
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Moyamoya disease incidentally discovered in head trauma
Amal Lahfidi*; Wend-Yam Mohamed Traore; Onka Benyamet; Amina El khamlichi, Firdaous Touarsa; Najoua Ech-cherif El Kettani; Mohamed Jiddane; Meriem Fikri
Department of Neuroradiology, UHC Ibn Sina Rabat, Faculté de Médicine et de Pharmacie,Université Mohammed V, Rabat-Maroc.
*Corresponding Author : Lahfidi Amal
Département de neuro-radiologie, Centre hospitalieruniversitaire Ibn Sina, Rabat-Morocco.
Ph: +21-2610554872;
Email: lahfidial@gmail.com
Received : Sep 09, 2022
Accepted : Oct 05, 2022
Published : Oct 12, 2022
Archived : www.jcimcr.org
Copyright : © Amal L (2022).
Abstract
Moyamoya disease is a chronic cerebral vascular disease of undetermined origin, characterized by stenosis and progressive occlusion of the distal portion of the internal carotid arteries and the proximal portion of the middle and anterior cerebral arteries with resulting, abnormal vascular network development at the base of the skull, realizing a smoke volute appearance or moyamoya. The disease is most common in East Asia. It has two peaks of incidence: around the age of 05 years and during the 4th decade with a female predominance. In children, it leads more frequently to repeated ischemic strokes, while in adults, cerebral hemorrhages are observed. Cerebral MRI and arteriography are the imaging modalities allowing the positive diagnosis of the disease as well as the planning of the management which is based on a revascularization surgery which must be indicated at the optimal period during the follow-up of the disease.
Keywords: Head trauma; Cerebral hemorrhage; Ischemic stroke; Moyamoya; MRI.
Citation: Lahfidi A, Traore WYM, Benyamet O, Khamlichi AE, Touarsa F, et al. Moyamoya disease incidentally discovered in head trauma. J Clin Images Med Case Rep. 2022; 3(10): 2098.
Introduction
Moyamoya disease is a chronic cerebral vascular disease of undetermined origin derived from the Japanese language, characterized by stenosis and progressive occlusion of the distal portion of the internal carotid arteries and the proximal portion of the middle and anterior cerebral arteries with resulting, abnormal vascular network development at the base of the skull, realizing a smoke volute appearance or moyamoya.
It leads more frequently to repeated ischemic strokes, cerebral hemorrhages are observed. Cerebral MRI and arteriography are the imaging modalities allowing the positive diagnosis of the disease.
Clinical observation
A 62-year-old man, with no medical or surgical history, was involved in a traffic accident resulting in head trauma. He was immediately taken to the emergency room, where the initial clinical evaluation revealed a confused patient with a GCS of 14/15 without any sensory-motor deficit. Blood pressure was 157/95 mmhg with a heart rate of 115 beats per minute. Respiratory function was preserved with a respiratory rate of 18 cycles/min and room air saturation of 99%. The examination of the other devices was normal.
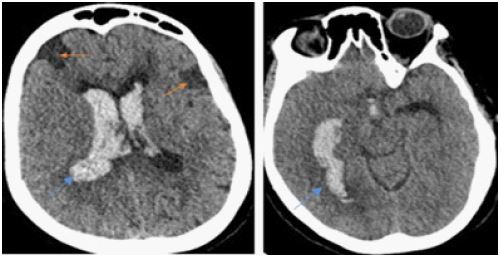
An emergency cerebral CT scan revealed a subarachnoid hemorrhage with ventricular inundation (Figure 1). No bone fracture was found, however, there was a widening of the cortical fissures as well as clearly hypodense areas suggesting sequels of previous ischemic episodes.
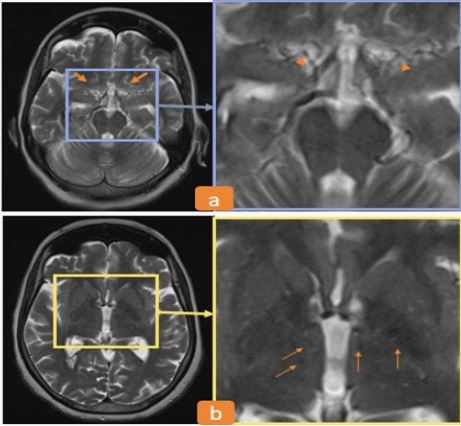
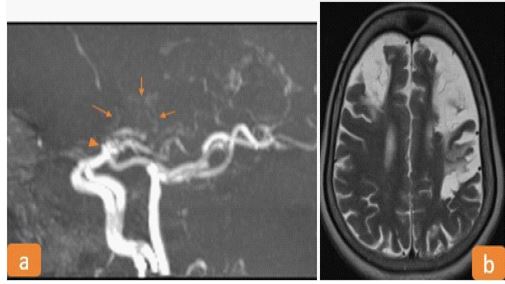
In order to detect and characterize eventual pre-existing vascular lesions, a cerebral CT angiography was performed. It did not reveal any abnormality, so a cerebral MRI was indicated as a delayed emergency. The angiographic sequences showed stenosis of the distal part of the internal carotid arteries as well as the proximal part of the anterior and middle cerebral arteries associated with the development of a vascular network at the base of the skull, thus making the diagnosis of Moyamoya disease (Figures 2,3). On the Flair and T2-weighted sequence, cortical atrophy and areas of gliosis related to ischemic sequels were found bilaterally in the fronto-parietal region, as well as stigma of cerebromeningeal hemorrhage (Figure 3). Biological examinations were normal.
