Mucosa-associated lymphoid tissue lymphomas | 30.6 Gy / 17 frx | The uterus mean dose was 22.5 Gy The ovary mean dose was 16.6 Gy, |
28y | 29y | NS | Healthy |
| 5 [25] | Rhabdomyosarcoma | 45 Gy | 6y | 1st: the patient aged 22 presented with a spontaneous miscarriage 2st: The patient aged 23 At 21 W G, she presented with threatened late miscarriage and gave birth to a live girl who would die. the patient gave birth to a live 402 g girl who would die at 1h17 of life. 3th:At 18 W G, emergency cervical cerclage was performed. At 35 W G the ultrasound found severe intrauterine growth retardation. Cesarean section was performed allowing the birth of a girl in good health status. |
35 w | Healthy | |
| 6 (current case) | Hodgkin Lymphoma | 36 Gy / 20 frx | Right ovary Dmax: 9.56 Gy,
mean dose: 2.08 Gy; Left ovary Dmax: 6.33 Gy, mean dose: 2.15 Gy |
25y | 25y | Healthy |
The ovarian doses received by the patient due to RT are as follows; right ovarian Dmax: 9.56 Gy, mean dose: 2.08 Gy; Left ovarian Dmax: 6.33 Gy, mean dose: 2.15 Gy (Figure 4).
The patient has followed up after treatment. In the 2nd month follow-up of the patient after radiotherapy, it was observed that all lymph nodes that were arrested in the previous imaging regressed and there were no new lesions.
In the follow-up of the patient, she had a spontaneous pregnancy in the 2nd month after the end of the radiotherapy. A 38-week, 3 kg, C/S baby boy was born at the 11th month post-RT. The baby has no health problems other than ASD, which was noticed after birth in the baby’s heart. In the follow-up of the baby, the ASD in his heart closed spontaneously. Our patient’s disease is in remission and her baby is 6 months-3 weeks old.


Figure C shows the DVH (dose-volume histogram) of the radiotherapy plan. Blue color is PTV and the yellow color is the left and right ovary.
Figure D shows the dose statistics table. Organs at risk doses are shown.

Discussion
There is limited data in the literature on spontaneous pregnancy of patients who received pelvic RT and did not apply fertility preservation approaches. In this case report, it was presented to the literature that a patient who did not accept the fertility-preserving approach and underwent pelvic RT was spontaneously pregnant shortly after RT and gave birth to a healthy baby at term. Both spontaneous pregnancy and delivery of a healthy baby at term are important in terms of showing that the ovarian and uterine functions of the patient continue despite RT.
RT has been one of the main treatments applied to oncological patients for nearly 100 years. The main goal of RT is to protect the surrounding critical organs as much as possible while giving effective doses to the target volume. The doses taken by the critical organs in the environment and the side effects to be seen as a result are predicted by a hundred years of experience. The risk of this side effect has been presented with guidelines [16,17]. The ovaries are highly radiosensitive organs and are affected by very low doses. The LD50 dose for the ovaries is 2 Gy [18]. Doses of 2 Gy or less applied to the ovaries can cause 50% loss in immature oocytes; At a dose of 4 Gy, it causes infertility in ⅓ of young women and in all women over the age of 40 [19-22]. In our patient, right ovary Dmax: 9.56 Gy Left ovary Dmax: 6.33 Gy dose. Although both ovaries were over 4 Gy, pregnancy soon followed.
The presence of a healthy oocyte originating from a functioning ovary is required for fertility. For a healthy pregnancy, it is necessary to have a functioning and healthy uterus. Abdominal and pelvic irradiation and side effects such as oocyte loss and uterine atrophy make it difficult to establish a healthy fertility and pregnancy [23]. The following side effects may occur after pelvic RT depending on the doses received by the uterus and ovaries: infertility, early menopause, low birth weight, preterm birth, perinatal baby loss, delivery of small-for-gestational-age infants, uterine rupture, preeclampsia, and abnormal placentation. Uterine problems cause problems especially related to the continuation of pregnancy. Preterm and low birth weight as a result of uterine radiation damage have been reported frequently in the literature [24-27]. It has been reported that a significantly higher rate of low birth weight and preterm delivery was observed in patients who received pelvic RT due to childhood tumors [28]. Birth weight < 10 percentile for gestational age was found to be significantly higher in women with uterine dose of 5 Gy and above [29]. Women treated with abdomino-pelvic radiation have an increased rate of uterine dysfunction leading to miscarriage, preterm labor, low birth weight, and placental abnormalities [30]. Irradiation doses approaching 14-30 Gy may also cause permanent damage to uterine musculature and vessels, thereby potentially impeding the ability of a survivor to carry a full-term pregnancy [11].
