
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
Perifissural pulmonary nodules in oncology
patients – Always benign?
Esther Pompe1*; Firdaus A Mohamed Hoesein1; Gerdien Kramer2; Pim A de Jong1; Onno M Mets3
1Department of Radiology, University Medical Center, Utrecht University, Utrecht, The Netherlands.
2Department of Radiology, Martini Hospital, Groningen, The Netherlands.
3Department of Radiology, Amsterdam UMC, Amsterdam, The Netherlands.
*Corresponding Author : E Pompe
Department of Radiology, University Medical Center Utrecht, Postbus 85500, 3508 GA Utrecht, E.03.511, Netherlands.
Tel: 0031 649502414;
Email: esther.pompe@gmail.com
Received : Jun 27, 2022
Accepted : Oct 06, 2022
Published : Oct 13, 2022
Archived : www.jcimcr.org
Copyright : © E Pompe (2022).
Abstract
Pulmonary nodules are a frequent finding on chest CT. Many are Perifissural Pulmonary Nodules (PFN), which are shown to be benign on follow-up in lung cancer screening and routine care subjects and represent intrapulmonary lymph nodes. Since a growing number of patients that undergo CT have an oncology history, it is increasingly important to have knowledge on whether metastases can mimic PFN and whether these lesions should be treated with more suspicion in oncology patients. We present eight oncology patients harbouring PFN to illustrate the current diagnostic uncertainty of this finding and highlight the need for further prospective data collection.
Keywords: Metastases; Perifissural pulmonary nodules; Chest CT.
Citation: Pompe E, Hoesein FAM, Kramer G, Jong PA, Mets OM. Perifissural pulmonary nodules in oncology patients – Always benign?. J Clin Images Med Case Rep. 2022; 3(10): 2100.
Background
Pulmonary nodules are a frequent finding on chest Computed Tomography (CT). Approximately a fourth of these represent Perifissural Nodules (PFN) [1,2]. Characteristically, PFN are sharply circumscribed, homogeneous, noncalcified solid nodules with an oval, lentiform or triangular shape [1]. In relation to fissures, PFN are described as typical (ie. fissure-attached) or a typical (ie. perifissural location without visible attachment) [1]. It has been shown that PFN do not represent early lung cancer and should not routinely initiate follow-up imaging in a screening setting [1-3].
In daily clinical practice many subjects have a history of malignancy and undergo chest CT to search for metastatic disease. In this setting, CT-detected perifissural nodules can potentially be misinterpreted as metastases leading to unnecessary diagnostic work-up or even withholding of potentially curative therapy, or as benign lesions while actually being metastases. Data on whether metastases can mimic PFN and whether these lesions should be treated with more suspicion in oncology patients is currently insufficient. We present a case series of eight oncology subjects harbouring PFN to illustrate the current diagnostic uncertainty of this finding.
Case presentations
All cases are routine-care oncology subjects from secondary and tertiary care centres, not originating from CT lung cancer screening. They were consecutively collected by five thoracic radiologists during daily-routine diagnostic interpretation. All patients received thin section chest CT as part of their standard clinical oncology work-up and surveillance. Six subjects had longitudinal chest CT scans showing imaging changes consistent with pulmonary metastatic disease, and two subjects underwent Video Assisted Thoracoscopic Surgical Excision (VATS) to exclude pulmonary metastatic disease. Clinical information on these cases is described in detail below, and is summarized in Table 1.
Table 1: The course of endoscopic treatments.
| Case | Sex / Age (yr) | Malignancy | Interval between most recent CT imaging and cancer diagnosis | Prior CT imaging available | Figure | Initial CT imaging findings | Follow-up CT imaging findings |
|---|---|---|---|---|---|---|---|
| 1 | M / 74 | 1) Neuroendocrine tumour of the colon 2) Laryngeal carcinoma |
1) 3 months 2) At time of diagnosis |
Yes | 1 | Small, well-defined rounded right upper lobe nodule in close relation with the major fissure.
