
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A case of Helcococcus kunzii infection
Xiang Wang; Jinhong Zhao; Zuozhou Xie; Zhenghua Zhu; Chen Yang, Yi Liu*
Department of Pulmonary and Critical Care Medicine, The Second People’s Hospital of Kunming, Kunming, China.
*Corresponding Author : Yi Liu
Department of Pulmonary and Critical Care Medicine, The Second People’s Hospital of Kunming, Kunming, China.
Email: Liuyi714@126.com
Received : Sep 10, 2022
Accepted : Oct 10, 2022
Published : Oct 17, 2022
Archived : www.jcimcr.org
Copyright : © Yi Liu (2022).
Abstract
Helcococcus is a resident bacteria in human and animal skin. It is a rare opportunistic pathogen in humans. Helcococcus kunzii, which causes mainly skin infection, was first discovered by Collins in 1993 [1]. At present, there are few case reports of infection caused by Helcococcus kunzii. Here, we report a case of Helcococcus kunzii infection admitted to our department, to increase the understanding of its diagnosis and treatment in the clinic.
Keywords: Helcococcus kunzii; mNGS; Antibiotic therapy; Incision drainage.
Citation: Wang X, Zhao J, Xie Z, Zhu Z, Liu Y, et al. A case of Helcococcus kunzii infection. J Clin Images Med Case Rep. 2022; 3(10): 2104.
Case presentation
A 39-year-old man was admitted to the hospital on July 29, 2022, with “skin swelling of the left lower extremity, multiple blisters, ruptured left little toe, and 3 days fever”. The patient’s left lower limb was scratched by an object while fishing by the river on July 26. The affected skin was swollen, and multiple blisters quickly appeared. The left fourth and fifth toes were ulcerated and purulent. Furthermore the patient developed a fever accompanied by chills and weakness. The highest reported temperature was 39.5oC. Oral antipyretic drugs were not effective. The patient presented to the local hospital for treatment on July 28, with persistent high fever, which did not reduce even after intravenous antibiotics (“cephalosporin)”.
On July 29, the patient’s temperature was 39.0oC, and he was transferred to our hospital for further diagnosis and treatment. The patient had a long history of alcohol consumption, approximately 300 mL to 500 mL daily. Physical examination results on admission were: temperature: 39.8oC, pulse: 123 bpm, respiration: 33 bpm, and blood pressure: 85/55 mmHg. The patient was acutely febrile and conscious. Cyanosis was apparent. Slightly coarse breath sounds were detected in both lungs. A 10 cm × 5 cm soft and tender mass was palpable in the left inguinal area. Swelling of the left lower limb below the knee joint and numerous blisters, measuring 2 cm - 3 cm, were evident. The affected area showed local skin redness, ulceration, and swelling, which was accompanied by severe pain. The skin temperature of the distal limb of the left knee joint was cold. The superficial sensation of the extremities of the left fourth and fifth toes was decreased. A subcutaneous ecchymosis was observed in the left thigh. The activity of the left lower limb was limited and the skin tension was increased. A wound, 2 cm in length, was observed in the anterior tibia of the left lower limb, and yellow purous discharge was observed in the space between the fourth and fifth toes of the left foot (Figure 1).The results of a routine blood test on July 29 are as follows. White blood cell count: 14.2 × 109/L. Platelet count: 91 × 109/L. C-Reactive Protein (CRP): 178.6 mg/L. Procalcitonin (PCT): 14.39 ng/mL. Interleukin-6 (IL-6): 1197.04 pg/mL. The superficial lymph node ultrasound highlighted the lymph nodes in the left groin, and some of them were enlarged. Reactive hyperplasia was considered. The dorsal foot ultrasound demonstrated edema and thickening of the subcutaneous soft tissue of the left dorsal foot. No abnormal sonography was found in the blood vessels of both lower extremities. The diagnoses on admission were: 1. necrotizing fasciitis of the left lower limb and 2. septic shock. Considering the severe infection and rapid disease