Every year, approximately 1 million male and female adult individuals of childbearing age are diagnosed with cancer, and 80% of these individuals have a long survival expectation. Especially prolonged survival and long-term side effects have become important in oncological patients [31,32]. Before the treatment, the risks are discussed with the patients and fertility-preserving approaches can be applied before the treatment. However, in order to implement fertility preservation, first of all, it is necessary to predict the reproductive potential of the patients after the treatment, taking into account their ovarian reserves, oncological diseases and the treatment to be applied. A number of Assisted Reproduction Technology (ART) approaches such as reproductive cryobiology and translational medicine are currently adopted to preserve and restore fertility in women after their chemotherapy and radiotherapy gonadotoxic regimens [33,34]. To this regard, in order to prevent or reduce the impact of these therapies on fertility, several well established procedures (ovarian suppression with GnRH, oocyte cryopreservation, ovarian cortex cryopreservation for woman and sperm cryopreservation for men) and other ongoing experimental practices (ovar ian cortex cryopreservation, OSCs for women and testicular tissue cryopreservation for men) are widely adopted for young patients before and during anticancer therapy or are under intensive investigation [34]. Ovarian transposition is another possibility to conserve fertility in females. It is a procedure performed in order to transpose an ovary out of the radiation field for the duration of therapy. It was introduced in the 1950s and is applied in the settings of cervical cancer, rectal cancer, Hodgkin and non-Hodgkin lymphoma and childhood sarcoma radiotherapy. The procedure consists of relocating the ovary and part of the Fallopian tube superolaterally as far as possible, most often above the pelvis, at the level L4–L5 [12,19,30]. It is recommended to evaluate the uterine and ovarian functions separately, especially in patients who want a baby after oncological treatments, and try different approaches according to the individual situation of the patient. For example, in a patient with premature ovarian failure, there is a case in the literature in which a healthy pregnancy was obtained with an egg donor after uterine functions were evaluated as normal [27]. There are many options in terms of fertility in oncological patients, but the patients’ access to it, the cost, and the time taken for fertility-preserving approaches before oncological treatment are important. However, according to USA data, only 4-20% of women can access fertility preservation techniques [35,36]. In the current case, fertility-preserving approaches were recommended to our patient. However, the patient did not want it because of its high cost and the concern that it might delay the oncological treatment.
It is a well-known fact that the patient’s age is important in the fertility-RT relationship [19,28,37]. In particular, according to Kroman at all. More than 10,000 women with primary breast cancer who were younger than 45 years at the time of diagnosis; only 371 had a full-term delivery after cancer treatment [38]. The optimal time to attempt conception after completion of cancer treatment is unknown. Many experts recommend waiting at least 2 years after therapy is concluded because it is speculated that, beyond this window, the greatest risk of recurrence has passed [39]. Irradiation dosage and patient age also largely determine the degree of follicular loss and the likelihood of developing premature menopause. In female cancer survivors, the relative risk of developing premature ovarian failure and infertility rates have both been observed to increase with increasing doses of abdominal pelvic radiation. In addition, older patients are more susceptible to radiation-induced damage [33,40]. Due to the young age of our patient, it is thought that there is no problem in ovarian functions due to radiation.
Another important issue is the presence or absence of an optimal time for pregnancy after RT. In the literature review, we noticed that 2 cases (case 2 and case 4) who gave birth to a healthy baby at term became pregnant spontaneously in the first 1 year after RT, similar to our case [41,42]. However, there is not enough data in the literature on the subject.