Additional bilateral typical PFNs. |
Growth and morphologic change. |
| 2 | M / 23 | Osteosarcoma of the femur | 5 years | Yes | 2 | Small, well-defined rounded right lower lobe nodule in close relation to the major fissure. Additional bilateral PFNs. | Growth and morphologic change. |
| 3 | F / 41 | 1) Radiation induced osteosarcoma 2) Pelvis Ewing sarcoma |
1) At time of diagnosis 2) 27 year |
No | 3 | Small, well-defined ovoid nodule along the left major fissure. Three additional parenchymal nodules bilaterally. | Growth and morphologic change. Proof of several other lung metastases. |
| 4 | M / 79 | Oesophagus carcinoma | 2 years | Yes | 4 | Small well-defined nodule along the left major fissure. | Growth and morphologic change. Diffuse metastatic disease |
| 5 | M / 55 | Oropharyngeal carcinoma | 4 months | Yes | 5 | Triangular well-defined nodule in the apex of the left lower lobe in close relation to the major fissure. Two additional suspicious solid nodules. | Growth and morphologic change. PET-CT confirmation of pulmonary metastatic disease. |
| 6 | M / 67 | Transitional cell carcinoma of the urinary tract | At time of diagnosis | No | 6 | Small well-defined rounded right lower lobe nodule in close relation to the major fissure. | Growth and morphologic change. Proof of several other lung metastases. |
| 7 | M / 73 | Chondrosarcoma of the femur | 9 years | No | 7 | One lenticular and one triangular nodule in close relation to an accessory fissure. | PET-CT negative. |
| 8 | M / 60 | Colorectal carcinoma with liver metastases | 15 months | No | 8 | Two small, well-defined angular subpleural nodules in the left lower lobe. | No interval change. |
Cases with perifissural nodules showing change on longitudinal imaging, in keeping with pulmonary metastastic disease
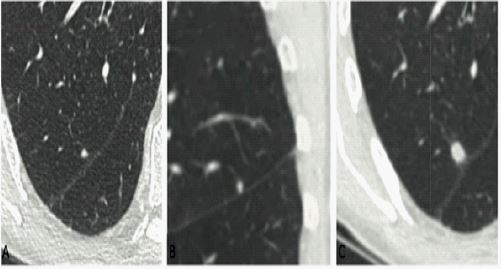
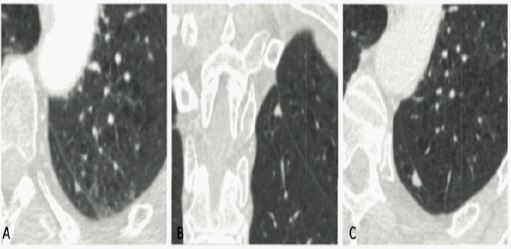
Case 1: A 74 years old male with two primary malignancies; a neuroendocrine colon carcinoma and a laryngeal carcinoma. He had multiple typical PFNs bilaterally and the majority did not change on longitudinal imaging. During follow-up a suspicious round perifissural nodule was noted in the right upper lobe, which was labelled most likely a metastasis based on growth and morphologic transformation. When compared to prior imaging, the suspicious lesion developed from a benign appearing perifissural nodule (Figure 1 A-C). More careful retrospective evaluation of several older scans revealed that this perifissural nodule had not always been present and had suddenly appeared in a scan interval. In contrast, the other PFNs in this patient were present on all scans and did not change in size or morphology over time. The subject was referred to a specialized center for head and neck cancer therapy and lost to follow-up.
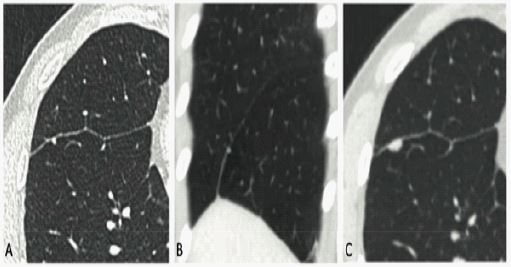
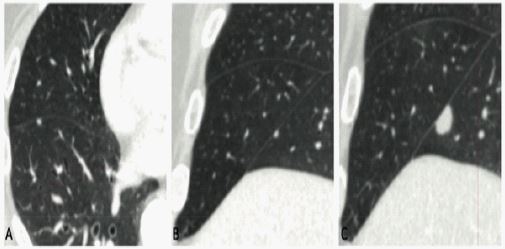
Case 2: A 23 years old male with an osteosarcoma of the femur. A CT scan 5 years after baseline CT showed a well-defined nodule in the right lower lobe at a location where previously a presumed benign PFN was present (Figure 2 A-C). Again, careful retrospective evaluation of several prior CT scans revealed that this nodule had not always been present, but appeared in a scan interval. Since this patient was known with two prior lung metastases, treatment strategy did not change. Given the highly suspicious morphology, growth and patient history, local radiotherapy was applied without obtaining pathological proof.
