
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 3
Prognostic value of hematological along with biochemical, and inflammatory parameters in COVID-19 infection
*Corresponding Author : Minoo Shahidi
Department of Hematology and Blood Banking, School of Allied Medical Sciences, Iran University of Medical Sciences, Tehran, Iran.
Email: shahidi.minoo@gmail.com
Received : Sep 07, 2022
Accepted : Oct 07, 2022
Published : Oct 14, 2022
Archived : www.jcimcr.org
Copyright : © Shahidi M (2022).
Abstract
Keywords: Background and objective: Coronavirus 2019 (COVID-19), first detected in patients in Wuhan, China, and soon became an international emergency concern. Since, blood tests can play a pivotal role in the early diagnosis and management the present study aimed to investigate any possible association between hematological and biochemical markers and the prognosis in these patients.
Methods: The study was conducted in 60 confirmed COVID-19 patients (31 males, 29 females; mean age 64.43 ± 17.52. The data were extracted from available medical records. COVID-19 patients were assigned to two groups: A “recovered” group and a “deceased” group. Examinations involved Complete Blood Count (CBC) and serum biochemical factors. Inflammatory indicators, including C-reactive protein (CRP), Neutrophil-To-Lymphocyte Ratio (NLR) was assessed in terms of age and gender in groups. The parameters were assessed again at the time of discharge and compared with those at admission.
Results: Elevated Neutrophil (NEUT), NLR, and Sodium were significantly correlated with adverse outcomes (P= 0.030 and 0.037, and 0.032 respectively). Low Levels Of Lymphocyte (LYMP) increased the occurrence of death in females (P= 0.011). Low platelet counts increased death rate in patients older than 60 years old (P= 0.021). In addition, higher ages were significantly associated with poor clinical outcome (P=0.031).
Conclusion: Among previously mentioned routine laboratory parameters NEUT, LYMP, NLR, PLT, and Na were valuable indicators for a prediction of severity and prognosis of COVID-19 patients upon hospital admission as well as during therapeutic interventions.
Keywords: SARS-CoV-2; COVID-19; hematological parameters; prognosis; biochemical parameters; inflammatory markers.
Citation: Shahidi M. Prognostic value of hematological along with biochemical, and inflammatory parameters in COVID-19 infection. J Clin Images Med Case Rep. 2022; 3(10): 2103.
Introduction
Since the arrival of 2020, the whole world has been struggling with a new outbreak of a flu-like illness.Blood tests including Complete Blood Count (CBC), biochemistry analysis, and inflammatory parameters (e.g., CRP and ESR) play a pivotal role in the early diagnosis, management, and therapy monitoring of infectious disease and are available in many laboratories. A part from neutrophil and platelet counts, the ratio of Neutrophil To Lymphocyte (NLR) and Platelet To Lymphocyte (PLR) have also been reported as the parameters that associated with worse prognosis infection. Therefore, the immunological, hematological, and biochemical parameters can be used not only as appropriate indicators to monitor therapy-related side effects but also to determine the disease prognosis [1-5]. In this regard, studies have shown that hematological and biochemical parameters may be useful indicators for determining the diagnosis and prognosis of COVID-19 [6-11]. The present study was performed to evaluate and compare hematological, biochemical, and inflammatory parameters in two independent groups recuperated/discharged and deceased COVID-19 patients. We aimed to investigate the possible association between these factors and the COVID19 outcome.
Materials and methods
Study participants
The current study was performed on 60 patients with COVID-19 who referred to Shahid Beheshti Hospital, Ardestan. All included patients showed a SARS-COV2 positive real-time Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) from nasal or throat swab according to the basis of the World Health Organization (WHO) guidelines. Patient’s demographic data, including age and sex, and clinical outcome as well as hematological, biochemical, and inflammatory parameters were all gathered from available medical records. According to the clinical outcome, patients were categorized into discharged/recovered and deceased group.
