
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
The bile duct stenosis by a complete annular
pancreas: A rare association
A Lahfidi*; Z el yousfi; WM Traore; K Imrani; N Moatassim Billah; I Nassar
Central Radiology Department, Hospital Ibn Sina, Faculty of Medicine and Pharmacy, Mohammed V University, Rabat, Morocco.
*Corresponding Author : Lahfidi Amal
Pediatric Radiology Department, Rabat Children’s Hospital, Ibn Sina Hospital, Mohamed V University, Rabat, Morocco.
Email: lahfidial@gmail.com
Received : Sep 09, 2022
Accepted : Oct 07, 2022
Published : Oct 14, 2022
Archived : www.jcimcr.org
Copyright : © Lahfidi A (2022).
Abstract
The annular pancreas is a rare congenital anomaly with retained ventral pancreas encircling the duodenum. It can be either complete or incomplete. The annular pancreas may manifest clinically in the neonate, but in the elderly it can mimic a wide range of clinical entities as a duodenal obstruction, rarely as a biliary tract obstruction making the diagnosis difficult. At present imaging modalities such as CT, ERCP and MRCP are used to arrive at a diagnosis. We are reporting an unusual combination of annular pancreas and dilated biliary system due to distal common duct stenosis without pancreatitis or underlying malignancy which is a rare presentation in adults.
Keywords: Pancreas; Annular; Dilated bile duct; CT scan.
Citation: Lahfidi A, Yousfi Z, Traore WM, Imrani K, Moatassim Billah N, et al. The bile duct stenosis by a complete annular pancreas: A rare association. J Clin Images Med Case Rep. 2022; 3(10): 2102.
Introduction
Annular pancreas is an uncommon congenital abnormality, it consists of a ring of pancreatic tissue encircling the descending duodenum. It may manifest clinically in the neonate, but in the elderly it can mimic a wide range of clinical entities as a duodenal obstruction, rarely as a biliary tract obstruction making the diagnosis difficult. At present imaging modalities such as CT, ERCP and MRCP are used to arrive at a diagnosis. We are reporting an unusual combination of annular pancreas and dilated biliary system due to distal common duct stenosis without pancreatitis or underlying malignancy which is a rare presentation in adults.
Case report
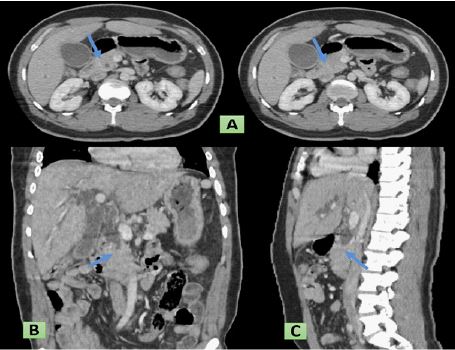
A 65-year-old male patient was admitted to the emergency room with epigastric pain, jaundice, very dark urine, and almost white stools that had developed 12 months ago. The biological work-up showed increases in the concentrations of total/direct bilirubin (14.0/12.9 mg/dL), alkaline phosphatase (744 U/L), and aspartate/alanine aminotransferase (226/549 U/L). Abdominal sonography revealed dilatation of the intrahepatic and Common Bile Ducts (CBD), with narrowing at the distal portion. Abdominal CT scan confirmed that CBD was dilated and shows pancreatic tissue encircling the second part of duodenum suggestive of annular pancreas (Figure 1). The Magnetic Resonance Cholangiopancreatography (MRCP) result was similar to the CT scan, and showed a fusiformly dilated CBD with distal CBD narrowing. The patient was diagnosed with annular pancreas complicated by dilated biliary system.
The endoscopic US examination shows a circumferential band like structure surrounding the duodenum and having the same echo pattern as the pancreas and confirmed a dilatation of the hepatic duct and a short, stenosis of the choledochal duct, looking benign with no signs of tumour like masses. The patient underwent abdominal laparotomy. Hepaticojejunal anastomosis for distal CBD stenosis was performed. The patient recovered successfully without any complications. 6 months after surgery, there was no evidence of symptoms having recurred.
Discussion
The annular pancreas is a rare congenital anomaly with retained ventral pancreas encircling the duodenum. Its first anatomical description seems to date back to 1818 by Tied man but its name was first attributed in 1862 by Ecker [1]. Its frequency is variable and difficult to assess: 1/20,000 cases in an autopsy series [2].
The embryological origin of the annular pancreas falls under two hypotheses:
-Persistence of the left ventral bud which will wrap around the intestinal loop during its rotation (Baldwin’s theory) [3].
-Deposition of embryonic remnants during rotation of the right ventral bud (Lecco theory) [4].
Annular pancreas can be either complete or incomplete. Complete annular pancreas: pancreatic parenchyma or an annular duct is seen to completely surround the 2nd part of duodenum. Incomplete annular pancreas: annulus does not surround the duodenum completely, giving a ‘crocodile jaw’ appearance [5].
The annular pancreas is revealed in half of the cases in children and in the other half in adults [1]. In children, the annular pancreas is most often revealed in the first week of life as a duodenal stenosis. It is estimated that annular pancreas accounts for 35% of the causes of duodenal atresia [6]. Other associated congenital malformations have been reported: Common mesentery, cardiac malformations, Down syndrome (or trisomy 21), anal imperforation, tracheoesophageal malformations, facial anomalies. The sex ratio is male, two males to one female. In adults, the anomaly is revealed between 40 and 60 years of age (mean age 45 years). In a series of 105 patients, the clinical manifestations and associated conditions are varied: Abdominal pain, jaundice, peptic ulcer, acute or chronic pancreatitis, biliarylithiasis, pancreatic or biliary cancer. Abdominal pain is the most frequent manifestation (70% of cases), followed by vomiting and nausea (47%). These manifestations usually reflect a digestive stenosis, complicated or not by a peptic ulcer. Jaundice is described in 12% of cases. It is related to choledocholedocholithiasis or to an ampulloma or to a cancer of the gallbladder. Pancreatic involvement is described in 13 to 24% of cases. It may take the form of acute pancreatitis or chronic pancreatitis with calcified or non-calcified stones [7].
