
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Axillary artery aneurysm as rare cause of concurrent cerebellar infarct and acute limb ischemia: A case report
Xiaolin Jia1; Prashanth Krishna Mohan2; Karthik Mikkineni3
1Department of Medicine, Stanford University, Stanford Health Care Valley Care Hospital. 5555 W Las Positas Blvd, Pleasanton, CA 94588, USA.
2Department of Neurology and Neurological Sciences, Stanford University, Stanford Health Care Valley Care Hospital. 5555 W Las Positas Blvd, Pleasanton, CA 94588, USA.
3Department of Vascular Surgery, Stanford University Hospital, 300 Pasteur Dr. Stanford, CA 94305, USA.
*Corresponding Author : Xiaolin Jia
Department of Medicine, Stanford University, Stanford Health Care Valley Care Hospital. 5555 W Las
Positas Blvd, Pleasanton, CA 94588, USA.
Email: kjia@stanford.edu
Received : Sep 02, 2022
Accepted : Sep 26, 2022
Published : Oct 03, 2022
Archived : www.jcimcr.org
Copyright : © Jia X (2022).
Citation: Jia X, Mohan PK, Mikkineni K. Axillary artery aneurysm as rare cause of concurrent cerebellar infarct and acute limb ischemia, a case report. J Clin Images Med Case Rep. 2022; 3(10): 2083.
Introduction
Axillary artery aneurysms are well documented and have potentially severe or life-threatening complications [1-3]. While pseudoaneurysms of the axillary artery can be caused by trauma or iatrogenic complications, true aneurysms are often due to repeated blunt trauma to the axillary artery over time, leading to weakening of the artery wall. The most common example is prolonged crutch use, though some athletes who have repetitive forceful movement of the upper limb, such as baseball players, may also be at risk [3]. Rarer causes include degenerative disorders such as Marfan’s syndrome or inflammatory diseases such as vasculitis [2]. Potential complications of axillary artery aneurysms include neurologic or vascular compromise of the involved upper extremity. Here we report the rare case of a patient presenting with concurrent acute cerebellar stroke and critical limb ischemia as embolic complications of axillary artery aneurysm.
Case report
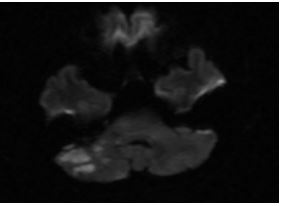
57 year old Asian male with history of childhood poliomyelitis with residual right lower extremity atrophy and chronic crutch use presented with 12 hours of right-sided hearing loss, vertigo, and right arm numbness. His past medical history included hypertension and hyperlipidemia successfully managed with lifestyle modification. Physical exam confirmed decreased hearing on the right ear, left horizontal nystagmus, otherwise normal exam with equal 1+ radial pulse bilaterally. CT head showed subtle hypoattenuation in the right inferior cerebellar hemisphere suspicious for right Posterior Inferior Cerebellar Artery (PICA) territory infarct. MRI brain and MR Angiogram had and neck revealed small acute infarction in the right inferior cerebellum involving the Anterior Inferior Cerebellar Artery (AICA) and PICA vascular territories; chronic lacunar infarction in the left cerebellum. No flow-limiting stenosis noted in the head and neck vasculature.
Further stroke workup included transthoracic echo with bubble study which was negative for patent foramen ovale and transesophageal echo which was negative for cardiac source of emboli. Hypercoagulable workup and CT of chest, abdomen and pelvis were all unremarkable. Telemetry was without atrial fibrillation. He was started on aspirin 81 mg, atorvastatin 80 mg, and DVT prophylaxis.
On hospital day 3 patient reported right arm and hand numbness and coolness. These symptoms started concurrently with the stroke but spontaneously improved, so they were not reported until hospital day 3 when symptoms suddenly worsened. Exam showed decreased sensation over the right forearm and hand, decreased radial pulse on the right compared to the left, and right hand coolness to touch. Strength was intact. Right upper extremity CT Angiography (CTA) showed occlusive thrombus in the axillary artery and proximal brachial artery.

At this point, he was started on a heparin drip and taken for urgent right arm embolectomy. Intraoperative ultrasound showed the presence of an axillary artery aneurysm with intramural thrombus. This was not evident on CTA due to complete occlusion and healthy vessel wall. Patient subsequently underwent embolectomy, resection of the axillary aneurysm and bypass with saphenous vein graft.
Post operatively patient had return of right arm neurovascular function. He was discharged on dual antiplatelet therapy with aspirin 81 mg and clopidogrel 75 mg daily given the bypass graft. At six months follow up he showed complete recovery with no further episodes of stroke.
Discussion
Repeated blunt trauma to the axillary artery results in artery wall weakening and axillary artery aneurysms. Our patient with childhood polio and prolonged crutch use is certainly at risk. Aneurysms resulting from crutch-use are more frequently accompanied by intraluminal thrombus due to sluggish blood flow through the dilated area of the aneurysm [2]. The thrombus may dislodge due to repeated trauma and cause acute, chronic, or repetitive emboli, especially to the affected upper extremity [3]. Very few cases of cerebral embolism from a peripheral arterial occlusion have been reported, and none in the setting of axillary artery aneurysm.