Discussion
Derived from the Japanese language, the term moyamoya means smoke cloud. Moyamoya disease is a chronic cerebrovascular disease of undetermined origin first described by Suzuki and Takasu in 1969 [1]. It is characterized by stenosis and progressive occlusion of the distal portion of the internal carotid arteries as well as of the proximal portion of the middle and anterior cerebral arteries, resulting in the development of up to three collaterals: Collaterals of the perforating vessels that form an abnormal vascular network at the base of the skull having a cloudy or smoke volute appearance hence the name moyamoya; then the leptomeningeal collaterals that are developed from the posterior cerebral arteries and finally the transdural collaterals that derive from the external carotid arteries [2]. Epidemiologically, moyamoya disease is most common in East Asia. There is a familial form of the disease which is autosomal dominant with incomplete penetrance. Women seem to be more affected than men with a sex ratio of 2.18 and there are two peaks of incidence: around the age of 5 years and during the 4th decade [3,4]. The manifestations of the disease change according to age. In children, recurrent ischemic strokes are more frequent, triggered by dehydration and hyperventilation (crying, physical activity); whereas in adults, cerebral or meningial hemorrhages are more frequently observed [5]. The clinical signs found are not specific to the disease, but are related to ischmic stroke or cerebral hemorrhage. Cognitive deficiencies, migraine-like headaches and convulsions may also be present. Imaging plays an important part in diagnosis of the disease. The CT scan, which is most often performed in the first instance in the context of an emergency, can find parenchymal abnormalities (recent ischemia or sequels, cerebral hemorrhage). On the other hand, it is less efficient for the study of arteries which are based on cerebral MRI and cerebral arteriography. On MRI, different abnormalities are found: stenosis of the supra-clinoid portion of the internal carotid arteries, of the proximal portion of the ACA and ACM associated with the presence of the abnormal vascular network (moya) which appears in flow void at the base ganglia thus establishing the positive diagnosis of the disease. Other signs such as the ivy sign corresponding to a leptomeningeal hypersignal on the flair or T1 injected sequences can be observed [6]. The parenchymal outcome of the disease (ischemia, hemorrhage, parenchymal atrophy) depends on the degree of progression and is best analyzed on FLAIR. In addition to the diagnostic purpose, MRI is used for preoperative evaluation of the disease as well as postoperative follow-up with the ASL sequence to assess cerebral perfusion. Angiography confirms the diagnosis of the disease by highlighting arterial stenoses and the moya network, and allows a better study of the transdural anastomoses. The Suzuki classification allows to distinguish 06 stages of evolution describing the natural history of moyamoya disease [1]:
Stage 1: stenosis
Stage 2: appearance of moya vessels
Stage 3: progression of moya vessels
Stage 4: appearance of transdural vessels
Stage 5: progression of transdural vessels and decrease of moya vessels
Stage 6: occlusion and disappearance of moya vessels.
Therapeutic management is based on medicinal means (antiplatelet, anticoagulant) and especially on revascularization surgery. There are 03 types of surgical revascularization: Direct bypass surgery (anastomosis of the superficial temporal artery to the middle cerebral artery), indirect bypass surgery or pialsynangiosis (consists of making drill holes through the cranial cavity with the aim of promoting the development of transduralanastomosis) or even combined direct and indirect bypass procedures [7]. Surgical indication must be taken in multidisciplinary consertation, considering the patient’s clinical condition, MRI and angiography data.
Conclusion
Moyamoya disease is a rare cerebral arteriopathy of undetermined origin responsible for stroke in children as well as in adults. Positive diagnosis is possible thanks to MRI and arteriography. Management requires multidisciplinary collaboration and relies on revascularization surgery, which must be indicated at the optimal time during the evolution of the disease.
Learning points
● Moyamoya disease is a cerebral vascular disease of undetermined origin responsible mainly for ischemic stroke in children and cerebral hemorrhage in adults.
● Cerebral MRI and arteriography allow a positive diagnosis of the disease, and then to study its parenchymal and hemodynamic outcomes.
● Management is based on revascularization surgery which should not be indicated too early or too late in order to avoid neurological sequels.
Declarations
Competing interests: The authors declare that they have no links of interest.
This research did not receive any specific subsidy from public, commercial or not-for-proft funding organizations.
Article produced in compliance with legal, ethical and institutional rules.
References
- Suzuki J, Takaku A. Cerebrovascular “moyamoya” disease. Disease showing abnormal net-like vessels in base of brain. Archives of neurology. 1969; 20: 288-299.
- Ancelet C, Boulouis G, Blauwblomme T, Kossorotoff M, Rodriguez Regent C, Mellerio C, et al. [Imaging Moya-Moya disease]. Revue neurologique. 2015; 171: 45-57.
- Currie S, Raghavan A, Batty R, Connolly DJ, Griffiths PD. Childhood moyamoya disease and moyamoya syndrome: a pictorial review. Pediatricneurology. 2011; 44: 401-413.
- Kuriyama S, Kusaka Y, Fujimura M, Wakai K, Tamakoshi A, et al. Prevalence and clinicoepidemiological features of moyamoya disease in Japan: findings from a nationwide epidemiological survey. Stroke. 2008; 39: 42-47.
- Velo M, Grasso G, Fujimura M, Torregrossa F, Longo M, Granata F, et al. Moyamoya Vasculopathy: Cause, Clinical Manifestations, Neuroradiologic Features, and Surgical Management. World Neurosurgery. 2022; 159: 409-425.
- Bentaleb D, Boumlik K, Hafoud S, Labied M, Sabiri M, et al. Maladie de Moyamoya : Le signe du lierre. Journal d’imagerie diagnostique et interventionnelle. 2022.
- Xu R, Xie ME, Khalifeh J, Feghali J, Yang W, et al. Timing of revascularization in ischemic Moyamoya disease: Association of early versus delayed surgery with perioperative and long-term outcomes. World Neurosurg. 2022.