progression of the patient, peripheral blood and fluids from the affected area were sampled for Metagenomics Next -Generation Sequencing (mNGS) and common culture. Empirical antibiotics (cefoperazone-sulbactam and levofloxacin) were commenced. On July 30, the patient was still febrile,with a peak temperature of 39.4oC. Results from routine blood examinationwere as follows. White blood cell count: 12.60 × 109/L. Platelet count: 82 × 109/L. Liver function: alanine aminotransferase, 243 U/L, aspartate aminotransferase, 389 U/L. Total protein: 58.46 g/L. Albumin: 35.36 g/L. Erythrocyte sedimentation rate: 25 mm. Renal function: creatinine, 275.4 mol/L and lactic acid: 5.8 mmol/L. The skin tension of the patient’s left lower extremity was higher than that at admission. A 4 cm × 4 cm tension blister was seen on the back of the left foot (Figure 2), and a 4 cm × 2 cm blister was seen below the ankle joint in the left lower extremity. After surgical consultation, incision, and drainage of the abscess in the fascial space of the left foot were performed (Figure 3). Helcococcus kunzii and Streptococcus pyogenes were identified from the blood (Figure 4) and secretion (Figure 5) samples. Considering the patient’s history of river fishing and left lower limb scratches, as well as the identification of Helcococcus kunzii as the main pathogenic bacteria, considering Helcococcus Kunzii as the main pathogenic bacteria, the diagnoses were updated: 1. Necrotizing fasciitis of the left lower extremity due to Helcococcus kunzii, 2. Helcococcus kunzii sepsis, 3. impaired liver function, 4. acute kidney injury. Mean while, the patient’s peak temperature decreased and the infection markers also decreased. As the treatment was effective, cefoperazone-sulbactam plus and levofloxacin were continued. On July 31, the patient’speak temperature dropped to 38.2oC and his chills resolved. Peripheral T lymphocyte subsets showed CD3+ cells/lymphocytes of 70%, CD3+CD4+T cells/lymphocytes of 24%, CD3+CD8+T cells/lymphocytes of 44%, and the ratio of CD3+CD4+T cells /CD3+CD8+T cells was 0.55. On August 1, the patient’s temperature measured 37.7oC. Results from routine blood examination were as follows. White blood cell count: 8.9 × 109/L. Platelet count: 126 × 109/L. CRP: 146.5 mg/L. PCT: 10.14 ng/mL. IL-6: 36.29 pg/mL. On August 2, the peak temperature measured 37.5oC. Swelling of the left lower extremity also improved. Moreover, the skin tension of the left dorsum of the foot was decreased. There was no purulent discharge from the incision of the left dorsum of the foot and discharge from the left toe space was reduced. The patient’s temperature was normal on August 3. On August 4, both blood and wound secretion cultures were negative. Results from routine blood tests on August 5 showed a white blood cell count of 8.7×109/L, platelet count of 245 × 109/L, CRP of 15.2 mg/L, PCT of 1.33 ng/mL, and IL-6 of 7.10 pg/mL. Redness, swelling, heat, and pain subsided from the patient’s left lower limb. No secretions were found in the left toe space and there was no obvious exudation or bleeding on the left foot dressing. The patient requested to be transferred to the local hospital for further treatment. He was discharged from our hospitalon August 6.
Discussion
In 1993, British scholar, Collins, during the clinical separation of some gas “aureus”with undetermined taxonomic status which presented as catalase enzyme-negative and Gram-positive cocci, proposed a possible new species. After the16s rRNA sequence homology, Collins suggested that these bacteria had the low G+C content of Gram-positive bacteria, and thus, proposed the new bacteria genus of Helcococcus. Currently, Helcococcus has five species, namely, Helcococcuskunzii, Helcococcus ovis, Helcococcus pyogenica, Helcococcus sueciensis, and Helcococcus seattlensis [2], Helcococcus kunziiis one of the most common species [3-6]. As Gram-positive, facultative, anaerobic, non-sporulating cocci, Helococcus kunzii are arranged in couplets, tufted, and with no power [7].



