
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Age estimation at puberty, avoiding extrapolation using a non-invasive easily applicable method
Jean Claude Pineau1; Fernando V Ramirez Rozzi2,3
1CNRS, BABEL, Université de Paris, Paris, France.
2Eco-anthropologie (EA), Muséum national d’Histoire naturelle, CNRS, Université de Paris Cité, Musée de l’Homme, Paris, France.
3EA 2496, Faculté de Chirurgie Dentaire, Université de Paris Cité, Montrouge, France.
*Corresponding Author : Fernando VR Rozzi
Eco-anthropologie (EA), Muséum national d’Histoire naturelle, CNRS, Université de Paris Cité, Musée de l’Homme, Paris, France.
Email: fernando.ramirez-rozzi@mnhn.fr
Received : Aug 24, 2022
Accepted : Sep 22, 2022
Published : Sep 29, 2022
Archived : www.jcimcr.org
Copyright : © Rozzi FVR (2022).
Abstract
Age determination in children and adolescents of unknown age is often based on the degree of bone development (Greulich and Pile method). However, the variability of development at puberty, extrapolation to other populations and the use of invasive means make the reliability and feasibility of this method uncertain. Using pubertal criteria that are simple to identify and easily applicable to any population, we distributed a sample of Tunisian adolescents aged 11 to 16 years into pubertal stages. A nonlinear model between pubertal stages and chronological age was obtained by weighted line square procedures using quantile-quantile plots. Tunisian adolescents have an advanced onset of puberty of slightly more than 13 months compared to French adolescents. The use of our model allowed us to estimate with good accuracy the age of Tunisian adolescents based on their biological maturation. The mean differences between estimated age and actual age from these values were 0.12 ± 0.66 years. In 60% of the cases, the differences between chronological age and estimated age are between ± 6 months. The procedure followed uses simple pubertal criteria. This allows the development of a model for age attribution easily applicable to any population and thus avoids the drawbacks observed in other methods.
Keywords: Pubertal stages; Greulich and pile method; Ethnicity; Nonlinear model; Estimated age.
Citation: Pineau JC, Rozzi FVR. Age estimation at puberty, avoiding extrapolation using a non-invasive easily applicable method. J Clin Images Med Case Rep. 2022; 3(9): 2079.
Introduction
The determination of age at puberty is of great importance from a sociological, anthropological and legal point of view. Age estimation techniques are usually based on the assessment of skeletal development in particular from the biometric analysis of hand bones [1], ratio of hand bone area [2,3] and more commonly through hand bone development compared to standard models such as that of Greulich and Pyle (GP) [4]. From the analysis of radiographs of hand and wrist, GP proposed a model of skeletal age based on standard stages which correspond to chronological age. Largely employed [5-10], the use of this method however merits some comments especially concerning the stages of development, the extrapolation to other populations and its invasive nature.
The use of the GP method involves the estimation of chronological age from bone development. Bone development is correlated to pubertal stages and for the same pubertal stage there is a significant difference in age according to ethnicity [11]. It is therefore obvious that the GP method has severe limitations in the extrapolation to another population whose ethnicity is different from that of the population that was used to construct it [12]. It is worth noting that the GP method is widely used by prosecutors and judges to establish the marital status of adolescents and to estimate the age of individuals from abroad. There are two major drawbacks to this use. First, as discussed above, the relationship between stages of bone development and a specific age does not account for variations in development at puberty, and furthermore extrapolation of this method to other ethnic groups has biases whose magnitude has yet to be established. Secondly, the application of the GP method involves the taking of X-rays, which, being an invasive method, requires the consent of the person in question, which in many cases leads to his refusal. This makes it impossible to estimate the age and leads to a halt of the expertise process.
The strength of the GP method which indeed justifies its widespread use in determining age is based on the close relationship between bone development changes and reproductive system changes. These changes, ‘are directly responsible for most of the perceptible external changes on which the estimation of general body maturity is usually based’ (Greulich and Pile 1959, page 18). Thus, establishing a method that relies on external body changes to estimate maturation and infer the age of individuals, would make assessment easier and more direct because it would not involve analysis of bone development neither the use of invasive methods.
The objective of this study is to establish a reliable prediction of the chronological age of adolescents using a non-invasive method with simple pubertal criteria that can be widely applied to different and diverse populations. We applied the method to Tunisian individuals of a known age. The model established differs from the one proposed for European populations reinforcing the idea of the non-extrapolation of the models and the need to develop models for each ethnic population.
