
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Intrabronchial haemorrhage – the bronchoscopist’s nightmare: A case of major haemoptysis due to pulmonary Dieulafoy’s disease
Tiziana Locatelli1; Tino Schneider1; Thorsten Ottilinger2; Martin H Brutsche1*
1Lung Center, St. Gallen Cantonal Hospital, 9007 St. Gallen, Switzerland.
2Division of Radiology and Nuclear Medicine, St. Gallen Cantonal Hospital, 9007, St. Gallen, Switzerland.
*Corresponding Author : Martin H Brutsche
Lung Center, Canton Hospital St. Gallen, Rorschacherstrasse 95, 9007 St. Gallen, Switzerland.
Tel: 0041714941004;
Email: martin.brutsche@kssg.ch
Received : Sep 03, 2022
Accepted : Sep 29, 2022
Published : Oct 06, 2022
Archived : www.jcimcr.org
Copyright : © Brutsche MH (2022).
Abstract
Massive haemoptysis is a term used to describe a large amount of expectorated blood or rapid rate of bleeding (>100 ml blood in 24 h) and is associated with a serious risk of death. However, there is no clear consensus on its definition [1]. In the present we report the case of a 39-year-old male, investigated for haemoptysis, quickly turning bad during diagnostic flexible bronchoscopy due to a rare condition. The congenital abnormality with displaced right upper lobe segmental bronchus and lack of the apical segment bronchus of the right lower lobetogether with the endoscopic narrow-band imaging were the diagnostic clues for the presence of pulmonary Dieulafoy‘s disease and angiographic glue embolization (n-butyl-2-cyanoacrylate) the treatment of choice.
Keywords: Pulmonary haemorrhage; Major haemoptysis; Narrow-band imaging; Dieulafoy’s disease.
Citation: Locatelli T, Schneider T, Ottilinger T, Brutsche MH. Intrabronchial haemorrhage – the bronchoscopist’s nightmare: A case of major haemoptysis due to pulmonary Dieulafoy’s disease. J Clin Images Med Case Rep. 2022; 3(10): 2089.
Case report
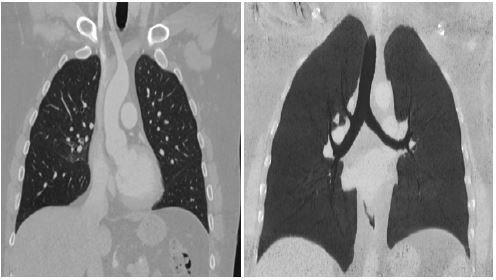
A 39-year-old smoker (5 pack-years) presented in a good general condition with symptoms of a common cold. Within days his cough – at first dry – turned into a productive cough with sputum contaminated with streaks of blood. His physical examination and history did not reveal other health issues nor pre-existing comorbidities. The lab came back normal apart from a slight anaemia (haemoglobin 123 g/L) and the C-reactive protein was slightly elevated. The nasal smear for influenza and two blood cultures were negative and the chest X-ray was normal. Due to the unexplained anaemia in the context of haemoptysis a contrast-enhanced CT of the thorax was performed, which showed alveolar infiltrates in the basal portion of the right upper lobe and discretely in the right lower lobe. The findings were compatible with pulmonary haemorrhage without signs of an active haemorrhage (Figure 1A). The CT also showed a congenital bronchial abnormality with preeparterial displacement of the apical branch of the right upper lobar bronchus arising from the right main bronchus and additionally fusion of the middle and right lower lobar bronchus with lack of the bronchus intermedius and the horizontal interlobar fissure, mimicking a left isomerism (Figure 1B). Faced with a potentially major haemoptysis inhaled tranexamic acid and a codeine-based antitussive was prescribed and the patient was admitted to the Lung Center for surveillance and follow-up.