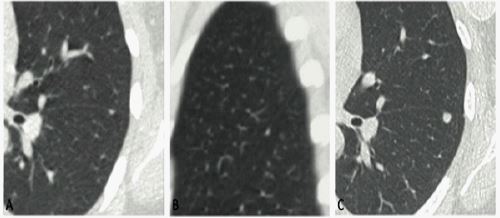
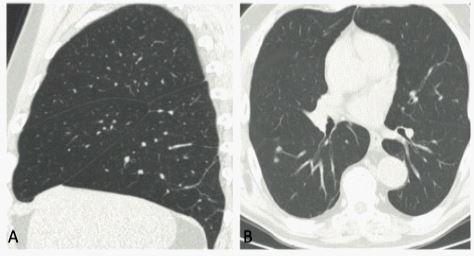
Case 3: A 41 years old female with two metachronous sarcomas in the pelvis. The first was a Ewings sarcoma treated with radiation 27 years previously, the second a radiation-induced osteosarcoma of the pelvis. A small well-defined ovoid nodule along the major fissure in the left lower lobe was found, which was initially labelled a benign PFN (Figure 3 A-C). Three other pulmonary parenchymal nodules were identified, which in the absence of a previous chest CT scan were considered suspicious for pulmonary metastases. At 4 months follow-up all four nodules had grown significantly. Based on this rapid growth, the four nodules were labelled metastases and palliative treatment instituted. No pathological proof was obtained. The patient died 2 months later secondary to metastatic disease.
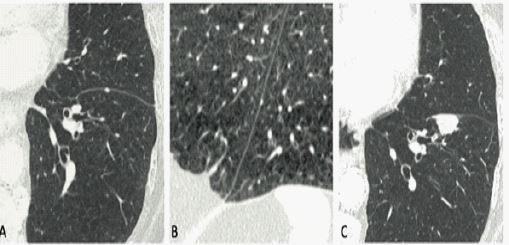
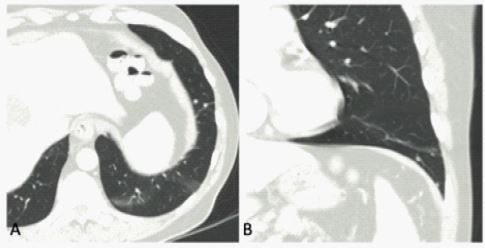
Case 4: A 79 year old male with a 2 year history of oesophageal carcinoma, treated with excision and gastric pull-up. Pulmonary metastatic disease was suggested on an abdominal CT performed for suspected appendicitis. Chest CT imaging confirmed multiple pulmonary and extrapulmonary metastases, setting treatment goals to palliative care. Careful evaluation of several prior CT scans revealed that all but one pulmonary metastases were new. The largest metastasis along the left major fissure was retrospectively found to be present on a CT obtained 19 months before, and was at that time indistinguishable from a benign PFN (Figure 4 A-C). However, this perifissural nodule had appeared in the 3 month scan interval since the last CT. Along the same fissure a benign typical PFN was stable over multiple CT scans.
Case 5: A 55 year old male with oropharyngeal cancer who developed three new pulmonary nodules on a 4 month follow-up chest CT. One of these nodules had typical morphology of a PFN in the superior segment of the left upper lobe (Figure 5 A-C). The other two parenchymal nodules were suspicious for pulmonary metastases. All three nodules grew on follow-up, and were also found to be positive on Positron Emission Tomography (PET). Given the characteristic clinical course, no pathological confirmation was obtained. The patient died eight months later from disseminated metastatic disease.