Laboratory data collection
Blood samples were taken from all patients and routine CBC test was performed by aKX-21 Sysmex analyzer. Hematological parameters include total White Blood Cell Count (WBC), Lymphocyte (LYMP %), Neutrophils (NEUT %), mixed cells (including monocytes, eosinophils, and basophils % together), Hemoglobin (Hb), Erythrocytes (RBC), Platelets (PLT), and other indices such as Mean Corpuscular Volume (MCV), Mean Platelet Volume (MPV), Red Cell Distribution Width (RDW), Mean Hemoglobin Concentration (MHC), and Mean Corpuscular Hemoglobin Concentration (MCHC). Biochemical parameters such as Urea, Creatinine (Cr), Sodium (Na) and Potassium (K) were also evaluated. In addition, ESR (Erythrocyte sedimentation rate) and CRP (C Reactive Protein) were analyzed and compared between the two groups. Furthermore, for a subgroup of 7 recovered patients, a CBC test was performed again at the time of discharge from the hospital and compared with those parameters at admission.
Statistical analysis
The statistical analysis was performed using the SPSS version 24 and Graph pad Prism software version 8.3. Categorical variables were described as counts and percentages. Chi-square or Fisher’s exact test was used to evaluate any significant difference for categorical factors. Continuous variables were expressed as mean ± Standard Deviation (SD). Mann-whitney U test and T-test were applied for continuous variables with or without normal distribution, respectively. Also, the diagnostic values of NLR and NEUT in COVID-19 outcome were assessed by Receiver Operating Characteristic (ROC) and Area Under The ROC Curve (AUC). Parameters with AUC<0.6 and no statistical significance (P>0.05) with AUC=0.5 were excluded. The best diagnostic cut-off was selected employing the Youden index. A p-value less than 0.05 was considered statistically significant.
Results
Sixty patients were included in the current study comprising of 31 males and 29 females ranging from 25 to 94 years old (64.43 ± 17.52). As Table 1 shows, in total, 45 cases (23 males, 22 females; 61.64 ± 18.32) were recovered while 15 patients (8 males, 7 females; mean age 72.80 ± 11.78) died. We found that the mean age of deceased patients was significantly higher compared to the recovered patients (P=0.031). In contrast, there was no significant difference in terms of gender between the two groups (P=0.999).
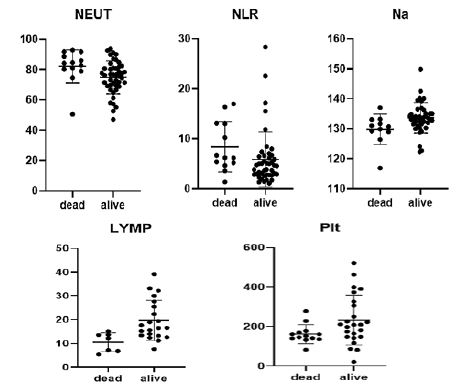
Hematological parameters were compared between deceased and recovered patients irrespective of their age or gender (Table 2). Based on our findings, neutrophil, as well as Neutrophil to Lymphocyte Ratio (NLR) were significantly higher in the deceased group (P=0.037 and 0.030, respectively). However, other hematological parameters such as total WBC, mixed cells, and Hb did not reveal a significant correlation with the disease outcome (P-value: 0.533, 0.090, and 0.762, respectively). Considering serum factors, Na was significantly higher in the recovered group compared to the deceased patients (P= 0.032). However, no association was found for Potassium, Urea, and Creatinine (P=0.500, 0.373, and 0.214, respectively). Hematological parameters were assessed between the recovered and deceased groups with respect to the patients’ gender. We found that NEUT, NLR, and LYMP were significantly associated with clinical outcome in females (P= 0.005, 0.028, and 0.011, respectively, Table 3), but no in males. Moreover, hematological parameters were compared between the recovered and deceased groups with regard to the age of patients (Table 4). Our results showed that in patients < 60 years of age, increased NLR was remarkably associated with poor outcome (P=0.028), whereas in patients ≥60 years, a low platelet count was significantly associated with a higher mortality rate (P=0.021). Figure 1 shows the scatter plots of the significant factors for both recovered and deceased patients.