Materials and methods
A sample of 238 Tunisian school-going boys, known to be between 11 and 16 years of age, from the Keff region in northwestern Tunisia was included in this study. All individuals were medically healthy and belonged to an urban, non-traditional “village” environment. The permission of the advising doctors and the regional education authority of Aisne was procured, all in accordance with the Helsinki Declaration. All participants and parents gave their oral and written informed consent to participate in this study.
Since the determination of sexual characteristics such as external genitalia is not ethically conceivable, the assessment of maturity was established from the evaluation of secondary sexual stages using a simplification of the Tanner stages [13].
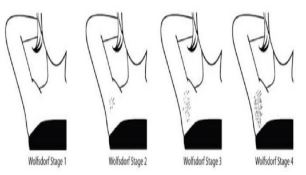
Four puberty stages were established based on three qualitative criteria that allow us to differentiate the subjects: facial and axillary pilosity as well as voice change. The different stages of axillary hair according to the Wolfsdorf classification [14] are illustrated in Figure 1. The physician had to check 2 boxes corresponding to axillary hair and then face pilosity with voice change. The four stages are illustrated in Table 1. When the axillary and face pilosity matched, we retained the indicated stage. In the event of conflict between stages, we kept the higher stage. In practice, the majority of stages concerned no more than two consecutive stages.
Table 1: Stages corresponding to degrees of biological puberty.
| ST1 Below the age of puberty Stage 1 of Tanner | ST2 Pre-pubescent Stage 2 of Tanner | ST3 Para-pubescent Stage 3 and 4 of Tanner | ST4 Pubescent Stage 5 of Tanner | |
| Axillary hair Face pilosity Voice change | No hair No facial hair Soft voice | Start of hairgrowth Facial hair Voice instability | Very visible Moustache Deep voice | Thick hair growth Abundant beard hair Deep voice |
A model establishing a correspondence between pubertal stages and chronological age was obtained by weighted line square procedures using a quantile-quantile plot. The mean chronological age at each pubertal stage was obtained. Mean difference (d) in years between the Chronological Age (CA) and the Estimated Age (EA) was calculated for each age group. For all tests, P< .05 was considered significant. Statistical tests were performed using Statistica software (version 6; StatSoft, Tulsa, Okla, USA).
The results from the Tunisian population were compared to those from a French population (Student t-test).
Results
The mean and standard deviation of the differences between the actual chronological age and the estimated age (in years) are presented in Table 2. The distribution of differences between Chronological Age (CA) and Estimated Age (EA) is Gaussian X²= 2.75 (P=0.43). In 60% of the cases, the differences between CA and EA are between ±6 months (Figure 2).
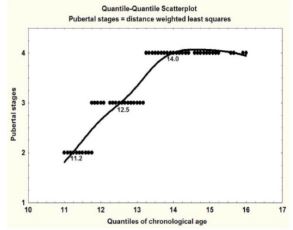
The model for Tunisian boys obtained by weighted line square procedures using a quantile quantile plot is shown in Figure 3. The correspondence between pubertal stages and chronological age in the quantile-quantile plot is 11.2 years for ST2, 12.5 years for ST3 and 14.0 years for ST4.
Comparison with a French population
In a previous study [15], we mapped a correspondence between pubertal stages and chronological age from a sample of 170 French boys aged 11 to 16 years, followed up longitu dinally for 5 consecutive years. The database was made up of 1135 measurements of the French teenagers. The fitted model was also obtained by weighted line square procedures using quantile-quantile plots. Under these conditions the optimization of age according to the pubertal stage in the different age groups led us to retain the following values: 11.9 years at ST1, 12.9 years at ST2, 13.9 years at ST3 and 14.9 years at ST4. Mean differences between CA and the EA were 0.06 ± 0,91 years.
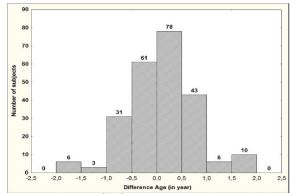
Table 2: Comparison between chronological age and estimated age of the Tunisian boys.
| Age groups (years) | N | d ± SD (years) |
| [11-12[ [12-13[ [13-14[ [14-15[ [15-16] Total |
45 51 87 41 14 238 |
-0.01 ± 0.38 -0.15 ± 0.65 -0.04 ±0.57 0.46 ± 0.36 1.54 ± 0.35 0.12 ± 0.66 |
Comparison of the chronological age of the Tunisian and French boys based on the pubertal stage shows a difference in distribution (Table 3). The percentage of pubertal adolescents among Tunisian boys is much higher (P< 0.01) than among French boys. At the pubertal stages ST2 ST3 and ST4, a statistically significant difference (P<0.01) between the average ages of the Tunisian boys and French boys exists (Table 4). Beyond the age of 15, all Tunisian adolescents are pubescent and therefore, if the French model is applied to Tunisians, the average gap is overestimated by +1.54 years. Consequently, the maturation of Tunisian boys is much more advanced than that of the French boys. Tunisian adolescents have an advanced puberty of more than 13 months. In these conditions, the model of age estimation according to pubertal stages established for French adolescents does not apply to the Tunisian sample.