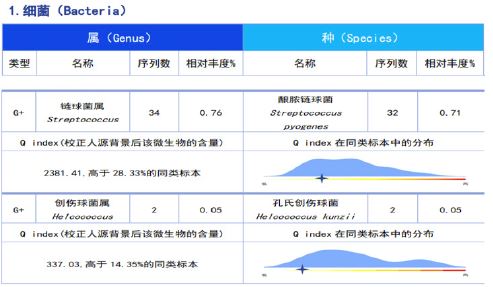

Table 1: Infection markers over time.
| July 29 | July 30 | August 1 | August 5 | |
|---|---|---|---|---|
| White blood cell count (×109/L) | 14.2 | 12.6 | 8.9 | 8.7 |
| Platelet count (×109/L) | 91 | 82 | 126 | 245 |
| Neutrophil percentage (%) | 87.63 | 89.28 | 80.81 | 65.21 |
| Neutrophil count (×109/L) | 12.404 | 11.249 | 7.202 | 5.648 |
| Lymphocyte percentage (%) | 7.88 | 7.74 | 13.40 | 23.20 |
| Lymphocyte count (×109/L) | 1.116 | 0.975 | 1.194 | 2.009 |
| CRP (mg/L) | 178.6 | 146.5 | 15.2 | |
| PCT (ng/mL) | 14.39 | 10.14 | 1.33 | |
| IL-6 (pg/mL) | 1197.04 | 36.29 | 7.10 |
Helcococcus kunzii is a resident bacteria in human and animal skin, especially in the lower limbs. Helcococcus kunzii can cause a variety of opportunistic infections, often occurring in patients with underlying diseases-(diabetes, hypertension)or immune deficiency (chronic alcohol consumption, malignancy) [8]. Our patient has a long history of drinking. The peripheral blood T lymphocyte subsets confirmed immune deficiency. There was a history of injury to the left foot after fishing by the river (the skin was scratched by an object). Subsequently, his left leg swelled, local tension increased, tension blisters appeared on the left foot, and the blood and secretion mNGS detected Helcococcus kunzii. Thus, Helcococcus kunzii infection was established.
In the cases of Helcococcus kunzii infection reviewed by Caliend [9], other strains were detected in all specimens at the same time, including Staphylococcus aureus and Enterobacteriaceae. The blood and secretion mNGS from our patient identified Helcococcus kunzii and Streptococcus pyogenes, which is consistent with the co-existence of Helcococcus kunzii and other pathogens. At present, there are few case reports of Helcococcus kunzii infection worldwide. To date, only 2 cases have been reported in China, including 1 case of breast abscess and 1 case of the diabetic foot [10,11]. This patient was the first case of Helcococcus kunzii infection diagnosed by mNGS in China. The common blood culture and wound secretion culture were negative. The diagnosis of Helcococcus kunzii infection was finally verified by mNGS.
Helcococcus kunzii resistance to the antibiotics used to treat the infection, including trimethoprim sulfamethoxazole, macrolides, clindamycin, fluoroquinolones, aminoglycosides, and penicillin have been reported [12]. The clinical symptoms of our patient, a middle-aged man with immune deficiency, were relieved significantly after cefoperazone-sulbactam and levofloxacin. Following treatment, the infection markers were reduced, which confirmed the effectiveness of this combination of antibiotics. This treatment plan has a certain reference value for the clinical treatment of future cases.
Katrin [13]. Pointed out that any infected wound requires appropriate surgical debridement. Timely correct use of antibiotics combined with surgical removal of the necrotic tissues can greatly reduce the risk of amputation and mortality. The patient’s left leg was inflamed, hot, and painful. The local tension increased. The left foot quickly developed tension blisters. On the second day of admission, the patient’s left foot fascia space abscess was incised and drained, followed by, postoperative wound irrigation with hydrogen peroxide and physiological saline, and dressed with 0.5% iodine volts gauze hydropathin compress. After treatment, the patient’s left lower limb swelling, heat, and pain subsided, and the partial tension returned to normal. In this case, early surgical debridement combined with wound dressing led to significant clinical improvement of a for local abscess caused by Helcococcus kunzii.