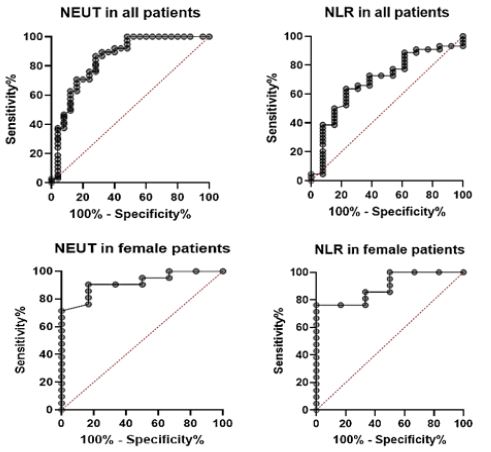
The ROC curve was illustrated for NLR and NEUT to determine their potential as predictors of hospital death (Figure 2 and Table 5). The results showed that NEUT in female patients was the most suitable parameter in distinguishing recovered from deceased cases with AUC, cut-off, sensitivity, and specificity of 0.917, 84.10, 83.3%, and 90.5% respectively. Regarding NLR in female patients, the AUC was 0.897, the cut-off was 6.02, the sensitivity was 100% and the specificity was 76.2%. For the NEUT in the total population, the sensitivity was 84.6% and the specificity was 65.9%. For NLR in the total population, the sensitivity and specificity were 76.9% and 63.6%, respectively. In a group of recovered patients (n=7), we analyzed and compared hematological parameters including WBC, LYMP, NEUT, NLR, and RDW documented upon admission to those at the time of discharge from the hospital. The difference between results was visualized as an error-Bar chart (Figure 3). CRP, as an inflammatory marker, was assessed and assigned on a scale of grades 0 to 3 in both recovered and deceased groups. Subsequently, the relationship between the grade of CRP and the observed clinical outcome was investigated. Based on our findings (Table 6), CRP was increased in both groups. No statistically significant relationship was observed between the grade of CRP and the clinical outcome of the disease (P=0.873). Similarly, we did not find any association between ESR level and the clinical outcome (P=0.545).
Table 1: Demographic characteristics of included covid-19 patients.
| Factor | Total (n=60) | Recovered (n=45) | Deceased (n=15) | P |
|---|---|---|---|---|
| Age, Mean ± SD | 64.43 ± 17.52 | 61.64 ± 18.32 | 72.80 ± 11.78 | 0.031 |
| Sex, N (%) | 0.999 | |||
| Male | 31(51.7) | 23(51.1) | 8(53.3) | |
| female | 29(48.3) | 22(48.9) | 7(46.7) |
Table 2: The course of endoscopic treatments.
| Factor, Mean ± SD | Total (n=60) | Recovered (n=45) | Deceased (n=15) | P-Value |
|---|---|---|---|---|
| WBC (103/ul ± SD) | 7.39 ± 3.73 | 7.57 ± 4.06 | 6.87 ± 2.56 | 0.533 |
| RBC (103/ul ± SD) | 4.69 ± 0.59 | 4.69 ± 0.62 | 4.67 ± 0.53 | 0.905 |
| Hb(gr/dl ± SD) | 13.26 ± 1.62 | 13.29 ± 1.64 | 13.15 ± 1.63 | 0.762 |
| Hct (% ± SD ) | 38.12 ± 4.35 | 38.23 ± 4.33 | 37.79 ± 4.53 | 0.736 |
| MCV(fl ± SD) | 81.01 ± 5.84 | 80.82 ± 6.23 | 81.57 ± 4.69 | 0.671 |
| MCH (pg± SD) | 28.38 ± 1.95 | 28.44 ± 2.06 | 28.20 ± 1.66 | 0.678 |
