
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Unusual pediatric pleural effusions: A case
series and a review of the literature
Tommaso Bellini1*; Matteo D’alessandro1; Luca Basso2; Benedetta Chianucci1,3; Margherita Ricci1,3; Maria Beatrice Damasio2; Emanuela Piccotti1
1Pediatric Emergency Room and Emergency Medicine Unit, Gaslini Children Hospital, IRCCS Istituto Giannina Gaslini, Genoa, Italy.
2Radiology Unit, Gaslini Children Hospital, IRCCS Istituto Giannina Gaslini, Genoa, Italy.
3Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health (DINOGMI), University of Genoa, Genoa, Italy.
*Corresponding Author : Tommaso Bellini
Pediatric Emergency Room and Emergency Medicine Unit, Gaslini Children Hospital, IRCCS Istituto Giannina Gaslini, 16147 Genoa, Italy.
Tel: 0039-010-56363853;
Email: tommasobellini@gaslini.org
Received : Sep 03, 2022
Accepted : Sep 30, 2022
Published : Oct 07, 2022
Archived : www.jcimcr.org
Copyright : © Bellini T (2022).
Abstract
Point-of-care ultrasound is an effective tool for pediatric emergency physicians in addition to the physical examination for respiratory failure and suspected pleural effusion. We present a series of three unusual cases where point-of-care ultrasound was crucial as first diagnostic tool to identify pleural effusion and to allow further therapeutic choices.
Keywords: POCUS; Pleural effusion; Emergency medicine; Ultrasound.
Citation: Bellini T, D’alessandro M, Basso L, Chianucci B, Ricci M, et al. Unusual pediatric pleural effusions: A case series and a review of the literature. J Clin Images Med Case Rep. 2022; 3(10): 2091.
Background
Lung Point-Of-Care Ultrasound (POCUS) is an important diagnostic tool to detect pleural effusion and its use in the Pediatric Emergency Departments (PEDs) is increasing. Thanks to its high sensitivity and specificity and its safety profile, POCUS should be considered as an extension of the physical exam and should be the first line procedure to guide the choice of further diagnostic-therapeutic procedures [1-4]. In this case series we have presented three unusual etiologies of pleural effusion and suggested that POCUS together with careful clinical evaluation and a low threshold of suspicion can improve the management of dyspnoic patients in PED; being repeatable and comparable, ultrasound also allows for a real-time follow-up and a reduction in the radiation dose received due to a decrease in the number of chest radiographs performed [3,6,7].
Here we report three unusual cases of pleural effusion in which POCUS played a key role in diagnosis and management. Local ethical board committee approved and permitted the use of patients images.
Cases presentation
Case 1: A 8-year-old girl affected by Congenital Myotonic Dystrophy was admitted to our third-level PED due to respiratory failure. She was usually assisted with nocturnal Pressure Support Mechanical Ventilation (PSV) via tracheostomy; the morning of admission, upon awakening, her parents noticed an increased respiratory effort which prevented daytime suspension of PSV. At presentation she was assisted by PSV; she was alert, sweaty, tachycardic and pale, with low-grade fever and normal oxygen saturation in room air. During examination she presented two desaturation < 50% episodes, resolved after as piration of abundant blood-mixed mucus from airways. Lungs auscultation showed silent right middle-lower lobes. The remaining physical examination was unremarkable.
We performed a lung POCUS, with the patient in the supine position, finding a large right pleural effusion with hepatization of the underlying lung parenchyma (Figure 1).
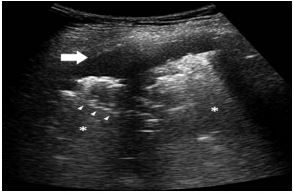
The father reported that, four days before, he noticed blood during the upper airways routine aspiration inducing us to suspect that she could have inhalated a tooth, confirmed by Computed Tomography (CT) scan.
The pleural effusion was drained with a POCUS-assisted thoracetesis and two fibroscopies were subsequently attempted to remove the Foreign Body (FB), both unsuccessfully. A lobectomy was performed but the patient died due to cardiopulmonary arrest 18 days after the surgical procedure.
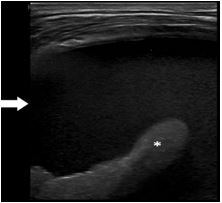
Case 2: A 13-year-old otherwise healthy girl presented to the PED with a one-month history of dry cough and breathing shortness with no other symptoms and no improvement despite broad spectrum antibiotics. Her past medical history was unremarkable. She was eupnoic and apyretic with normal heart rate and slight respiratory distress. Physical examination revealed a silent right chest.
We performed a lung POCUS, with the patient in the sitting position, finding an extensive right anechoic pleural effusion with underlying atelectatic lung (Figure 2). There were no ultrasound signs of pericardial effusion. Routine blood tests were not useful to clarify the origin of pleural effusion, with normal white blood cell count and inflammation markers. Due to the unclear origin of the effusion, a chest CT was performed, showing a right paramedian mediastinal hypodense solid mass.
