
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Mastitis tuberculosis: About an uncommon case report
Aziz Slaoui*; Jihane El Moudane; Oumaima Mourran; Najia Zeraidi; Amina Lakhdar; Aicha Kharbach; Aziz Baydada
Gynaecology-Obstetrics and Endoscopy Department, Maternity Souissi, University Hospital Center IBN SINA, University Mohammed V, Rabat, Morocco.
*Corresponding Author : Aziz Slaoui
Gynaecology-Obstetrics and Endoscopy Department & Gynaecology-Obstetrics and Endocrinology Department, University Mohammed V, Rabat, Morocco.
Email: azizslaoui27@gmail.com
Received : Aug 11, 2022
Accepted : Sep 27, 2022
Published : Oct 04, 2022
Archived : www.jcimcr.org
Copyright : © Slaoui A (2022).
Abstract
Background: Mastitis tuberculosis is a very unusual form of extrapulmonary tuberculosis, even in endemic countries. The clinical and imaging features are not specific to this condition, which must be distinguished from other mammary pathologies, especially breast cancer, in order to avoid investigations and treatments that are sometimes mutilating.
Case presentation: We report an uncommon case of breast tuberculosis in a 39-year-old woman. The ultrasound and mammography performed suggested a lesion suspicious of cancer classified as ACR 5. Pathological examination confirmed tuberculosis of the breast. Anti-tuberculosis medical therapy resulted in a complete cure of the condition.
Conclusions: Mammary extrapulmonary tuberculosis is uncommon and presents a difficult diagnostic challenge that requires a high degree of suspicion, especially in endemic areas. The clinical and radiological pictures are misleading, and raise a diagnostic problem especially with breast cancer. But it is only the histopathological or bacteriological examination that allows a diagnosis of certainty.
Keywords: Breast tuberculosis; Mastitis tuberculosis; Breast cancer.
Abbreviations: MRI: Magnetic Resonance Imaging; WHO: World Health Organization; TB: Tuberculosis; HIV: Human Immunodeficiency Virus; AIDS: Acquired Immunodeficiency Syndrome.
Citation: Slaoui A, Moudane JE, Mourran O, Zeraidi N, Lakhdar A, et al. Mastitis tuberculosis: About an uncommon case report. J Clin Images Med Case Rep. 2022; 3(10): 2085.
Background
Mastitis tuberculosis is a very unusual form of extrapulmonary tuberculosis, even in endemic countries. This is a very unusual clinical entity since mammary glandular tissue, like the spleen and skeletal muscle, is resistant to the survival and multiplication of the tuberculosis bacillus [1-4]. It represents 0.06 to 0.1% of all tuberculosis sites [1-4]. The clinical and imaging features are not specific to this condition, which must be distinguished from other mammary pathologies, especially breast cancer, in order to avoid investigations and treatments that are sometimes mutilating [5-7]. We hereby report an uncommon case of breast tuberculosis to raise the problem of differential diagnosis of breast tuberculosis with breast cancer.
Case presentation
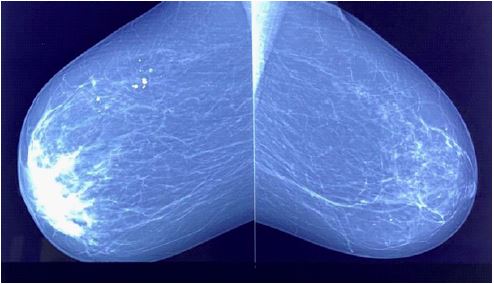
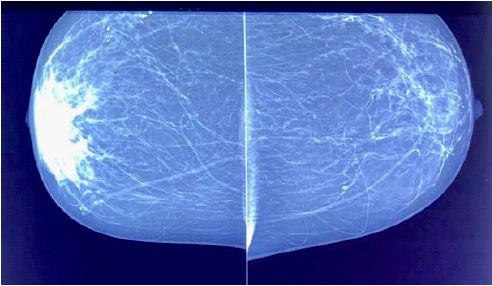
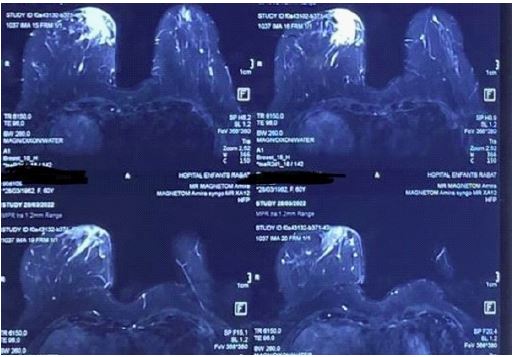
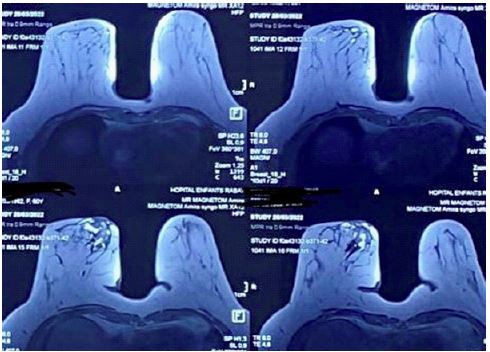
We present the uncommon case of a 39-year-old female patient, with 4 children delivered vaginally, from a low socioeconomic background, without any particular history, in particular no notion of tuberculosis infection, who presented to our training for mastodynia that had appeared six months earlier. The clinical examination revealed an inflamed left breast (Figures 1 and 2) with homolateral axillary adenopathies suggesting locally advanced left breast cancer. The right breast was without abnormality as was the rest of the clinical examination. Mammography (Figures 3 and 4) showed a significant increase in density of the left breast, predominantly in the retro areolar region, with diffuse thickening of the skin soft tissues without nodular lesions or microcalcifications. Breast ultrasound showed diffuse skin thickening with infiltration of the breast tissue, especially in the retro-areolar region, associated with multiple hypoechoic axillary adenopathies, the largest of which measured 13 mm x 9 mm. The lesion was classified as ACR 5. A complementary breast MRI (Figures 5 and 6) had also shown a left mastitis. A skin biopsy and a biopsy of the breast lesion were performed. Anatomopathological examination showed chronic fibro-inflammatory non-specific skin changes and the presence of epithelio-giganto-cellular granuloma with caseous necrosis within the breast lesion. The diagnosis of tuberculosis mastitis with associated lymph node invasion was retained.