| MCHC (gr/dl ± SD) | 34.60 ± 1.96 | 34.53 ± 2.19 | 34.79 ± 1.10 | 0.660 |
| PLT (103/ul ± SD) | 206.07 ± 107.46 | 218.37 ± 117.72 | 170 ± 58.37 | 0.133 |
| MIX (% ± SD) | 5.96 ± 3.29 | 6.37 ± 3.22 | 4.53 ± 3.27 | 0.090 |
| LYMP (% ± SD) | 18.08 ± 3.29 | 19.20 ± 9.53 | 14.79 ± 8.66 | 0.119 |
| NEUT (% ± SD) | 76.51 ± 11.15 | 74.84 ± 10.78 | 82.15 ± 10.93 | 0.037 |
| NLR (X ± SD) | 6.44 ± 5.45 | 5.87 ± 5.49 | 8.38 ± 5.02 | 0.030 |
| RDW-CV (% ± SD) | 13.86 ± 1.21 | 13.92 ± 1.35 | 13.69 ± 0.59 | 0.529 |
| RDW-SD (fl ± SD) | 43.03 ± 4.44 | 43.29 ± 4.87 | 42.20 ± 2.63 | 0.427 |
| PDW (fl ± SD) | 12.86 ± 2.34 | 12.72 ± 2.45 | 13.31 ± 1.97 | 0.423 |
| MPV (fl ± SD) | 9.81 ± 1.01 | 9.70 ± 1.03 | 10.15 ± 0.91 | 0.152 |
| PLCR (% ± SD) | 24.92 ± 7.14 | 24.21 ± 7.11 | 27.14 ± 6.99 | 0.183 |
| ESR (mm/h ± SD) | 58.72 ± 38.33 | 56.90 ± 40.23 | 64.67 ± 32.21 | 0.545 |
| Urea (mg/dl ± SD) | 52.36 ± 37.86 | 49.79 ± 37.33 | 61.45 ± 40.02 | 0.373 |
| Na (mmol/L ± SD) | 132.80 ± 5.24 | 133.64 ± 5.04 | 129.83 ± 5.08 | 0.032 |
| K (mEq/L ± SD ) | 4.13 ± 0.65 | 4.09 ± 0.68 | 4.25 ± 0.56 | 0.500 |
| Cr (mg/dl ± SD) | 1.41 ± 0.94 | 1.38 ± 0.98 | 1.53 ± 0.82 | 0.214 |
| BS | 150.62 ± 90.67 | 150.61 ± 96.47 | 150.63 ± 68.85 | 0.695 |
| NLR and RDW-SD | 1.60 ± 2.35 | 1.68 ± 2.56 | 1.32 ± 1.47 | 0.628 |
| NLR and RDW-CV | 1.60 ± 1.61 | 1.61 ± 1.76 | 1.55 ± 0.94 | 0.910 |
Table 3: Hematologic factors for recovered and deceased patients in terms of patient’s gender.
| Male | Female | |||||
|---|---|---|---|---|---|---|
| Factor | Alive | Dead | P | Alive | dead | P |
| PLT | 191.57 ± 116.80 | 161.87 ± 64.80 | 0.503 | 247.71 ± 114.27 | 179.28 ± 53.50 | 0.142 |
| ESR | 53.17 ± 38.66 | 48 ± 19.85 | 0.759 | 60.09 ± 42.20 | 81.33 ± 34.96 | 0.272 |
| WBC | 7.55 ± 4.65 | 6.19 ± 3.15 | 0.449 | 7.59 ± 3.42 | 7.64 ± 1.56 | 0.969 |
| RDW-CV | 13.93 ± 1.56 | 13.50 ± 0.64 | 0.486 | 13.91 ± 1.13 | 13.87 ± 0.51 | 0.924 |
| RDW-SD | 43.59 ± 5.33 | 41.38 ± 2.26 | 0.300 | 42.97 ± 4.42 | 43.01 ± 2.91 | 0.979 |
| NEUT | 74.82 ± 12.21 | 77.84 ± 13.18 | 0.578 | 74.86 ± 9.27 | 87.18 ± 4.66 | 0.005 |
| NLR | 6.98 ± 7.14 | 6.69 ± 5.03 | 0.921 | 4.66 ± 2.41 | 10.35 ± 4.63 | 0.028 |
| LYMP | 18.73 ± 10.60 | 18.49 ± 10.15 | 0.955 | 19.72 ± 8.44 | 10.57 ± 4.00 | 0.011 |
| NLR and RDW-SD | 1.92 ± 2.89 | 0.82 ± 1.25 | 0.340 | 1.43 ± 2.18 | 1.91 ± 1.59 | 0.621 |
| NLR and RDW-CV | 1.73 ± 2.14 | 1.22 ± 1.03 | 0.551 | 1.48 ± 1.28 | 1.94 ± 0.74 | 0.413 |
Table 4: Hematologic factors between recovered and deceased patients in terms of patient’s age.