Contrary to the case we presented to the literature, there are many cases in the literature presenting unsuccessful pregnancies of patients in similar situations. In the article presented by Cigante in 2019, a case with infertility and recurrent abortion after pelvic RT was presented. In this case report, the pregnancy of a patient who underwent CRT at the age of 13 for Ewing sarcoma was terminated by misscariage at the age of 17 weeks after fertility treatment at the age of 28. Afterwards, when she was 30 years old, she became pregnant again after fertility treatment. In her second pregnancy, emergency curettage and hysterectomy were performed as a result of the development of uterine rupture at the 20th week. It was observed that the patient with a left iliac bone localized lesion had uterine rupture in the left horn of the uterus and was 3 cm wide. No macroscopic anomaly was found in the fetus [43]. In the article presented by Wald et al. in 2016, spontaneous twin pregnancy was seen 11 years after the treatment with the diagnosis of rectum cancer and 50 Gy pelvic RT, but the pregnancy was terminated urgently at 28 weeks with preterm premature rupture of membranes [24]. In the article presented by Verhaeghe in 2021, a patient with a diagnosis of rhabdomyosarcoma who received 45 Gy pelvic RT when he was 6 years old, had 3 consecutive spontaneous pregnancies. Although the first two pregnancies were unsuccessful, a healthy baby was born in the third pregnancy despite complications [25]. Pregnancy after pelvic RT is high risk and may be accompanied by many complications. The ovarian and uterine doses, which are the main causes of infertility and complications, should be meticulously noted [26]. There is a lack of data on this subject in the literature, especially since this situation is often overlooked in pediatric patients.
Conclusion
Fertility considerations should be questioned in adult female patients diagnosed with cancer in whom long survival is expected, and fertility-preserving approaches should be explained to the patients before treatment. Infertility and pregnancy complications increase after pelvic RT. Although these patients are defined as high-risk pregnancies, spontaneous pregnancy and healthy baby delivery can be observed, as in the case we presented.
Declarations
Conflict of interest: The authors whose names are listed certify that they have no affiliations with or involvement in anyorganization or entity with any financial interest or non-financial interest inthe subject matter or materials discussed in this manuscript.
Financial disclosure: The authors declared that this study received no financial support.
References
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021; 71: 209-249.
- https://gco.iarc.fr/today/online-analysis-multi-bars?v=2020&mode=cancer&mode_population=countries&population=900&populations=900&key=total&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=55&group_cancer=0&include_nmsc=0&include_nmsc_other=1&type_multiple=%257B%2522inc%2522%253Atrue%252C%2522mort%2522%253Atrue%252C%2522prev%2522%253Afalse%257D&orientation=horizontal&type_sort=0&type_nb_items=%257B%2522top%2522%253Atrue%252C%2522bottom%2522%253Afalse%257D
- https://www.cancer.org/cancer/hodgkin-lymphoma/detection-diagnosis-staging/survival-rates.html
- Andrea K, Ng and Ann S. LaCasce. Hodgkin Lymphoma, etiology and epidemiyology. In: Joel E. Tepper, Robert L. Foote, Jeff M. Michalski editors. GUNDERSON & TEPPER’S CLINICAL RADIATION ONCOLOGY, FIFTH EDITION. Elsevier 1600 John F. Kennedy Blvd. Ste. 1600 Philadelphia, PA 19103-2899.
- Andrea K., Ng and Ann S. LaCasce. Hodgkin Lymphoma, Clinical Manifestations/Patient Evaluation/Staging. In: Joel E. Tepper, Robert L. Foote, Jeff M. Michalski editors. Gunderson & Tepper’s Clinical Radiation Oncology, Fifth Edition. Elsevier 1600 John F. Kennedy Blvd. Ste. 1600 Philadelphia, PA 19103-2899.
- Eichenauer DA, Aleman BMP, André M, Federico M, Hutchings M, Illidge T, et al. ESMO Guidelines Committee. Hodgkin lymphoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018; 29: iv19-iv29.
- Ciavarella S, Minoia C, Quinto AM, Oliva S, Carbonara S, Cormio C, et al. Improving Provision of Care for Long-term Survivors of Lymphoma. Clin. Lymphoma Myeloma Leuk. 2017; 17: e1–e9.
- Minoia C, Bari A, Nassi L, Banzi R, Gerardi C, Lenti V, et al. A. Management of lymphoma survivor patients in Italy: An evaluation by Fondazione Italiana Linfomi. Tumori J. 2021; 107: 91–94.
