
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Extreme brain sagging and transtentorial herniation in spontaneous intracranial hypotension
Jennifer Sartor Pfeiffer1,3*; Katharina Berger2,3; Melanie Schreiber2,3; Annerose Mengel1,3; Ulf Ziemann1,3; Benjamin Bender4ⴕ; Katharina Feil1,3ⴕ
1Department of Neurology & Stroke, University of Tübingen, Tübingen, Germany
2Department of Neurology & Epileptology, University of Tübingen, Tübingen, Germany.
3Hertie-Institute for Clinical Brain Research, University of Tübingen, Tübingen, Germany.
4Department of Diagnostic and Interventional Neuroradiology, University of Tübingen, Tübingen, Germany.
ⴕThese authors contributed equally.
*Corresponding Author : Jennifer Sartor-Pfeiffer
Department of Neurology & Stroke, and Hertie Institute for Clinical Brain Research, Eberhard-Karls University of Tübingen, Hoppe-Seyler-Straße 3, 72076 Tübingen, Germany.
Phone: +49 7071 29 82141;
Email: jennifer.sartor-pfeiffer@med.uni-tuebingen.de
ORCID ID: 0000-0003-0275-1134.
Received : Sep 01, 2022
Accepted : Sep 21, 2022
Published : Sep 28, 2022
Archived : www.jcimcr.org
Copyright : © Sartor-Pfeiffer J (2022).
Abstract
Keywords: Introduction: Spontaneous intracranial hypotension often results in a new-onset headache that is worse with upright posture, along with other neurologic signs and symptoms. It is less rare than once thought and is not usually considered in the differential diagnosis of chronic daily headaches for months.
Keywords: Methods: We present clinical symptoms and unusual imaging findings of a case of spontaneous intracranial hypotensionin time course.
Keywords: Case description: A 34-year-old female suffered from increasingly severe, orthostatic headache for 5 months, and additionally from nausea and recurrent vomiting. Cranial computed tomography revealed slit-like ventricles and suspected cerebral edema. Magnetic resonance imaging further showed extreme brain sagging with beginning herniation of cerebellar tonsils in the foramen magnum and left uncaltranstentorial herniation, consistent with spontaneous intracranial hypotension. Further detailed diagnostic workup, including conventional and dynamic myelography identified spinal meningeal diverticula as the culprit of the massive cerebrospinal fluid leak and the patient underwent surgical ligation of the fistula.
Keywords: Discussion: We discuss diagnostic findings, therapeutic options, and the occurrence of cerebral edema concurrent with spontaneous intracranial hypotension. Cerebral spinal fluid leaks should not be dismissed in patients with new onset of orthostatic headaches and spontaneous intracranial hypotension and treatment should be initiated promptly.
Keywords: Brain edema; Spontaneous intracranial hypotension; Brain sagging; Cerebrospinal fluid leakage; Headache.
Citation: Sartor-Pfeiffer J, Berger K, Schreiber M, Mengel A, Ziemann U, et al. Extreme brain sagging and transtentorial herniation in spontaneous intracranial hypotension. J Clin Images Med Case Rep. 2022; 3(9): 2076.
Introduction/Background
Spontaneous intracranial hypotension is usually presenting with orthostatic headache manifesting minutes after assuming upright position, less often accompanied by nausea, vomiting, dizziness or other symptoms [1]. Defined by the International Classification of Headache Disorders, third edition, it is defined as spontaneously developed headache, temporally related to a Cerebral Spinal Fluid (CSF) leak, and accompanied by CSF hypotension and low lumbar puncture opening pressure (< 60 mm) [2]. However regardless of an incidence of 5/100.000 [1] and preferential affection of women [1], with a mean age of 42.5 years [1] it is not usually considered in the differential diagnosis of chronic daily headaches for months.
We present a case of extreme spontaneous intracranial hypotension in a 34-year-old female patient suffering from chronic position-dependent headaches with suspected cerebral edema on initial imaging.
Case report/case presentation
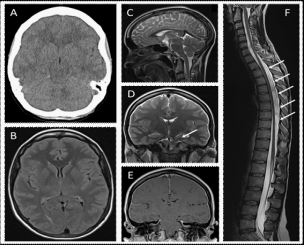
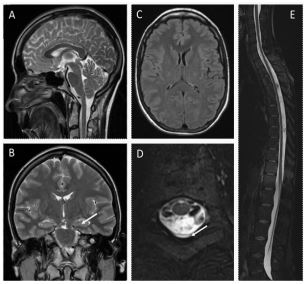
A 34-year-old female suffering from increasingly severe, partly orthostatic headache for 5 months, and additionally from nausea and recurrent vomiting the days before admission presented in our university hospital. Cranial Computed Tomography (CT) revealed slit-like ventricles and suspected cerebral edema (Figure 1A). Magnetic Resonance Imaging (MRI) showed extreme brain sagging with beginning herniation of cerebellar tonsils in the foramen magnum and left uncaltranstentorial herniation, consistent with spontaneous intracranial hypotension (SIH) (Figure 1C-D) as described before, [1] but by far not as pronounced. Conservative standard therapy was initiated including strict bed rest (in Trendelenburg position), hydration, and caffeine for two weeks [1-3]. Since this remained ineffective, CT-controlled autologous Epidural Blood Patch (EBP) (20 ml) was performed at the level of thoracic vertebrae 2/3. As progressive left-sided uncal herniation and mesencephalic compression in MRI (Figure 1D) caused further neurological symptoms including right-sided hemiparesis, EBP (30 ml) was repeated at thoracic vertebrae 8/9. At follow-up after 45 days, the patient was asymptomatic. Cerebral and spinal MRI findings had significantly improved with only a small persistent hygroma at thoracic vertebrae 8/9 (Figure 2D). As the patient suffered from recurrent headache four weeks later, further detailed diagnostic workup, including conventional and dynamic myelography was performed and identified Spinal Meningeal Diverticula (SMD) as the culprit of the massive Cerebrospinal Fluid (CSF) leak; the patient underwent surgical ligation of the fistula.