The successful treatment of this patient with Helcococcus kunzii infection can be summarized as follows [1]. Early diagnosis of Helcococcus kunzii infection was made according to the patient’s history and clinical manifestations [2]. As a new precision medicine technology, mNGS was advantageous for the detection of rare pathogens, and was superior to common culture [3]. For immunodeficient patients, the possibility of opportunistic disease caused by a resident bacteria must be considered [4]. After the diagnosis was ascertained, sensitive antibiotics must be administered promptly [5]. For wound abscesses, early incision and drainage is recommended to prevent further expansion of the wound and maximize the preservation of limb function and the patient.
Funding: This study was supported by a Health Research Project of the Kunming Municipal Health Committee (grant number 2020-03-02-117).
References
- MD Collins, RR Facklam, UM Rodrigues, KL Ruoff. Phylogenetic analysis of some Aerococcus-like organisms from clinical sources: Description of Helcococcus kunzii gen. nov., sp. nov.[J]. International journal of systematic bacteriology. 1993; 43: 425-429.
- Siu-Kei, Chow, Jill E, Clarridge. Identification and clinical significance of Helcococcus species, with description of Helcococcus seattlensis sp. nov. from a patient with urosepsis.[J]. Journal of clinical microbiology. 2014; 52.
- Vergne A, Guerin F, Lienhard R, Le Coustumier A, Daurel C, et al. Identification and clinical significance of Helcococcus kunzii in human samples. J Clin Microbiol. 2015; 53: 2703–2705.
- Farid S, Miranda W, Maleszewski J, Sohail MR. Helcococcus kunzii prosthetic valve endocarditis secondary to lower extremity cellulitis. BMJ Case Rep. 2017; https://doi.org/10.1136/bcr-2017-219330.
- Lotte R, Lotte L, Degand N, Gaudart A, Gabriel S, et al. Infectious endocarditis caused by Helcococcus kunzii in a vascular patient: a case report and literature review. BMC Infect Dis. 2015; 15: 238.
- Ngba Essebe C, Visvikis O, Fines Guyon M, Vergne A, Cattoir V, et al. Decrease of Staphylococcus aureus virulence by Helcococcus kunzii in a Caenorhabditis elegans model. Front Cell Infect Microbiol. 2017; 7: 77.
- Margarida, Mouro, João, Frade, Catarina, Chaves, Jorge, Velez. Helcococcus kunzii, a skin-colonising microorganism with pathogenic capacity: A case of polymicrobial intracranial empyema.[J]. BMJ case reports. 2021; 14.
- Li Jinzhong. Research progress of nucleococcus. Chinese Tropical Medicine. 2009; 9(7): 1375-1377.
- AM Caliendo, CD Jordan, KL Ruoff. Helcococcus, a new genus of catalase-negative, gram-positive cocci isolated from clinical specimens.[J]. Journal of clinical microbiology. 1995; 33: 1638.
- Guo Fengli, Zhou Youquan, Li Wencong, Hu Liya. A case of mammary gland abscess caused by V. konzi[J]. Journal of Clinical Laboratory. 2015; 33(6): 480. DOI:10.13602/j.cnki.jcls.2015.06.25.
- Hou Chenrui, Rong Jianrong, Song Jing, Han Yaping, Li Ziyang, Li Xia, Zhang Xiaohui, Gao Chunyan, Dong Yiran, Wang Ruixue. A case of traumaticococcus konzi in a patient with diabetic foot [J].Chinese Journal of Clinical Infectious Diseases.
- Siddharth, Sridhar, Jasper F W, Chan, Kwok-Yung, Yuen. First report of brain abscess caused by a satelliting phenotypic variant of Helcococcus kunzii.[J]. Journal of clinical microbiology. 2014; 52: 370-373.
- Katrin M, Stanger, Frauke, Albert, Ulrich, Kneser, et al. Management of chronic osteomyelitis of the tibia with life-threatening complications under negative pressure wound therapy and isolation of Helcococcus kunzii.[J]. International wound journal. 2015; 2: 443-446.