In order to rule out malignancy or TB and to localize the origin of the haemorrhage a flexible bronchoscopy was performed. It showed some sequelae of haemorrhage in the right bronchial tree, but no active haemorrhage. The tracheal bronchus and the lack of the apical segment bronchus of the right lower lobe, as described on the CT, were confirmed. At the upper lobe and middle lobe bronchus with a common outlet, a nodular lesion of the bronchial mucosa was identified (Figure 2). This lesion seemed compatible with a carcinoid, another benign tumor or blood vessel abnormality. To better characterize the vascularity of the described lesion narrow-band imaging was applied, but in the opinion of the endoscopic team could not identify larger blood vessels or dysmorphic endomucosalangioneogenesis (Figure 2). Finally, an endobronchial mucosal biopsy was taken.

The first endobronchial forceps biopsy resulted in an immediate and major endobronchial haemorrhage clarifying the origin of the haemorrhage, but stressing the whole bronchoscopy team. Fortunately, the haemorrhage stopped after instillation of cold isotonic saline and three endobronchial applications of 0.5 mcg adrenaline. Endotracheal intubation or further endoscopic interventions were not necessary. However, the patient was transferred to the intensive care unit for haemodynamic and respiratory surveillance. The final diagnosis of bronchial Dieulafoy’s disease of the intermediate bronchus was retained and later confirmed histologically. The microbiology of the bronchial aspirate showed upper airway flora, the PCR for M. tuberculosis was negative, and the cytology of aspirated secretion showed no malignant cells.
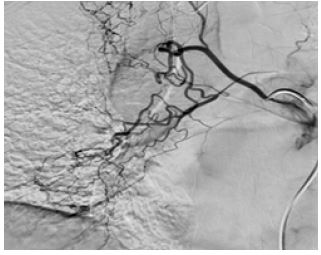
According to an interdisciplinary treatment decision an angiography was performed (Figure 3) with glue embolization (n-butyl-2-cyanoacrylate) of the right bronchial artery at the level of the middle and lower lobe. A repeat bronchoscopy documented no active bleeding and an irritation-free mucosal lesion of the intermediate bronchus at the site of the Dieulafoy’ lesion. The patient was discharged and no further haemoptysis occurred since.
Discussion
Dieulafoy’s disease was first described in 1898 by the French surgeon George Dieulafoy as a cause of bleeding in the stomach. It was defined as a vascular abnormality characterised by the presence of a dysplastic tortuous artery in the submucosa, from which vascular branches may be located in the mucosa [2]. The disease commonly appears in the digestive tract. Besides causing bleeding in the stomach, this malformation has been described in other organs of the gastrointestinal tract: oesophagus, duodenum, gall bladder, jejunum, colon and rectum [3]. Dieulafoy’s disease can occur, but has rarely been reported with bronchial localisation [4]. Dieulafoy’s disease of the bronchus was first described by Sweerts et al [2] in 1995, and to date, approximatively 100 cases have been reported worldwide. However, as the condition is under-recognized and frequently underdiagnosed, the actual incidence is likely to be higher [16]. In the largest series 74 cases of bronchial Dieulafoy’s disease have been identified in the past 20 years since the first reported case in 1995 [17-19]. The aetiology remains uncertain. Most researchers believe that the disease is congenital, while others believe that it can be acquired or is simply an abnormality of normal blood vessels [17,18,20]. However, an association with congenital organ and vascular dysplasia is postulated–as seen in our current case. Vascular dysplasia can originate from the systemic or pulmonary circulation [5]. Patients with lesions in the right bronchus account for approximately two-thirds of the reported cases [16].
It is thought that the tortuous artery in the submucosa causes erosive pressure on the mucosa with rupture of the vascular wall, frequently followed by severe, potentially life-threating bleeding. Several factors can cause haemoptysis in endobronchial Dieulafoy’ disease. In our case a mild haemoptysis occurring during an upper airway infection with cough turned into a massive haemoptysis by a single pass of endobronchial forceps biopsy. Haemoptysis was also reported after bronchoscopic washings by others [7,9,12]. A positive history of respiratory diseases [7,8,12,14] such as tuberculosis, bronchiectases, chronic bronchitis and frequent pneumonia and tobacco habit may contribute to spontaneous fatal haemoptysis [3,5,6,8]. Dieulafoy’ disease should also be suspected in heavy smokers with recurring and unexplained episode of massive hemomptysis. Haemoptysis often presents with non-typical symptoms such as cough, recurrent massive haemoptysis, chest discomfort, symptoms or signs of hypovolemia [7].