Discussion/conclusion
SIH is usually presenting with orthostatic headache manifesting minutes after assuming upright position, however regardless of an incidence of 5/100.000 [4] and preferential affection of women, with a mean age of 42.5 years [3] it is not usually considered in the differential diagnosis of chronic daily headaches for months. SIH may be caused by trauma, CSF over-drainage, or spontaneous CSF leak, usually from preexisting weakness of the dural sack, such as SMD [2]. In MRI it can manifest with subdural fluid collections, slit-like ventricles, dilated intracranial sinus and cortical veins, hyperemia of pituitary gland, pachymeningeal gadolinium enhancement and brain sagging, expressed, e.g., by a descent of the cerebellar tonsils below the level of the foramen magnum [1,3]. If standard treatment does not lead to satisfactory resolution of symptoms, an EBP should be performed [3], if possible at the level of an imaging-diagnosed liquor leak [5]. Surgical treatment of visible leaks can also be considered [2,3]. Extradural CSF as a sign for CSF leak is found in 48-76% of cases [3]. The causal relevance of SMD in the development of SIH is still debated [6,7]. A registry reported SMD in 42% of 580 SIH patients, of whom only 22% showed extradural CSF, so that SMD was defined as SIH cause only in these [6]. Surgical treatment of SMD is recommended when less invasive methods, such as EBP as first-line therapy, have failed to achieve the desired treatment success [1,2]. Our patient with chronic headaches presented with extreme brain sagging and transtentorial herniation in imaging due to SIH. There are case reports with severe SIH developing other complications, such as posterior reversible encephalopathy syndrome [8,9] and reversible cerebral vasoconstriction syndrome [9]. Impaired venous drainage produced by brain sagging with functional stenosis of, e.g., vein of Galen was discussed, resulting in swelling, especially of deep brain structures and subsequent cerebral edema [8–10]. This may create a vicious cycle, and in rare cases even rapid neurological deterioration resulting in coma attributed to cerebral herniation was reported [11,12].
Conclusion
In conclusion, although headache being among the most common symptoms in clinical practice and emergency rooms with an annual average prevalence of 13% [13], concerns about a spinal CSF leak should not be dismissed in patients with new onset of orthostatic headaches and SIH. Treatment should be initiated promptly to prevent potentially severe clinical deterioration.
Declarations
Acknowledgement: We thank the participating patient for her consent for publication.
Statement of ethics: Ethics approval was not required (Ethics Committee of the Eberhard Karls University Tübingen).Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Conflict of interest statement: Melanie Schreiber expects funding from Arvelle Therapeutics, which is not related to the present work. Ulf Ziemann received grants from the German Ministry of Education and Research (BMBF), European Research Council (ERC), German Research Foundation (DFG), Janssen Pharmaceuticals NV and Takeda Pharmaceutical Company Ltd., and consulting fees from Bayer Vital GmbH, Pfizer GmbH and CorTec GmbH, all not related to this work. Benjamin Bender is co-founder and share-holder of AIRAmed and has received consultancy fees from Medtronic, all outside of the submitted work. Katharina Feil received funding for Lexi study from Boehringer Ingelheim outside of the here presented work. Jennifer Sartor-Pfeiffer, Katharina Berger and Annerose Mengel have no competing interests to declare.
The authors did not receive support from any organization for the submitted work.
Funding sources: Authors must give full details about the funding of any research relevant to their study, including sponsor names and explanations of the roles of these sources in the preparation of data or the manuscript.
Author contributions: All authors contributed to diagnosis and treatment of the described patient. Material preparation, data collection and analysis were performed by Jennifer Sartor-Pfeiffer Benjamin Bender and Katharina Feil. The first draft of the manuscript was written by Jennifer Sartor-Pfeiffer and all authors commented on versions of the manuscript. All authors read and approved the final manuscript.
Data availability statement: All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
References
- D’Antona L, Jaime Merchan MA, Vassiliou A, et al. Clinical presentation, investigation findings, and treatment outcomes of spontaneous intracranial hypotension syndrome: A systematic review and meta-analysis. JAMA Neurol. 2021; 78: 329-337.
- Olesen J et al. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018; 38: 1-211.
- Mokri B. Spontaneous low pressure, low CSF volume headaches: Spontaneous CSF leaks. Headache. 2013; 53: 1034-1053.
- Schievink WI, Maya MM, Jean Pierre S, Nuño M, Prasad RS, Moser FG. A classification system of spontaneous spinal CSF leaks. Neurology. 2016; 87: 673-679.
- Savoiardo M, Minati L, Farina L, et al. Spontaneous intracranial hypotension with deep brain swelling. Brain. 2007; 130: 1884-1893.
- Pugliese S, Finocchi V, Borgia ML, et al. Intracranial hypotension and PRES: Case report. J Headache Pain. 2010; 11: 437-440.
- Feil K, Forbrig R, Thaler FS, et al. Reversible cerebral vasoconstriction syndrome and posterior reversible encephalopathy syndrome associated with intracranial hypotension. Neurocrit Care. 2017; 26: 103-108.
- Ghavanini AA, Scott CA, Chan DK, Tang Wai DF. Management of patients with spontaneous intracranial hypotension causing altered level of consciousness: Report of two cases and review of literature. Cephalalgia. 2013; 33: 43-51.
- Stovner LJ, Andree C. Prevalence of headache in Europe: A review for the Eurolight project. J Headache Pain. 2010; 11: 289-299.