- Gerardi C, Allocati E, Minoia C, Guarini A, Banzi R, et al. Long-Term Follow-Up of Classical Hodgkin Lymphoma and Diffuse Large B-Cell Lymphoma Survivors: Aims and Methodological Approach for Fondazione Italiana Linfomi Systematic Reviews. Cancers. 2021; 13: 2976.
- Ng AK, van Leeuwen FE. Hodgkin Lymphoma: Late Effects of Treatment and Guidelines for Surveillance. Semin. Hematol. 2016; 53: 209–215.
- Patel B, Rossi B. Preserving fertility in young patients with lymphoma: An overview. Blood Lymphat Cancer. 2015; 5: 1-15. https://doi.org/10.2147/BLCTT.S47236
- Di Molfetta S, Daniele A, Gerardi C, Allocati E, Minoia C, Loseto G, et al. Late Endocrine and Metabolic Sequelae and Long-Term Monitoring of Classical Hodgkin Lymphoma and Diffuse Large B-Cell Lymphoma Survivors: A Systematic Review by the Fondazione Italiana Linfomi. Cancers (Basel). 2022; 10; 14: 1439.
- Silvestris E, Cormio G, Skrypets T, Dellino M, Paradiso AV, Guarini A, et al.. Novel aspects on gonadotoxicity and fertility preservation in lymphoproliferative neoplasms. Crit Rev Oncol Hematol. 2020; 151: 102981.
- Wallace WH, Shalet SM, Crowne EC, Morris Jones PH, Gattamaneni HR. Ovarian failure following abdominal irradiation in childhood: natural history and prognosis. Clin Oncol (R Coll Radiol). 1989; 1: 75-79.
- Wallace WHB, Thomson AB, Saran F, Kelsey TW. Predicting age of ovarian failure after radiation to a field that includes the ovaries. Int J Radiat Oncol Biol Phys. 2005; 62: 738-744.
- Emami B. Tolerance of Normal Tissue to Therapeutic Radiation. Reports of Radiotherapy and Oncology. 2013; 1: 35-48.
- Gerhard SG, Palma DA, Arifin AJ, Louie AV, Li GJ, Al-Shafa F, et al. Organ at Risk Dose Constraints in SABR: A Systematic Review of Active Clinical Trials. Pract Radiat Oncol. 2021; 11: e355-e365.
- Stroud JS, Mutch D, Rader J, Powell M, Thaker PH, Grigsby PW, Effects of cancer treatment on ovarian function. Fertil Steril. 2009; 92: 417-427.
- Gross E, Champetier C, Pointreau Y, Zaccariotto A, Dubergé T, Guerder C, et al. Tolérance à l’irradiation des tissus sains: Les ovaires [Normal tissue tolerance to external beam radiation therapy: ovaries]. Cancer Radiother. 2010; 14: 373-375. French.
- Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF, et al. Accelerated disappearance of ovarian follicles in mid-life: Implications for forecasting menopause. Hum Reprod. 1992; 7: 1342–1346.
- Wallace WH, Thomson AB, Kelsey TW. The radio sensitivity of the human oocyte. Hum Reprod. 2003; 18: 117–121.
- Oncology Rot JCfC. Management of Gonadal Toxicity Resulting from the Treatment of Adult Cancer. 1998. ISBN 1 86016 071 9.
- Oktem O, Kim SS, Selek U, Schatmann G, Urman B, et al. Ovarian and Uterine Functions in Female Survivors of Childhood Cancers. Oncologist. 2018; 23: 214-224.
- Wald K, Easterling T, Swisher EM. Spontaneous Twin Pregnancy After Oophoropexy and Pelvic Radiation for Rectal Cancer. Obstet Gynecol. 2016; 128: 792-794.
- Verhaeghe C, Decanter C, Sudour H, Defachelles AS, Escande A, Grabarz A, et al. Pregnancy after chemoradiotherapy in childhood: Complications and recommendations - about one case. J Gynecol Obstet Hum Reprod. 2021; 50: 101947.
- Sudour H, Chastagner P, Claude L, Desandes E, Klein M, Carrie C, et al. Fertility and pregnancy outcome after abdominal irradiation that included or excluded the pelvis in childhood tumor survivors. Int J Radiat Oncol Biol Phys. 2010; 76: 867-873.