In Dieulafoy’s disease of the bronchus, chest X-rays and Computed Tomography (CT) scans of the thorax rarely result in findings other than the manifestation of an intrapulmonary haemorrhage and the original lung disease [21]. The possibility of Dieulafoy’s disease of the bronchus should be considered in patients with haemoptysis when chest X-ray and CT examinations demonstrate no obvious abnormalities other than pulmonary haemorrhage [16]. Multi-slice CT angiography of the bronchial or pulmonary artery can visualize an abnormal bronchial artery associated with tortuosity and dilation [22], and sometimes detects well-enhanced endobronchial nodules [23]. Lesions with >100 Hounsfield Units are indicative for a vascular lesion [16]. Angiography is useful to diagnose bronchial Dieulafoys’ disease and to detect the source of the abnormal vessels (e.g. bronchial vs. pulmonary arteries), although there are no specific criteria to confirm it [15]. Additionally, vascular malformations, based on a left-right shunt, with a bronchial artery draining into a pulmonary artery, can be identified [8-11].
Bronchoscopy demonstrates differend grades of endobronchial haemorrhage, which may be accompanied by blood clot formation [24,25]. Mucosal nodular projections can be a few millimetres in diameter and height with a smooth surface [24]. The lesion may also be congested and rough, with slight vascular pulsation in specific cases. Sometimes the protruding surface is coated with yellow-white exudate forming a ‘little white hat’-like shape, easily misdiagnosed as an endobronchial tumour nodule [26]. When convex probe EBUS is used to detect blood flow within a lesion, it often shows a fluid echo-free zone in submucosal lesions. The blood flow can be displayed in the colour or energy Doppler mode [26]. Owing to its large diameter, convex probe EBUS cannot reach the upper lobe bronchus or segmental bronchus. Alternatively, radial probe EBUS can be used to examine the lesion. However, the latter approach has no Doppler mode and, thus, cannot determine blood flow within the lesion. Nonetheless, radial probe EBUS can indicate an echo-free zone, which may be considered for vascular lesions in patients with haemoptysis. Alternatively, during bronchoscopy narrow-band imaging can help to identify the vascular nature of the lesion. Narrow Band Imaging (NBI) can display endobronchial lesions such as bronchial artery-pulmonary artery fistulae. However, there have been no studies to assess the diagnostic value of NBI in Dieulafoy’s disease [16]. If Dieulafoy’s disease of the bronchus is misdiagnosed as benign submucosal lesions under bronchoscopy, biopsy may be taken and results in potentially lethal bleeding. It is, therefore, recommended to either perform EBUS or NBI before taking bronchial biopsies in case of suspicion.
Currently, there is no consensus for the treatment of Dieulafoy’s lesion of the bronchus. The treatment strategy depends on the clinical presentation, the site of the lesion and medical expertise available [8-11]. The currently used treatment modalities include selective bronchial artery embolization (SBAE), pulmonary lobectomy and argon plasma coagulation via bronchoscopy. Currently, SBAE is the preferred approach, and lobectomy of the diseased lobe is used following embolization failure or recurrent post-embolization haemoptysis [16]. Topical application of haemostatic drugs, superficial haemostasis by dotted electrocoagulation, argon-beam-coagulation, Nd:YAG-laser treatment and freezing under bronchoscopy are affected by a poor haemostatic efficacy. Bronchoscopy can help to clarify the bleeding site, there by determining the target zone for bronchial angiography or surgery.