Her bone marrow aspirate demonstrated a 90% blasts infiltration and a diagnosis of T-cell Acute Lymphoblastic Leukemia (T-ALL) was made. The pleural effusion was successfully drained.
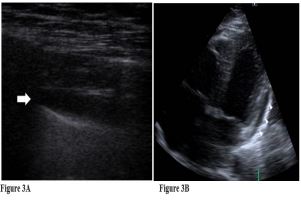
Case 3: A 16-year-old otherwise healthy boy presented to the PED with a 4-days history of persistent fever, chest pain and painful breathing. His past medical history was unremarkable except for Coronavirus Disease (COVID-19) twenty days before admission. At presentation he was suffering, alert and pale. He was tachycardic, tachypnoic and hypotensive. Cardiac activity was rhythmic, with muffled heart tones and ejective systolic murmur. Breath was bilaterally reduced at lung bases.
With the patient in the supine position, we performed lung POCUS and a subxiphoid chamber view Focus Cardiac Ultrasound (FOCUS), finding a pericardial effusion with preserved biventricular function and slight bilateral anechoic pleural effusion with sporadic B-lines (Figures 3A,3B).
Blood tests were consistent with a hyperinflammatory state; thus a diagnosis of COVID-related Multisystem Inflammatory Syndrome (MIS-C) was made. Pulses of methyl-prednisolone in association with anti-interleukin-1 therapy were started with progressive clinical and ultrasound improvement.
Discussion and literature review
Our Lung POCUS and FOCUS were performed by two PED physicians previously trained in basic and advanced US education with at least 2 years of PED and US experience.
Usually, if the patient is conscious and cooperative, an upright position is preferred for a suspected pleural effusion, although sometimes it may not be applicable due to trauma, altered level of consciousness or neuromuscular pathologies that force the patient to maintain a supine or a 45° position as our case 1; thus, it is mandatory to explore the most caudal area of the thoracic cavity because free-flowing pleural effusions accumulate in the most dependent portions of the thorax [1,2]. The type and frequency of transducer used should vary with the age of the patient; high frequency linear probe (5–10 MHz) with a small footprint are preferred in younger patients as our case 1, whereas in older or obese patients where a greater depth is required, a low frequency convex probe (2–5 MHz) is preferred, as our case 2 and 3 [3-5].
As shown in case1, FB Inhalation (IFB) is a critical occurrence in children, especially under three years of age and in those with neurological disabilities, due to uncoordinated swallowing or others anomalies of the protective mechanisms of the airways [8].
There are no specific clinical or radiological diagnostic criteria; antero-posterior chest radiographs are traditionally used although there are no sure signs and a substantial proportion of cases may have silent radiographs. In this case, the POCUS together with a careful medical history and clinical examination has allowed us to diagnose a IFB at patient’s bed. It is known that the longer a FB remains in the airways, the more difficult endoscopic removal will be, due to mucosal inflammation and edema, therefore timely diagnosis is very important. Although IFB secondary to trauma is known, to our knowledge this is the first reported case of dental inhalation secondary to traumatic airway aspiration [9].
As reported in the literature, pleural effusion could be the first sign of malignant disease as a result of various mechanisms, including lymphatic/venous obstruction due to mediastinal lymph nodes, mediastinal masses or thoracic duct obstruction or pleuropulmonary infiltration/superinfection [10]. Certainly, US findings are not specific and need always to be related to other clinical and laboratory data with a cytological or histological confirm, although our case2 point out the necessity for considering the T-cell lymphoblastic lymphoma and T-ALL within the differential diagnosis of any sterile pleural effusion with no response to antimicrobial therapy and POCUS could be a formidable tool for an early diagnosis.
Finally, the incidence of pleural effusion in MIS-C is debated; the few data reported are conflicting. Some authors have reported rare pulmonary involvement in MIS-C, unlike COVID-19, but other authors have suggested how bilateral B-lines and pleural effusions may help PED physicians to recognize systemic inflammatory disease, given the absence of effusion in acute SARS-CoV-2 infection [11]. Our case 3 revealed how a bilateral pleural effusion combined with a pericardial effusion can suggest an inflammatory etiology and therefore lead to targeted therapy; moreover, POCUS has the indisputable advantages to explore at first sight the multi-organ involvement typical of MIS-C and the possibility of being repeated to verify the effects of the therapeutic management [12]
While there is no doubt about the superiority of POCUS over physical exam and chest radiography to detect pleural fluid, there is no agreement on its usefulness for the differential diagnosis between transudate and exudates, where POCUS shows its main limit [2]. A transudate pleural effusion is always anechoic but exudates, both malignant and non-malignant, may be anechoic or echogenic, with or without fibrinous septations; therefore, while an echogenic effusion may suggest an exudate, an anechoic pleural effusion does not provide diagnostic evidence of a transudate and should not remove concern that the effusion may be exudative [13,14]. In these cases, if the etiology remains unclear, thoracentesis is needed to establish a diagnosis and POCUS can be useful facilitating this invasive procedure reducing complications and increasing its success rate as shown in case 1.