Case 6: A 67 years old male with a transitional cell carcinoma of the bladder. The baseline CT scan demonstrated a typical PFN in the right lower lobe (Figure 6 A-C). Over a period of 6 months the perifissural nodule grew and multiple other parenchymal nodules characteristic of pulmonary metastatic disease appeared. Since the primary tumour progressed as well, this was labelled metastatic bladder cancer and managed as such.
Cases with perifissural nodules that proved to be benign intrapulmonary lymph nodes
Case 7: A 73 years old male with chondrosarcoma of the femur. He had two PFN, one lenticular and one triangular, adjacent to an accessory fissure in the right lower lobe (Figure 7). Prior CT was not available to assess long term stability. Both nodules were negative on a staging PET CT scan, and no other suspicious metastatic lesions were identified. However, since the primary tumour was PET negative diagnostic concern remained over these PFN. The multidisciplinary team elected to perform VATS wedge resection of both nodules. Histopathology revealed benign intrapulmonary lymph nodes.
Case 8: A 60 year old male with colorectal carcinoma with liver metastases appropriate for potentially curative partial liver resection. At chest CT, two small, well-defined PFN were seen (Figure 8). Both nodules had been stable over 15 month follow-up. However, given the major liver resection proposed, the multidisciplinary team elected to excise both nodules using VATS after hook wire guidance. Histopathology revealed two benign intrapulmonary lymph nodes.
Discussion
In this case series, we discuss the challenges of managing perifissural nodules in oncology patients. Previous research has shown that PFN are common and benign, representing intrapulmonary lymph nodes [1-3]. Incidentally found PFN should therefore not routinely initiate follow-up imaging when encountered in either routine clinical practice or lung cancer screening setting. However, their significance and optimal management in oncology patients remains unclear.
Some studies conducted in subjects with primary lung cancer have shown pathologically proven metastatic spread to perilesional peripheral intrapulmonary lymph nodes, impacting staging and survival [4-6]. However, the data regarding metastasis from extrapulmonary malignancies is scarce [7,8]. Golia Pernicka et al. [9] evaluated 62 oncology patients harbouring 112 PFN, finding 59 patients (95.2%) with stable or smaller PFN after median follow-up of 5.7 years. They concluded stable PFN can be regarded as benign. However, since almost half (ie. 30/62) of the study population was on chemotherapy during the study period, stable or smaller PFN could also have represented metastases that responded to chemotherapy.
In oncology patients the detection of pulmonary metastatic disease greatly impacts treatment strategy. On a single CT scan, metastatic disease can be indistinguishable from PFN based on morphology, as illustrated by our cases. PFN are commonly located within 15-20 mm of the pleural surface, in the lower lung zones and may demonstrate a pleural tag [1,10,11]. However, lung metastases also typically demonstrate a smooth and rounded morphology and are most often located in the peripheral and lower lung zones. Although the distance from the costal pleura was shown to be an independent predictor of metastases in a cohort with melanoma patients, a perifissural location did not separate benign PFN from metastatic lesions [12].
When PFN are encountered in oncology patients, careful inspection of the nodule should always be performed in orthogonal planes to confirm the nodule fulfils PFN criteria. Studies have shown substantial interobserver variation in pulmonary nodule classification [13,14], which remains an inherent limitation in daily practice. The best classifier remains comparison to previous CT imaging to assess for nodule growth. This case series illustrates multiple examples of presumed PFN that were retrospectively shown to grow or appear in the prior scan intervals. Interestingly, other PFN in the same subjects showed long term stability. It is noted that growth assessment is not foolproof, with PFN occasionally showing temporary rapid growth [1]. Nevertheless, a lymph node will have an upper size limit that a metastasis lacks. In cases where doubt has risen about nodule aetiology, short term follow-up is likely a good strategy, which is in agreement with prior nodule management recommendations [8,15].
Based on our review of the literature, the overall incidence of perifissural metastases and their frequency with respect to primary malignancy subtype and stage is not well defined. Available nodule management guidelines either do not apply in patients with known prior malignancy [15] or is based on low-grade evidence [8]. Therefore, given the paucity of knowledge, radiologists are left with the options to either ignore the potential significance of small perifissural metastasis, recommend follow-up CT scans in high frequency with attendant workload, cost and radiation exposure impact, or even recommend guided resection; neither an optimal strategy and most likely highly variable between observers.