The most frequent cause of stroke is atherosclerosis, followed by cardioembolism. Approximately 5% of strokes are caused by cervical artery dissections, nonatherosclerotic vasculopathies, vasculitis, and collagen vascular diseases. Even after thorough evaluation, around 30% of strokes are cryptogenic - no specific cause is identified, and the classic risk factors are not present [4]. Most cryptogenic strokes are considered Embolic Strokes of Undetermined Source (ESUS), especially if pattern of infarction suggest an embolic cause [6]. However anticoagulation such as rivaroxaban are not superior to aspirin in preventing recurrent strokes in patients with history of ESUS [7]. The current secondary prevention for cryptogenic strokes consists of vascular risk factor modification and treatment with antiplatelet therapy [5].
Our patient presented with symptoms consistent with acute AICA territory stroke, such as vertigo, hearing loss, ataxia, nystagmus, and numbness [8]. Concurrently, he experienced intermittent right arm numbness and weakness associated with hand coolness and decreased pulse. The right upper extremity symptoms are not due to stroke but a separate vascular occlusive phenomenon. The temporal correlation of stroke symptoms with symptoms of arterial occlusion suggest that the patient had embolic events from a common source causing both right arm ischemia as well as right AICA and PICA territory infarction. The source of emboli was found to be an axillary artery aneurysm with intramural thrombus. A proposed mechanism is retrograde flow and embolization of the cerebral artery due to occlusion and lack of forward flow from the thrombosed peripheral artery [9,10].
Treatment of axillary artery aneurysm depends on patient presentation. For patients presenting with acute limb ischemia, recanalization of the occluded artery should be considered as soon as possible via either catheter-directed thrombolysis or surgical thrombectomy. After recanalization, aneurysms should be treated with surgical resection and reconstruction with graftor aneurysm exclusion with subsequent bypass grafting [2]. For asymptomatic patients incidentally found to have axillary artery aneurysm, treatment depends on risk of complications. Aneurysms containing a thrombus should have surgical treatment to prevent potential embolisms. If no thrombus is present, it may be reasonable to closely monitor the aneurysm [1], however other potential risks can occur including extrinsic compression or aneurysm rupture, so shared decision-making with the patient is important.
Conclusion
True aneurysms of the axillary artery, though rare, should be considered in the patient with risk factors (i.e. prolonged crutch use, degenerative or inflammatory disease history) presenting with neurologic or embolic symptoms. In addition to affecting the involved upper extremity, it can be a source of embolic strokes and a careful search for potential peripheral arterial occlusions, especially involving the upper extremities, should be considered in certain patient populations presenting with cryptogenic strokes.
References
- Konishi T, Ohki S, Saito T, Misawa Y. Crutch-induced bilateral brachial artery aneurysms. Interactive Cardiovascular And Thoracic Surgery. 2009; 9: 1038-1039.
- Furukawa K, Hayase T, Yano M. Recurrent upper limb ischaemia due to a crutch-induced brachial artery aneurysm. Interactive Cardiovascular And Thoracic Surgery. . 2013; 17: 190-192.
- Moon I, Hwang J, Kim J. Recurrent Upper Extremity Embolism Due to a Crutch-Induced Arterial Injury: A Different Cause of Upper Extremity Embolism. Annals Of Vascular Surgery. 2010; 24: 554.e7-554.e12.
- Ionita C, Xavier A, Kirmani J, Subasini D, Divani A, Qureshi A, et al. What Proportion of Stroke Is Not Explained by Classic Risk Factors?. Preventive Cardiology. 2005; 8: 41-46.
- Schulz U. Cryptogenic stroke – How to make sense of a non-diagnostic entity. Maturitas. 2019; 122: 44-50.
- Diener H, Grond M. Embolic Stroke of Undetermined Source. Cardiovasc. 2018; 18: 38-40.
- Hart R, Sharma M, Mundl H, Kasner S, Bangdiwala S, Berkowitz S, et al. Rivaroxaban for stroke prevention after embolic stroke of undetermined source. Journal Of Vascular Surgery: Venous And Lymphatic Disorders. 2019; 7: 147.
- Lee H. Neuro-Otological Aspects of Cerebellar Stroke Syndrome. Journal Of Clinical Neurology, 2009; 5: 65.
- Baek JH, Shin DH, Kang CK, Lee YB, et al. Distal subclavian artery occlusion causing multiple cerebral infarcts consequence of retrograde flow of a thrombus?. J Cerebrovasc Endovasc Neurosurg. 2013; 15: 221‐224.
- WH Chen, SS Chen, JS Liu. Concurrent cerebral and axillary artery occlusion: A possible source of cerebral embolization from peripheral artery thrombosis. Clin Neurol Neurosurg. 2005; 108: 93-96.