She underwent a 6-month course of anti-tuberculosis therapy of 2HRZE/4HR (2 months of Isoniazid, Rifampin, Pyrazinamide and Ethambutol followed by 4 months of Isoniazid and Ethambutol biotherapy). Despite difficulties with therapeutic compliance, she was cured of her mastitis tuberculosis after 6 months. The follow-up at one year was uneventful.


Discussion
According to the latest WHO report [8], TB is a global health problem that is the 13th leading cause of death and the second leading infectious killer after COVID-19 (above HIV/AIDS). Mammary tuberculosis is an extrapulmonary form of TB that was first described by Cooper et al. [9] in 1829 as a cold breast tumor. This location is very unusual and represents 0.06% of all tuberculosis locations and is the last visceral localization of TB [10]. It is an extrapulmonary localization of TB which mainly affects young women during their reproductive years as in our patient who was 39 years old [11]. This was also reported by Mehta G et al. [12] in a retrospective study of a series of 63 patients with mammary tuberculosis; 49.2% were under 30 years of age. According to his work, it is a disease that mainly affects women since almost all (98.41%) of their patients were female [12]. Pregnancy, lactation and multiparity are risk factors [11], which are explained by the galactophoric ectasia during lactation.
There are various routes of contamination [2]: The lymphatic route, where an axillary adenopathy is often found; the hematogenous route, in the context of a tubercular infection; propagation by contiguity from a neighbouring focus; the ductal route: The dilation of the galactophoric ducts in women during pregnancy or lactation increases the sensitivity of these ducts to bacillus infection; a direct route: exceptional, it is the penetration of Koch’s bacillus into the breast following a cutaneous or galactophoric abrasion. Classically, two types of tuberculosis are distinguished: Secondary tuberculosis with involvement of other organs and primary tuberculosis where the tuberculosis appears to be strictly localized to the breast, the latter is the most frequent [13,14]. In our patient the involvement was also primary.
Breast tuberculosis has non-specific and often misleading clinical manifestations. Its clinical features include centered erythematous lesions, a fluctuating abscess or a well-limited nodule [12]. It can also present as a tumor-like lesion without pain and purulent discharge [15], or as mastitis of the breast with nipple retraction and skin fistulas. This variety of clinical presentations makes it a very difficult diagnostic entity even in endemic areas [2]. However, several clinical criteria can point to TB [2]: the existence of recurrent abscesses resistant to antibiotics; the existence of fistulized axillary adenopathies and finally, breast fistula with nipple discharge.
Radiologically, there are no specific mammographic signs of breast tuberculosis [16,17], mammography may show irregular heterogeneous opacities, poorly limited, sometimes with calcifications, pointing to a malignant etiology. Breast tuberculosis ultrasound often appears as a hypoechoic, heterogeneous image, well or poorly limited with minimal posterior enhancement [18]. The diagnosis of certainty remains the histological or bacteriological examination [3,7,19]. In fact, demonstration of epithelioid and giganto-cellular granuloma with caseous necrosis is very specific of TB [3,7].