| Age < 60 | Age≥60 | |||||
|---|---|---|---|---|---|---|
| Factor | Alive | Dead | P | Alive | dead | P |
| PLT | 202.80 ± 108.63 | 225 ± 115.96 | 0.786 | 231.34 ± 125.59 | 161.54 ± 47.67 | 0.021 |
| ESR | 52.29 ± 41.88 | 42.50 ± 10.61 | 0.752 | 60.45 ± 39.52 | 69.10 ± 33.54 | 0.553 |
| WBC | 6.68 ± 3.54 | 6.65 ± 2.33 | 0.989 | 8.31 ± 4.39 | 6.90 ± 2.68 | 0.300 |
| RDW-CV | 13.58 ± 0.57 | 13.50 ± 0.71 | 0.844 | 14.20 ± 1.73 | 13.72 ± 0.60 | 0.223 |
| RDW-SD | 41.61 ± 2.16 | 38.70 ± 0.14 | 0.077 | 44.70 ± 6.00 | 42.78 ± 2.37 | 0.299 |
| NEUT | 73.02 ± 9.54 | 84.35 ± 2.33 | 0.117 | 76.36 ± 11.70 | 81.75 ± 11.90 | 0.216 |
| NLR | 4.20 ± 1.89 | 7.72 ± 3.56 | 0.028 | 7.26 ± 7.00 | 8.50 ± 5.37 | 0.607 |
| LYMP | 20.36 ± 7.57 | 12.15 ± 5.30 | 0.154 | 18.23 ± 10.97 | 15.20 ± 9.16 | 0.402 |
| NLR and RDW-SD | 0.73 ± 1.10 | -0.41 ± 0.35 | 0.165 | 2.48 ± 3.13 | 1.63 ± 1.37 | 0.402 |
| NLR and RDW-CV | 1.06 ± 0.75 | 1.33 ± 1.15 | 0.649 | 2.07 ± 2.21 | 1.59 ± 0.96 | 0.502 |
Table 5: ROC analysis for significant factors.
| 95%CI of AUC | |||||
|---|---|---|---|---|---|
| Factors | AUC | SE | P | LL | UL |
| NEUT in female patients | 0.917 | 0.055 | 0.002 | 0.808 | 1.000 |
| NLR in female patients | 0.897 | 0.063 | 0.004 | 0.773 | 1.000 |
| NEUT in all patients | 0.739 | 0.800 | 0.009 | 0.581 | 0.896 |
| NLR in all patients | 0.696 | 0.082 | 0.033 | 0.535 | 0.857 |
Table 6: Comparison of the CRP grade between recovered and deceased patients..
| CRP grade | Alive n (%) | Dead n (%) | P |
|---|---|---|---|
| 0 | 4 (8.9) | 1 (6.7) | 0.873 |
| Weak Positive | 2 (4.4) | 0 (0) | |
| 1+ | 17 (37.8) | 3 (20) | |
| 2+ | 18 (40) | 6 (40) | |
| 3+ | 2 (4.4) | 1 (6.7) |

Discussion
In the current study, hematologic and biochemical parameters and their relationship to clinical outcome were evaluated in a cohort of Iranian COVID-19 patients. Our findings, NEUT, NLR, LYMP, as well as PLT could predict the prognosis of COVID-19. We found that advanced age was associated with worsening outcome. Previous studies have also suggested that older patients are at higher risk of fatal complications. No difference was found between patients’ gender and clinical outcome in our cohort.
A previous systematic review study suggested that increased total WBC and NLR, often driven by elevated neutrophils, were associated with poor prognosis in patients. They proposed the hypothesis that SARS-COV2 infection probably leads to increased formation of neutrophilic extracellular traps in the airways, which in turn initiate and propagate inflammation and thrombosis and therefore exacerbate the outcome. Previous studies also reported elevated NLR to be associated with poor clinical outcomes in other viral infections. They found that four subtypes of lymphocytes, including NK cell, B cell, TCD4+, and TCD8+ were all significantly decreased in deceased patients. Likewise, they reported that decreased PLT count conferred a poor prognosis. They found no remarkable difference between eosinophil count, monocyte count, or hemoglobin levels between the two groups [28]. Similarly we showed that higher levels of NEUT and NLR were associated with poor prognosis in total population. Besides, decreased PLT and lymphopenia were associated with adverse outcomes in patients older than 60 years and females, respectively.