Arterial embolization reduces the need for surgery and is obviously advantageous for patients who cannot tolerate major surgery. A previous review by Fang et al. reported that selective bronchial artery embolization was performed in a cohort of 17 patients [6]. Reasons contributing to failure of bronchial artery embolization are 1) abnormal vessels arising from the pulmonary circulation rather than the systemic circulation [7], 2) revascularisation and neovascularisation that can cause recurrences of haemoptysis after embolization [6] and 3) secondary coil migration may cause failure of an initially successful embolization. Therefore, it is highly recommended to locate and follow up the bronchial lesions and their feeding vessels as precisely as possible with bronchoscopy in combination with angiography [6]. In some cases, surgical resection is necessary and might be indicated in some cases when the abnormal vessel arises from pulmonary circulation and embolization fails [13].
A lobectomy may be necessary if recurrent haemoptysis occurs after an embolization and when the follow-up arterial angiography suggests revascularization and a neovascularization in the same lobe [8]. If a malignant tumour is responsible for the angiodysplastic lesion and haemorrhage surgical resection needs to be performed with a safe margin [3]. Angiographic embolization is the method of choice in inoperable or unresectable tumour cases.
In the Lung Center St. Gallen, we have seen a total of 4 cases in the last 15 years or 15,000 bronchoscopies - this corresponds to an incidence of 0.3 cases per 1000 bronchoscopies. All of them had a bronchoscopy for haemoptysis and a “harmless” looking mucosal lesion without malignancy criteria. Only one case of them had congenital abnormality (tracheal bronchus).
Conclusion
Although bronchoscopy is a reliable and safe method for the work-up of endobronchial haemorrhage and, to a certain extent, for distinguishing Dieulafoy’s lesion from malignant tumours and other benign lesions, the intent of our case report is to remind the bronchoscopist to be careful and cautious when examining haemoptysis and to avoid biopsy when Dieulafoy’s disease is suspected. The case described above and the literature reviewed, indicates, that in case of haemoptysis and a harmless mucosal lesion, an NBI or EBUS should first be performed before performing a biopsy. In case of doubt, it is indicated to abstain from any biopsy but to perform interventional angiography. In retrospect the congenital abnormality with tracheal bronchus and missing bronchus of the apical segment together with the endoscopic narrow-band imaging were the clues for the presence of Dieulafoy‘s disease in our case.
References
- Christopher Radchenko, Abdul Hamid Alraiyes, Samira Shojaee, A systematic approach to the management of massive hemoptysis, J Thorac Dis. 2017; 9: S1069–S1086.
- Kuzucu A, Gurses I, Soysal O. Dieulafoy’s disease: A cause of massive hemoptysis that is probably underdiagnosed. Ann Thorac Surg. 2005; 80: 1126-1128.
- Stoopen E, Baquera-Heredia J, Cortes D, Green L, et al. Dieulafoy’s disease of bronchus in association with a paravertebral neurilemma. Chest. 2001; 119: 292-294.
- Chen W, Chen P, Li X. Clinical characteristics and treatments for bronchial Dieulafoy’s disease. Respir Med Case Rep. 2019; 26: 229-235.
- Sweerts M, Nicholson AG, Goldstraw P, Corrin BM, et al. Dieulafoy’s disease of the bronchus. Thorax. 1995; 50: 697–698.
- Fang Y, Wu Q, Wang B. Dieulafoy’s disease of the bronchus. Report of a case and review of the literature. J Cardiothorac Surg. 2014; 9: 191.
- Van der Werf TS, Timmer A, Zijlstra JG. Fatal haemorrhage from Dieulafoy’s disease of the bronchus. Thorax. 1999; 54: 184-185.
- Bhatia P, Hendy MS, Li Kam Wa E, Bowyer PK. Recurrent embolotherapy in Dieulafoy’s disease of the bronchus. Can Respir J. 2003; 10: 331-333.