- Lu BJ, Chi MS, Lan YP, Chang YE, Chen CH, Chen CH. Successful live birth after repeated high-dose radiotherapy to the uterus. Reprod Biomed Online. 2021; 42: 774-777.
- Chiarelli AM, Marrett LD, Darlington GA. Pregnancy outcomes in females after treatment for childhood cancer. Epidemiology. 2000; 11: 161–166.
- Green DM, Sklar CA, Boice JD Jr, Mulvihill JJ, Whitton JA, Stovall M, et al. Ovarian failure and reproductive outcomes after childhood cancer treatment: results from the Childhood Cancer Survivor Study. J Clin Oncol. 2009; 27: 2374-2381.
- Wo JY, Viswanathan AN. Impact of radiotherapy on fertility, pregnancy, and neonatal outcomes in female cancer patients. Int J Radiat Oncol Biol Phys. 2009; 73: 1304-1312.
- Griffiths MJ, Winship AL, Hutt KJ. Do cancer therapies damage the uterus and compromise fertility? Hum Reprod Update. 2020; 26: 161-173.
- Gorman JR, Usita PM, Madlensky L, Pierce JP. Young breast cancer survivors: Their perspectives on treatment decisions and fertility concerns. Cancer Nurs. 2011; 34: 32–40.
- Meirow D, Biederman H, Anderson RA, Wallace WH. Toxicity of chemotherapy and radiation on female reproduction. Clin Obstet Gynecol. 2010; 53: 727-739.
- Silvestris E, Cormio G, Skrypets T, Dellino M, Paradiso AV, Guarini A, et al. Novel aspects on gonadotoxicity and fertility preservation in lymphoproliferative neoplasms. Crit Rev Oncol Hematol. 2020; 151: 102981.
- Gorman JR, Usita PM, Madlensky L, Pierce JP. Young breast cancer survivors: Their perspectives on treatment decisions and fertility concerns. Cancer Nurs. 2011; 34: 32–40.
- Hohmann C, Borgmann Staudt A, Rendtorff R, Reinmuth S, Holzhausen S, Willich SN, et al. Patient counselling on the risk of infertility and its impact on childhood cancer survivors: Results from a national survey. J Psychosoc Oncol. 2011; 29: 274–285.
- Ghadjar P, Budach V, Köhler C, et al. Modern radiation therapy and potential fertility preservation strategies in patients with cervical cancer undergoing chemoradiation. Radiat Oncol. 2015; 10: 50. https://doi.org/10.1186/s13014-015-0353-4
- Kroman N, Jensen MB, Wohlfahrt J, Ejlertsen B. Pregnancy after treatment of breast cancer: a population-based study on behalf of Danish Breast Cancer Cooperative Group. Acta Oncol. 2008; 47: 545-549.
- Jensen JR, Morbeck DE, Coddington CC 3rd. Fertility preservation. Mayo Clin Proc. 2011; 86: 45-49.
- Wallace WHB, Thomson AB, Kelsey TW. The radiosensitivity of the human oocyte. Hum Reprod. 2003; 18: 117–121.
- Hürmüz P, Sebag Montefiore D, Byrne P, Cooper R. Successful spontaneous pregnancy after pelvic chemoradiotherapy for anal cancer. Clin Oncol (R Coll Radiol). 2012; 24: 455-457.
- Hatayama Y, Aoki M, Kawaguchi H, Hirose K, Sato M, Akimoto H, et al. Safe and successful birth following pelvic radiotherapy for rectal mucosa-associated lymphoid tissue lymphoma: A case report. J Med Case Rep. 2017; 11: 26.
- Huarte Ciganda M, Estaún Echavarren C, García Jiménez A, Huarte Sala I. Spontaneous Uterine Rupture in the Second Trimester in a Patient With Previous Pelvic Radiotherapy in Childhood: A Case Report. J Obstet Gynaecol Can. 2020; 42: 84-87.
- Saparmi F, Jeyasingam V. Successful spontaneous pregnancy after pelvic radiotherapy for a sacral giant cell tumor: A case report. Precision Radiation Oncology. 2020; 4: 61-63.
- Murphy C, Gilham C. Spontaneous Pregnancy Following Pelvic Irradiation for Anal Cancer: A Case Report. Applied Radiation Oncology December. 2020; 49-51.