In our case, no laboratory or clinical signs of pancreatitis were present and Endoscopic Ultrasonography (EUS), revealed a complete annular pancreas with dilated common bile duct, normal main pancreatic duct and normal duodenal ampulla. No malignant features were seen in the duodenal mucosa. No obvious mass lesions were seen.
In reviewing literature, not many cases of annular pancreas, causing biliary obstruction, without pancreatitis or (underlaying duodenal neoplasm) duodenal obstruction, were found.
The diagnosis of annular pancreas was initially based on duodenography, which demonstrated a regular midduodenal stenosis corresponding to the pancreatic ring [8]. Computed Tomography (CT) can directly show a periduodenal ring. Echo-endoscopy shows circumferential bandlike structure, isoechoic with the adjacent pancreas, surrounding the descending duodenum with hyperechoic foci or even true cystic dilatations of secondary ducts [9]. Finally, MRCP and ERCP (cholangio-pancréatographierétrograde) are the most reliable means to demonstrate a pancreatic duct encircling the duodenum, or even to look for associated biliary stenosis or signs suggestive of chronic pancreatitis and can also diagnose coexisting malignancies [7].
Peptic ulcer disease, pancreatic divisum, primary duodenal and pancreatic malignancies should be considered in the differential diagnosis of an adult patient suspected to have AP [10]. Fortunnally imaging shows a ring of normal pancreatic parenchyma (high T1-weighted signal intensity) about the duodenum and an aberrant pancreatic duct encircling the duodenum and joining the main pancreatic duct (best seen on MRCP).
The treatment of annular pancreas is essentially based on digestive bypass: Duodenojejunal bypass is the most efficient way to treat duodenal stenosis and the peptic ulcer.
In the presence of obstructive jaundice associated with annular pancreas the treatment is essentially based on biliary bypass with choledochoenterostomy or placement of an internal stent to relieve the obstruction. But only when there is clinical and laboratory evidence of cholestasis. The duodenal ring should not be cut because it contains a pancreatic duct whose rupture is complicated by a pancreatic fistula.
Surgical treatment of annular pancreas has an excellent prognosis as long as there is sufficient appropriate perioperative and postoperative care [11].
Conclusion
Annular pancreas presenting with extra hepatic obstructive jaundice is rare, it is usually associated with malignancies of ampulla, pancreas or the biliary tract and should not be overlooked in adults, and in a few cases as this one could be just an innocent bystander.
Learning points
‐ The annular pancreas is a rare congenital anomaly. Imaging plays a fundamental role in the revelation of this pathol ogy, hence the interest in knowing it.
‐ The abdominal CT and Magnetic Resonance Imaging (MRI) make the positive diagnosis by showing the islets of the pancreatic parenchyma encircle the 2nd duodenum.
‐ The treatment of annular pancreas is essentially based on digestive bypass.
‐ Surgical treatment should be avoided given postoperative complications such as pancreatic fistula.
Declarations
Financial support/conflict of interests: There is no funding supporting this work. The authors have no relevant affiliation or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter discussed in the manuscript.
Note: Informed Consent, Informed patient consent was obtained for publication of the case details.
Competing interests: The authors declare that they have no links of interest.
This research did not receive any specific subsidy from public, commercial or not-for-profit funding organizations.
Article produced in compliance with legal, ethical and institutional rules.
References
- Kiernan PD, Remine SG, Kiernan PC, Remine WH. Annular pancreas. Mayo clinic experience from 1957 to 1976 with review of the literature. Arch Surg. 1980; 115: 46-50.
- Ravitch MM. The pancreas in infants and children. Surg Clin N Am. 1975; 55: 377-385.
- Baldwin WM. A specimen of annular pancreas. Anat Rec (Hoboken). 1910; 4: 299-304.
- Lecco TM, Zur morphologie des Pankreas annulare. SitzungsbAkad Wissensch. 1910; 119: 391-406.
- Sandrasegaran K, Patel A, Fogel EL, et al. Annular pancreas in adults. AJR Am J Roentgenol. 2009; 193: 455-460.
- Synn AY, Mulvihill SJ, Fonkalsrud EW. Surgical disorders of the pancreas in infancy and childhood. Am J Surg. 1988; 156: 201-205.
- Yogi Y, Shibue T, Hashimoto S. Annular pancreas detected by endoscopic retrograde cholangiopancreatography: Report of four cases. Gastroenterol Jpn. 1987; 22: 92-99.
- Gilinsdky NH, Lewis JW, Flueck JA, Fried AM, et al. Annular pancreas associated with diffuse chronic pancreatitis. Am J Gastroenterol. 1987; 82: 681-684.
- Gress F, Yiengpruksawan A, Sherman S, Ikenberry S, Kaster S, Cerulli MA, et al. Diagnosis of annular pancreas by endoscopic ultrasound. Gastrointest Endosc. 1996; 44: 485-489.
- Adedeji OA, Trescoli Serrano C, Garcia Zarco M. Primary duodenal carcinoma. Postgrad Med J. 1995; 71: 354-358.
- Selvaraj B, Kumaran KS, Sekar GP. Annular pancreas-a case report and review of the literature. International Journal of Recent Trends in Science and Technology. 2014; 13: 317- 321.