According to Javanian et al study, high WBC was associated with poor disease prognosis. Moreover, a significant decrease in LYMP was observed in the deceased group, whereas Eos, PLT, and Hb did not show any correlation with the clinical outcome. In another study, Lingli Li et al. proposed that although total WBC was not associated with disease outcome, elevated NEUT and NLR, as well as decreased LYMP, were correlated with poor prognosis. They also did not observe any significant difference in hemoglobin levels between the survivors and non-survivors [29-30]. Lower Na levels were significantly associated with poor prognosis in our study. Likewise, a meta-analysis study by Yi Luo et al. showed that the mean serum sodium concentration in critical patients was remarkably lower than those with mild or moderate COVID-19. They proposed that low sodium concentration may be a result of the aging process which may lead to ACE2 over expression and higher mortality. They also suggested providing therapeutic sodium supplementation to reduce the progression of severe complications. Correspondingly, Javanian et al. found an association between hyponatremia and poor prognosis [29,31]. Regarding Creatinine and Potassium, theyreported no significant difference between the recovered and deceased groups. Likewise, we did not find any relationship between these parameters and COVID-19 outcome. In contrast, Lingli Li et al. found that although Creatinine was not associated with disease outcome, BUN was significantly associated with a poor prognosis. Further studies are suggested concerning the relationship between BUN and prognosis of COVID-19 [29-30]. The successful use of anti-inflammatory drugs in the treatment of patients highlights the key importance of inflammation in the progression of COVID-19. However, the role of inflammatory markers as prognostic indicators is still disputable [32].
In terms of CRP, a study by Chen et al. showed there is no statistically significant relationship between CRP levels and disease severity. Similarly, in our study, CRP and ESR were shown to be higher in COVID-19 patients, but the difference between the recovered and deceased patients was not statically significance. Contraversly, some studies have shown an association between b CRP and ESR with COVID-19 severity [30, 32-33]. However, studies with larger populations will be able to better identify the prognostic importance of laboratory parameters in COVID-19.
Conclusion
We found that older age, increased NEUT and NLR levels, and decreased Na, LYMP and PLT levels were associated with an increased risk of mortality in COVID-19 patients. We recommend that clinicians pay special attention to these biomarkers during the treatment procedure of patients. However, to obtain more conclusive results, we suggest further studies with larger populations in different ethnic groups.
Declarations
Acknowledgments: The authors would like to thank our colleagues in Shahid Beheshti Hospital, Ardestan, Iran.
Conflict of interest: The authors declare that there is no conflict of interest.
Compliance with ethical standards: The current study was approved by the Ethical Committee of Iran University of Medical Sciences and conformed to the provisions of the Declaration of Helsinki (Ethical code: IR.IUMS.REC 1397.32576).
References
- Peeri NC, Shrestha N, Rahman MS, Zaki R, Tan Z, Bibi S, et al. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned?. International journal of epidemiology. 2020.
- Usul E, Şan İ, Bekgöz B, Şahin A. The role of hematological parameters in COVID-19 patients in the emergency room. Biomarkers in Medicine. 2020.
- De Oliveira Toledo SL, Nogueira LS, das Graças Carvalho M, Rios DR, de Barros Pinheiro M, et al. COVID-19: Review and hematologic impact. Clinica Chimica Acta. 2020; 510: 170-176.
- Terpos E, Ntanasis‐Stathopoulos I, Elalamy I, Kastritis E, Sergentanis TN, et al. Hematological findings and complications of COVID‐19. American journal of hematology. 2020.
- Cai Q, Huang D, Yu H, Zhu Z, Xia Z, et al. COVID-19: Abnormal liver function tests. Journal of hepatology. 2020.
- Benedetti C, Waldman M, Zaza G, Riella LV, Cravedi P, et al. COVID-19 and the Kidneys: An Update. Frontiers in medicine. 2020; 7.