Conclusion
In conclusion, this report discusses the current management dilemma regarding PFN found in patients with a known prior extrapulmonary malignancy. Although this situation is common, there is insufficient data to guide radiologists. We acknowledge this is a small case series with limited pathologic proof. However, our cases nicely illustrate the need for prospective cohort data to estimate the absolute risk and negative predictive value of PFNs in various tumour types and different stages. A waiting further data, radiologists and other members of the multidisciplinary team in oncology care should at least be aware of perifissural metastases mimicking PFN, and consider the risk on a per case basis. It is important to focus specifically on nodule morphology in three orthogonal planes, as well as compare to all available prior imaging. If consequences are high, short term follow-up is probably the preferred strategy.
Conflict of interest: Dr. Pompe reports personal fees from Thirona BV outside the submitted work. Dr. Mohamed Hoesein, Dr. Mets, Dr. Mayo, Dr. Kramer, and Prof. Dr. de Jong have nothing to disclose.
References
- de Hoop B, van Ginneken B, Gietema H, Prokop M. Pulmonary perifissural nodules on CT scans is rapid growth is not a predictor of malignancy. Radiology. 2012; 265: 611-616.
- Ahn MI, Gleeson TG, Chan IH, et al. Perifissural nodules seen at CT screening for lung cancer. Radiology. 2010; 254: 949-956.
- Mets OM, Chung K, Scholten ET, et al. Incidental perifissural nodules on routine chest computed tomography: Lung cancer or not? Eur Radiol. 2018; 28: 1095-1101.
- Osarogiagbon RU, Eke R, Sareen S, et al. The impact of a novel lung gross dissection protocol on intrapulmonary lymph node retrieval from lung cancer resection specimens. Ann Diagn Pathol. 2014; 18: 220-226.
- Smeltzer MP, Faris N, Yu X, et al. Missed intrapulmonary lymph node metastasis and survival after resection of non-small cell lung cancer. Ann Thorac Surg. 2016; 102: 448-453.
- Boubia S, Barthes FL, Danel C, Riquet M. Peripheral intrapulmonary lymph node metastases of non-small-cell lung cancer. Ann Thorac Surg. 2004; 77: 1096-1098.
- Taniguchi Y, Haruki T, Fujioka S, Adachi Y, Miwa K, Nakamura H, et al. Subpleural intrapulmonary lymph node metastasis from colorectal cancer. Ann Thorac Cardiovasc Surg. 2009; 15: 250-252.
- Callister ME, Baldwin DR, Akram AR, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules. Thorax. 2015; 70: ii1-ii54
- Golia Pernicka JS, Hayes SA, Schor-Bardach R, et al. Clinical significance of perifissural nodules in the oncologic population. Clinical Imaging. 2019; 57: 110-114.
- Matsuki M, Noma S, Kuroda Y, Oida K, Shindo T, et al. Thin-section CT features of intrapulmonary lymph nodes. J Comput Assist Tomogr. 2001; 25: 753-756.
- Snoeckx A, Reyntiens P, Desbuquoit D, Spinhoven MJ, van Schil PE, et al. Evaluation of the solitary pulmonary nodule: Size matters, but do not ignore the power of morphology. Insights Imaging. 2018; 9: 73-86.
- Soliman M, Petrella T, Tyrrell P, et al. The clinical significance of indeterminate pulmonary nodules in melanoma patients at baseline and during follow-up chest CT. Eur J Radiol Open. 2019; 6: 85-90.
- van Riel SJ, Sanchez CI, Bankier AA, et al. Observer variability for classification of pulmonary nodules on low-dose CT images and its effect on nodule management. Radiology. 2015; 277: 863-871.
- Schreuder A, van Ginneken B, Scholten ET, et al. Classification of CT pulmonary opacities as perifissural nodules: Reader variability. Radiology. 2018; 288: 867-875.
- Mac Mahon H, Naidich DP, Goo JM, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society. 2017. Radiology. 2017; 284: 228-243.