The main differential diagnosis to be feared in breast tuberculosis is breast cancer, other pathologies should be discussed, such as breast abscess, fibroadenoma, sarcoidosis and granulomatous mastitis. In our observation, in front of an inflammatory breast, the first diagnosis to be evoked is essentially breast cancer and only the histological examination allowed the diagnosis of tuberculosis mastitis.
The therapeutic management of breast tuberculosis is based on anti-bacillary medical therapy, with possible percutaneous drainage of a breast abscess, which was not the case in our patient. Surgery such as mastectomycan also be proposed in case of resistance to medical treatment [11].
Conclusion
Mammary extrapulmonary tuberculosis is uncommon and presents a difficult diagnostic challenge that requires a high degree of suspicion, especially in endemic areas. The clinical and radiological pictures are misleading, and raise a diagnostic problem especially with breast cancer. But it is only the histopathological or bacteriological examination that allows a diagnosis of certainty.
Declarations
Guarantor of submission: The corresponding author is the guarantor of submission.
Acknowledgements: None.
Funding: There are no funding sources to be declared.
Availability of data and materials: Supporting material is available if further analysis is needed.
Competing interests: The authors declare that they have no competing interests.
Consent for publication: Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethics approval and consent to participate: Ethics approval has been obtained to proceed with the current study. Written informed consent was obtained from the patient for participation in this publication.
References
- Agoda Koussema LK, Djibril AM, Adjenou KV, et al. Tuberculose mammaire: A propos d’un cas (Breast tuberculosis: a case report). Journal Africain d’Imagerie Médicale. 2014; 6.
- Ben Hassouna J, Gamoudi A, Bouzaïene H, et al. Tuberculose mammaire: étude rétrospective de 65 cas. Gynécologie Obstétrique et Fertilité. 2005; 33: 870-876.
- Sarah T, Slaoui A, Benzina I, et al. Primary Breast Tuberculosis. Surg Case Rep. 2020; 5: 5.
- Benmouna I, Slaoui A, Cherradi S, Lakhdar A, Zeraidi N, Baidada A, et al. Mixed mucinous carcinoma of breast - a case report. wjpmr, 2022; 8: 01-04.
- Benaouicha N, Slaoui A, Louzali FZ, Zeraidi N, Lakhdar A, et al. Phyllodes Carcinoma of the Breast: An Uncommon Case Report. Sch Int J Obstet Gynec. 2022; 5: 201-204.
- Benmouna I, Mouimen S, Slaoui A, Baydada A. Intracystic papillary carcinoma of the breast: Report case and literature review. International Journal of Frontiers in Science and Technology Research. 2022; 02: 019–023.
- Slaoui A, Cherkaoui N, El Harmouchi O, et al. Fortuitous discovery of ganglionic tuberculosis after conservative treatment of breast cancer: a case report and review of the literature. BMC Womens Health. 2019; 19: 79.
- Global tuberculosis report 2021. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO.
- Cooper A. Illustration of the diseases of the breast, London. 1928.
- Khair M, El Hafidy K, Ghalloudi A. La tuberculose mammaire à propos de trois cas. Espérance médicale A. 2010 ; 17: 498-501.
- Hawilo A, Abdelmalek R, Mebazaa A, Addouni O, Kanoun F, et al. Tuberculosis of the breast: A rare often unrecognized diagnosis. Med Sante Trop. 2012; 22: 292-296.
- MehtaG, Mittal A, Verma S. Breast tuberculosis clinical spectrum and management. Indian J Surg. 2010; 72: 433-437.
- Marinopoulos Spyridon, Lourantou Dionysia, Gatzionis Thomas, et al. Breast tuberculosis: diagnosis, management and treatment. International journal of surgery case reports. 2012; 3: 548-550.
- Gulpinar Kamil, Ozis S Erpulat, Ozdemir Suleyman, et al. Primary breast tuberculosis: Report of a case. Surgical Science. 2013; 4: 68-71.
- Seker D, Kaya O, Seker G E. Tuberculosis of the Breast: Medical Treatment Actachirurgica Belgica A. 2010; 614-615.
- Morsad F, Ghazli M, Boumzgou K, Abbassi H, El Kerroumi M, et al. Tuberculose mammaire: A propos de 14 cas. J Gynecol Obstet Biol Reprod. 2000; 30: 331-333.
- Filippou Dimitrios C, Rizos Spiros, et al. Nissiotis, Athanasios. Primary breast tuberculosis: A case report. Radiology and Oncology. 2003; 37.