- Chen HJ, Qiu J, Wu B, Huang T, Gao Y, Wang ZP, et al. Early chest CT features of patients with 2019 novel coronavirus (COVID-19) pneumonia: Relationship to diagnosis and prognosis. European Radiology. 2020; 1.
- Francone M, Iafrate F, Masci GM, Coco S, Cilia F, Manganaro L, et al. CT score in COVID-19 patients: correlation with disease severity and short-term prognosis. European radiology. 2020; 1-0.
- Callender LA, Curran M, Bates SM, Mairesse M, Weigandt J, Betts CJ, et al. The Impact of Pre-existing Comorbidities and Therapeutic Interventions on COVID-19. Frontiers in Immunology. 2020; 11.
- Pourbagheri-Sigaroodi A, Bashash D, Fateh F, Abolghasemi H. Laboratory findings in COVID-19 diagnosis and prognosis. Clinica Chimica Acta. 2020.
- Garcia PD, Fumeaux T, Guerci P, Heuberger DM, Montomoli J, et al. Prognostic factors associated with mortality risk and disease progression in 639 critically ill patients with COVID-19 in Europe: Initial report of the international RISC-19-ICU prospective observational cohort. EClinical Medicine. 2020; 100449.
- Khartabil TA, Russcher H, van der Ven A, de Rijke YB, et al. A summary of the diagnostic and prognostic value of hemocytometry markers in COVID-19 patients. Critical reviews in clinical laboratory sciences. 2020; 57: 415-431.
- Elshazli RM, Toraih EA, Elgaml A, El-Mowafy M, El-Mesery M, et al. Diagnostic and prognostic value of hematological and immunological markers in COVID-19 infection: A meta-analysis of 6320 patients. PloS one. 2020; 15: e0238160.
- Lippi G, Plebani M. Laboratory abnormalities in patients with COVID-2019 infection. Clinical Chemistry and Laboratory Medicine (CCLM). 2020; 58: 1131-1134.
- Wang C, Deng R, Gou L, Fu Z, Zhang X, et al. Preliminary study to identify severe from moderate cases of COVID-19 using combined hematology parameters. Annals of translational medicine. 2020; 8.
- Zhou F, Yu T, Du R, Fan G, Liu Y, et al. Clinical course and risk factors for mortality of adult in patients with COVID-19 in Wuhan, China: a retrospective cohort study. The lancet. 2020.
- Fan BE, Chong VC, Chan SS, Lim GH, Lim KG, et al. Hematologic parameters in patients with COVID‐19 infection. American journal of hematology. 2020; 95: E131-E134.
- He L, Qin R, Yang Z, Jia N, Chen R, Xie J, et al. Identification of immunological, inflammatory, hematological, and coagulation abnormalities associated with severity and mortality of COVID-19: A meta-analysis of 64 observational studies.
- Javanian M, Bayani M, Shokri M, Sadeghi-Haddad-Zavareh M, Babazadeh A, et al. Clinical and laboratory findings from patients with COVID-19 pneumonia in Babol North of Iran: a retrospective cohort study. Romanian Journal of Internal Medicine. 2020 May 11; 1(ahead-of-print).
- Li L, Yang L, Gui S, Pan F, Ye T, et al. Association of clinical and radiographic findings with the outcomes of 93 patients with COVID-19 in Wuhan, China. Theranostics. 2020; 10: 6113.
- Luo Y, Li Y, Dai J. Low blood sodium increases risk and severity of COVID-19: a systematic review, meta-analysis and retrospective cohort study. Med Rxiv. 2020.
- Zeng F, Huang Y, Guo Y, Yin M, Chen X, et al. Association of inflammatory markers with the severity of COVID-19: A meta-analysis. International Journal of Infectious Diseases. 2020.
- Chen L, Liu HG, Liu W, Liu J, Liu K, et al. Analysis of clinical features of 29 patients with 2019 novel coronavirus pneumonia. Zhonghua jie he he hu xi za zhi= Zhonghua jiehe he huxi zazhi= Chinese journal of tuberculosis and respiratory diseases. 2020; 43: E005.