- Loschhorn C, Nierhoff N, Mayer R, Zaunbauer W, Neuweiler J, Knoblauch A, et al. Dieulafoy’s disease of the lung. A potential disaster for the bronchoscopist. Respiration. 2006; 73: 562-565.
- Kolb T, Gilbert C, Fishman EK, Terry P, Pearse D, et al. Dieulafoy’s disease of the bronchus. Am J Respir Crit Care Med. 2012; 186: 1191-10.1164/rccm.201206-1016IM.
- Barisione EE, Ferretti GG, Ravera SS, Salio MM, et al. Dieulafoy’s disease of the bronchus: A possible mistake. Multidiscip Respir Med. 2012; 7: 40-10.1186/2049-6958-7-40.
- Maxeiner H. Lethal hemoptysis caused by biopsy injury of an abnormal bronchial artery. Chest. 2001; 119: 1612-1615. 10.1378/chest.119.5.1612
- Pomplun A, Sheaff TM. Dieulafoy’s diease of the bronchus: An uncommon entity. Histopathology. 2005; 43: 587-599.
- D’Souza F, Sharma R. Dieulafoy’s disease of the bronchus. Pathology. 2010; 42: 683-684.
- Xie BS, Chen YS, Lin MF, Huang QH, Lin ZS, et al. [Dieulafoy’s disease of the bronchus: A case report and review of the literature]. Zhonghua Jie He He Hu Xi Za Zhi. 2006; 29: 801-803.
- Xiqian Xing, Jei Liu, Shuanglan Xu, Yishu Dendgu and Jiao Yang, et al. Research advances in Dieulafoy’s disease of the bronchus (Rewiew), Experimental and therapeutic medicine. 2022; 23: 100.
- Sweerts M, Nicholson AG, Goldstraw P and Corrin B, et al. Dieulafoy’s disease of the bronchus. Thorax. 1995; 50: 697–698.
- Smith B, Hart D and Alam N. Dieulafoy’s disease of the bronchus: A rare cause of massive hemoptysis. Respirol Case Rep. 2014; 2: 55–56.
- Fields EL and De Keratry DR. Dieulafoy disease of the bronchus. Case report and presentation of a novel therapeutic modality. J Bronchology Interv Pulmonol. 2008; 15: 107–109.
- Barisione EE, Ferretti GG, Ravera SS and Salio MM. Dieulafoy’s disease of the bronchus: A possible mistake. Multidiscip Respir Med. 2012; 7.
- Stoopen E, Baquera Heredia J, Cortes D and Green L, et al. Dieulafoy’s disease of the bronchus in association with a paravertebral neurilemoma. Chest. 2001; 119: 292–294.
- Kolb T, Gilbert C, Fishman EK, Terry P, Pearse D, Feller-Kopman D, et al. Dieulafoy’s disease of the bronchus. Am J Respir Crit Care Med. 2012; 186.
- Xie BS, Chen YS, Lin MF, Huang QH and Lin ZS, et al. Dieulafoy’s disease of the bronchus: A case report and review of the literature. Zhonghua Jie He He Hu Xi Za Zhi. 2006; 29: 801–803.
- Pan F, Wang F, Liu Z, Yuan F, Sun KK, et al. The computed tomography angiography features of Dieulafoy disease of the bronchu]. Zhonghua Jie He He Hu Xi Za Zhi. 2018; 41: 949–953.
- Chen W, Chen P, Li X, Gao X and Li J, et al. Clinical characteristics and treatments for bronchial Dieulafoy’s disease. RespirMed Case Rep. 2019; 26: 229–235.
- Parrot A, Antoine M, Khalil A, Théodore J, Mangiapan G, et al. Approach to diagnosis and pathological examination in bronchial Dieulafoy disease: A case series. Respir Res. 2008; 9.
- Gurioli C, Casoni GL, Gurioli C, Tomassetti S, Romagnoli M, et al. Endobronchial ultrasound in Dieulafoy’s disease of the bronchus. An additional application of EBUS. Monaldi Arch Chest Dis. 2010; 73: 166–168.