Conclusion
During the acute phase, these described cases are usually admitted to the PED, but the etiological diagnosis remains difficult. Ultrasound is superior to radiography and physical examination in diagnosing pleural effusion, with results similar to CT scans, then offering the benefits of reduced cost, avoidance of ionizing radiation, and bedside availability [15].
Our case series highlights the heterogeneous etiologies of pleural effusion and suggests that POCUS is a key tool in unusual and emerging diseases; therefore, it should always be considered in any unclear case of dyspnea or respiratory failure to choose wisely which patients need further study such as CT or thoracentesis.
Declarations
Conflicts of interest: The authors have no relevant financial or non-financial interests to disclose.
Funding: The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
ORCID: Tommaso Bellini, https://orcid.org/0000-0001-7559-0111; Matteo D’Alessandro, https://orcid.org/0000-0003-0301-5753; Luca Basso, https://orcid.org/0000-0003-0289-8283; Benedetta Chianucci, https://orcid.org/0000-0001-8607-4200; Margherita Ricci, https://orcid.org/0000-0003-4949-5967; Maria Beatrice Damasio, https://orcid.org/0000-0001-6737-1090; Emanuela Piccotti, https://orcid.org/0000-0002-1569-0222.
References
- Weerdenburg KD, Kwan CW, Fischer JW. Point-Of-Care Ultrasound Findings Associated With Foreign Body Aspiration in the Pediatric Emergency Department. Pediatr Emerg Care. 2016; 32: 486-48s8.
- Beers SL, Abramo TJ. Pleural effusions. Pediatr Emerg Care. 2007; 23: 330-334.
- Joshi P, Vasishta A, Gupta M. Ultrasound of the pediatric chest. Br J Radiol. 2019; 92: 20190058.
- Wimalasena Y, Kocierz L, Strong D, et al. Lung ultrasound: A useful tool in the assessment of the dyspnoeic patient in the emergency department. Fact or fiction? Emerg Med J. 2018; 35: 258-266.
- Gardecki J, Patel K, Rowshan O. Scan the lung: Point-of-care ultrasound of a pulmonary consolidation with loculated pleural effusion. Am J Emerg Med. 2019; 37: 377.e1-377.e3.
- Singh Y, Tissot C, Fraga MV, et al. International evidence-based guidelines on Point of Care Ultrasound (POCUS) for critically ill neonates and children issued by the POCUS Working Group of the European Society of Paediatric and Neonatal Intensive Care (ESPNIC). Crit Care. 2020; 24: 65.
- Le Coz J, Orlandini S, Titomanlio L, et al. Point of care ultrasonography in the pediatric emergency department. Ital J Pediatr. 2018; 44: 87.
- Antón-Pacheco JL, Martín-Alelú R, López M, et al. Foreign body aspiration in children: Treatment timing and related complications. Int J Pediatr Otorhinolaryngol. 2021; 144: 110690.
- Madan K, Aggarwal AN, Bhagat H, et al. Acute respiratory failure following traumatic tooth aspiration. BMJ Case Rep. 2013; 2013: bcr2012008393.
- McCarten KM, Metzger ML, Drachtman RA, et al. Significance of pleural effusion at diagnosis in pediatric Hodgkin lymphoma: a report from Children’s Oncology Group protocol AHOD0031. Pediatr Radiol. 2018; 48: 1736-1744.
- Musolino AM, Boccuzzi E, Buonsenso D, et al. The Role of Lung Ultrasound in Diagnosing COVID-19-Related Multisystemic Inflammatory Disease: A Preliminary Experience. J Clin Med. 2022; 11: 234.
- Delmonaco AG, Carpino A, Raffaldi I, et al. First diagnosis of multisystem inflammatory syndrome in children (MIS-C): an analysis of PoCUS findings in the ED. Ultrasound J. 2021; 13: 41.
- Shkolnik B, Judson MA, Austin A, et al. Diagnostic Accuracy of Thoracic Ultrasonography to Differentiate Transudative From Exudative Pleural Effusion. Chest. 2020; 158: 692-697.
- Evans PT, Zhang RS, Cao Y, et al. The Use of Thoracic Ultrasound to Predict Transudative and Exudative Pleural Effusion. POCUS Journal. 6: 97–102.
- Brogi E, Gargani L, Bignami E, et al. Thoracic ultrasound for pleural effusion in the intensive care unit: A narrative review from diagnosis to treatment. Crit Care. 2017; 21: 325.