Table 3: Proportion of individuals (11-16 years of age) according to pubertal stage in both populations.
| Variables | Tunisians n=238 | French n=170 |
| Puberty stages ST1 ST2 ST3 ST4 |
% - 15.6 33.6 50.8 |
% 12.5 42.6 30.9 14.0 |
Table 4: Mean and standard deviation of age (in years) at each pubertal stage for French and Tunisian adolescents.
| Sample | Sample Average age (years) | ST1 | ST2 | ST3 | ST4 |
| French Tunisians |
13.9 ± 1.1
Average age (years) 13.3 ± 1.2 Average age (years) |
n=66
12.9 ± 0.26 - |
n=477
13.3 ± 0.60 n = 37 11.3 ± 0.2 |
n= 471
14.1 ± 0.77 n = 80 12.8 ± 0.5 |
n = 121
15.1 ± 0.76 n = 121 14.0 ± 0.8 |
Discussion
The most frequently employed method for age estimation is based on bone development using the Greulich & Pyle Atlas [6,16-19]. GP suggest that ‘the maturation changes in the skeleton are intimately linked to those of the reproductive system. These in turn, are directly responsible for most of the externally discernible changes on which the estimation of general body maturity is usually based’. External body maturity changes are closely linked to changes in bone development. Thus, they proposed that bone development can be used to infer individual maturation and to suggest an estimation of individual age. In other words, the basis of the GP thinking is the relationship between ‘the externally discernible changes’ of maturation and changes in skeletal development. The atlas built by them is a qualitative method using reference radiographic images of the left wrist and hand from birth to 19 years of age.
Comparing bone development by the degree of ossification in hand and wrist bones in individuals with reference images in the GP Atlas enables the estimation of age. The variability in development depends on age as variability increases at puberty [20,21]. At puberty the development of individuals can be advanced, standard or delayed [11]. Therefore, the establishment of the type of development at puberty is of extreme importance because it determines the channel of development that the individual will follow until the adult stage [11]. In other words, the fairly narrow developmental channel that allows the use of the GP method during childhood diversifies and adopts a wide variability during adolescence. GP knew that puberty implies a wider variability in development and add an intermediate stage (6 months) to the earlier and later stages (1 year). They, however, keep only one model for each stage and so the variability of their model accepts that it remains very limited compared to the three types of development at puberty. Our results highlight this variability because the Tunisians, although having an average age close to, but lower than that of the French, display an advanced stage of development (Tables 3,4).
Although the Greulich and Pyle technique seems to show good reliability, the applicability of this method to ethnically distinct populations should be carried out with caution [22,23], sometimes the method needs to be recalibrated to the population under study [24]. Recently, Alshamrani et al. [25] have assessed the accuracy of the GP atlas in 49 previous studies to estimate age in different groups coming from different geographic regions. They suggested that the GP atlas should be used with caution when applied to Asian male and African female populations. It is worth noting that this study is based on the analysis of groups coming from large world areas like ‘Asia’ or populations with large geographic distribution like ‘Caucasian’ or ‘Hispanic’ and thus does not take into account the high degree of heterogeneity of these large groups. It is very likely that variation differs between ethnic groups, even between those that inhabit the same geographical area today, as they may have followed different adaptive and evolutionary mechanisms throughout their history.
Some studies have reported major mean differences and standard deviations between bone age and chronological age for different groups. For instance, the GP standards are imprecise for African - American boys where the mean difference and standard deviation between chronological and estimated age is -0.32 ± 1.14 (n=39) and 1.87 ± 1.47 years on 8–15-year-old teenagers [23]. The same is true for South African boys with a difference between chronological and estimated age greater than ± 2.3 years [24] and for Moroccan boys with 95% difference about ± 3.4 years [12]. In general, the differences between chronological age and the age estimated from the GP method remain within the ± 2.5-year interval in 95% of cases for adolescents aged 13 and 14 years. The dispersion of the differences is often higher at the time of the growth peak when the maturation of the individuals offers a greater variability.
The determination of the chronological age of adolescents represents a very important source of information in many expert reports. From a legal point of view, magistrates need to know a precise age range for minors, adhering to the laws established at a European level [26]. In many cases, especially in the case of migrants, minors do not belong to the same group that served as a reference for Greulich & Pile, thus, as outlined above, its effectiveness remains doubtful. This method implies, in addition to the remarks we have just discussed, the taking of X-rays, an invasive method which requires prior agreement from the individual and in some cases of an ethics committee. The refusal by either party may lead to a situation where it is impossible to determine the age of the individual thus preventing the expert from making a decision.
As a result of the procedure used in this study, the reservations associated with the Greulich and Pile method do not exist. It succeeds in carrying out a study of living individuals, fulfilling the four demands advanced by Ritz-Timme et al. [27], better than others. Firstly, our analysis is based on the formation of groups according to pubertal stage, allowing better control of age variability within each stage of biological maturation. Secondly, pubertal stages are determined from direct biological maturation characteristics without the use of indirect and invasive means such as X-rays. Thirdly, once the pubertal stages have been established, the weighted line squares procedure enables us to obtain the value of the chronological age associated with each pubertal stage. Fourthly, this method makes the development of models for each ethnic group possible, a very important aspect because the relationship between pubertal maturation and chronological age is not the same for all populations.
Conclusion
The sample was distributed according to pubertal stages determined from simple and direct biological maturation characteristics. It was then possible to establish that the Tunisian teenagers although having a similar average age presented a development in advance of more than one year compared to the French teenagers. This result supports the idea that extrapolation of models between different ethnic groups should be avoided. Thus, extrapolation of models to determine the age of individuals, such as that of Greulich and Pile, may introduce such a large bias that the effectiveness of its application remains questionable.
The weighted line squares method applied to pubertal stages allows the development of models specific to the population under study. The combination of this method and the analysis of simple and direct characteristics of biological maturation avoids the biases observed in other methods. The simplicity and accuracy of this procedure means that it could well be used within a medico-legal framework in response to legal requests in the near future.
Declarations
Funding: The authors received no specific funding for this work.
Competing interests: The authors declare no competing interests.
Informed consent: This study was carried out in accordance with the Helsinki Declaration. All participants and parents gave their oral and written informed consent to participate in this study. The permission of the advising doctors and the regional education authority of Aisne was procured.
References
- Lalys L. Estimation de l’âge des immatures par la biométrie radiologique des os de la main. Biometrie Hum Anthropol. 2013; 31: 133–137.
- De Luca S, Mangiulli T, Merelli V. A new formula for assessing skeletal age in growing infants and children by measuring carpals and epiphyses of radio and ulna. Forensic Sci Int. 2016; 39: 109–116. https://doi : 10.1016/j.jflm.2016.01.030
- Cameriere R, Ferrante L, Mirtella D. Carpals and epiphyses of radius and ulna as age indicators. Int J Legal Med. 2006; 120: 143–146. https://doi: 10.1007/s00414-005-0040-3
- Greulich WW, Pyle SI. Radiographic atlas of skeletal development of the hand and wrist, 2nd edn. Stanford, CA: Stanford University Press. 1959;
- Büken B, Erzengin ÖU, Büken E, et al. Comparison of the three age estimation methods: which is more reliable for Turkish children? Forensic Sci Int. 2009; 183: 103e1–103e7. https://doi: 10.1016/j.forsciint.2008.10.012
- Moradi M, Sirous M, Morovatti P. The reliability of skeletal age determination in an Iranian sample using Greulich and Pyle method Forensic Sci Int. 2012; 223: 372e1-372e4. https:// doi:10.1016/j.forsciint.2012.08.030
- Patil ST, Parchand MP, Meshram MM, Kamdi NY. Applicability of Greulich and Pyle skeletal age standards to Indian children. Forensic Sci Int 2012; 216: 200.e1-200e4. https://doi: 10.1016/j.forsciint.2011.09.022
- Schmidt S, Nitz I, Ribbecke S, Schultz R, Pfeiffer H, et al. Skeletal age determination of the hand: A comparison of methods. Int J Legal Med. 2013; 127: 691-698. https:// doi:10.1007/s00414-013-0845-4
- Urschler M, Krauskopf A, Widek T, Sorantin E, Ehammer T, et al. Applicability of Greulich -Pyle and Tanner-Whitehouse grading methods to MRI when assessing hand bone age in forensic age estimation: A pilot study. Forensic Sci Int. 2016; 266: 281-288. https://doi:10.1016/j.forsciint.2016.06.016
- Pinchi V, De Luca F, Ricciardi F, Focardi M, Piredda V, Mazzeo E, et al. Skeletal age estimation for forensic purposes: A comparison of GP, TW2 and TW3 methods on an Italian sample. Forensic Sci Int. 2014; 238: 83–90. https://doi:10.1016/j.forsciint.2014.02.030
- Pineau JC, Ramirez Rozzi FV. The same growth pattern from puberty suggests that modern human diversity results from changes during pre-pubertal development. Sci Rep. 2021; 11: 4817. https://doi:10.1038/s41598-021-84327-1
- Garamendi PM, Landa MI, Ballesteros J, Solano MA. Reliability of the methods applied to assess age minority in living subjects around 18 years old: A survey on a Moroccan origin population. Forensic Sci Int. 2005; 154: 3–12. https://doi:10.1016/j.forsciint.2004.08.018
- Tanner JM, Whitehouse RH, Resele L. The adolescent frowth spurt of boys and girls of the Harpenden growth study. Annals of Human Biology. 1976; 3: 109-126. https://doi:10.1080/03014467600001231
- Renthal N. Nora’s Endomemory: A Pocket Manual for Pediatric Endocrinology Fellows. 2014; www.rocketguts.com
- Pineau JC. Age estimation of teenage boys during puberty. Am J Forensic Med Pathol. 2020; 41: 188-193. https://doi:10.1097/PAF.0000000000000573
- van Rijn RR, Lequin MH, Robben SG, Hop WC, Van Kuijk C, et al. Is the Greulich and Pyle atlas still valid for Dutch Caucasian children today? Pediatr Radiol. 2001; 31: 748–752. https://doi:10.1007/s002470100531
- Santoro V, Roca R, De Donno A, et al. Applicability of Greulich and Pyle and Demirijan aging methods to a sample of Italian population. Forensic Sci Int. 2012; 221: 153.e1–153.e5. https://doi:10.1016/j.forsciint.2012.04.014
- Paxton ML, Lamont AC, Stillwell AP. The reliability of the Greulich-Pyle method in bone age determination among Australian children: bone age determination using Greulich Pyle. J Med Imaging Radiat Oncol. 2013; 57: 21–24. https://doi:10.1111/j.1754-9485.2012.02462.x
- Soudack M, Ben Shlush A, Jacobson J, Raviv Zilka L, Eshed I, Hamiel O, et al. Bone age in the 21st century: is Greulich and Pyle’s atlas accurate for Israeli children? Pediatr Radiol. 2012; 42: 343–348. https://doi:10.1007/s00247-011-2302-1
- Chaumoitre K, Colavolpe N, Marciano Chagnaud S, Dutour O, Boetsch G, Panuel M, et al. Validité de l’atlas de Greulich et Pyle appliqué à une population actuelle. J Radiol. 2007; 88: 1376. https://doi:10.1016/S0221-0363(07)81979-2
- Zabet D, Rerolle C, Pucheux J, Telmon N, Saint Martin P, et al. Can the Greulich and Pyle method be used on French contemporary individuals? Int J Legal Med. 2015; 129: 171-177. https://doi:10.1007/s00414-014-1028-7
- Zhang A, Sayre JW, Vachon L, Liu BJ, Huang HK, et al. Racial differences in growth patterns of children assessed on the basis of bone age. Radiology. 2009; 250: 228–235. https://doi:10.1148/radiol.2493080468
- Mansourvar M, Ismail MA, Raj RG, et al. The applicability of Greulich and Pyle atlas to assess skeletal age for four ethnic groups. J Forensic Leg Med. 2014; 22: 26–29. https://doi:10.1016/j.jflm.2013.11.011
- Dembetembe KA, Morris AG. Is Greulich–Pyle age estimation applicable for determining maturation in male Africans? S Afr J Sci. 2012; 108. http:// dx.doi.org/10.4102/sajs.v108i9/10.1036
- Alshamrani K, Messina F, Offiah AC. Is the Greulich and Pyle atlas applicable to all ethnicities? A systematic review and meta-analysis. European Radiology 2019; 29: 2910–2923. https://doi:10.1007/s00330-018-5792-5
- Feijen L. The Challenges of ensuring protection to unaccompanied and separated children in composite flows in Europe. Refug Surv Q. 2008; 27: 63–73. https://doi:10.1093/RSQ/HDN049
- Ritz Timme S, Cattaneo C, Collins MJ, Waite ER, Schütz HW, et al. Age estimation—the state of the art in relation to the specific demands of forensic practice. Int J Legal Med. 2000; 113: 129–136. https://doi:10.1007/s004140050283