
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 3
A case series assessing relationship between active motions and stereognosis in cerebral palsy
Hank White1*; Joel Eastman1; Sam Augsburger1; Scott Riley2; Henry Iwinski2
1Motion Analysis Center, Shriners Children’s Lexington, 110 Conn Terrace, Lexington, KY 40508, USA.
2Shriners Children’s Lexington, 110 Conn Terrace, Lexington, KY 40508 and University of Kentucky Department of Orthopaedic
Surgery and Sports Medicine, 740 S. Limestone Street, Lexington, KY 40536, USA.
*Corresponding Author : Hank White
Motion Analysis Center, Shriners Children’s Lexington, 110 Conn Terrace, Lexington, KY 40508, USA.
Ph: (859) 266-2101;
Email: hwhite@shrinenet.org
Received : Sep 10, 2022
Accepted : Oct 10, 2022
Published : Oct 17, 2022
Archived : www.jcimcr.org
Copyright : © White H (2022).
Keywords: Cerebral palsy; Upper extremity; Kinematics; Stereognosis.
Abbreviations: CP: Cerebral Palsy; MACS: Manual Ability Classification System; AROM: Active Range Of Motion.
Citation: White H, Eastman J, Augsburger S, Riley S, Iwinski H, et al. A case series assessing relationship between active motions and stereognosis in cerebral palsy. J Clin Images Med Case Rep. 2022; 3(10): 2105.
Introduction/background
Cerebral Palsy (CP) is an umbrella term used to describe a permanent disability resulting from non-progressive damage to the brain, specifically the corticospinal tract, of a developing fetus or infant. CP is believed to be caused by a malformation of the brain during its development and is a common pediatric disorder with about two to three cases occurring out of every thousand births. Children with CP experience a range of impairments including muscle weakness, sensory deficits, increased muscle spasticity, and upper limb dysfunction [1]. All of these interfere with a child’s motor function resulting in a reduction in their ability to interact effectively with their environment, decreases in the child’s daily self-care activities, as well as developmental nonuse, especially of the upper limbs [2]. In the past, treatment for unilateral CP has had a strong focus on correcting motor impairments such as muscle weakness and/or spasticity [3]. Recently, a shift in focus towards investigating the effects of assessing and improving tactile dysfunction in the upper limbs since findings have reported that the prevalence of sensory processing impairments in children with hemiplegia are up to 75% or more [4]. To date, there is a lack of research assessing the relationship between Active Range of Motion (AROM) and sensory processing (tactile discrimination) deficits. Therefore, the purpose of this study is to determine if there is a relationship between active AROM and tactile discrimination for children previously diagnosed with unilateral CP.
Methodology
This is an IRB approved retrospective study. Potential participants were previously evaluated for a clinical assessment of upper extremity functions in the motion analysis center between August 2014 and July 2021. Inclusion criteria were: Patients with the primary diagnosis of cerebral palsy, spastic hemiplegia, ages 7-21 years old at the time of the evaluation. Patients performed clinical assessment of active range of motion and Stereognosis assessments during one clinic visit. Exclusion criteria were: Patients who had undergone botulinum toxin injections in the past 6 months or surgical interventions in the past 12 months.
During the clinical assessment, each patient underwent a history and evaluation by a physical therapist and then performed active range of motion assessment using seventeen [17] surface reflective markers placed on each upper extremity and three-dimensional motion analysis system (optical tracking system). This is similar to the technology used in the movie and video game industries, a motion capture system uses multiple digital cameras linked together to a computer, simultaneously measuring the movement of reflective markers attached to the skin [5,6]. Using these imbedded coordinate systems and Euler rotations, resulting angles describe the rotation of one segment relative to an adjacent segment [7]. A six degree of freedom model is created from each body segment. Each segment is free to translate and rotate independently of other body segments [7].
Twelve 3-D motion capture cameras (Vicon Vantage Cameras, Nexus 2.12.1 software, Culver City, CA) were used for data collection and post processing. Three trials of active range of motion (wrist flexion/extension and forearm pronation/supination), first with their uninvolved and then their involved arm were averaged. Reflective markers were placed on the following anatomical landmarks: Left scapula (offset), bilateral lateral humeral head, lateral mid-humerus, lateral humeral epicondyle, mid-forearm in line with thumb, radial styloid process, ulnar styloid process, middle finger proximal phalange base and head. Radial and ulnar markers, bisecting the wrist, were placedso little to no motion can be detecting in the markers when supinating and pronating.
The patients were seated on height adjustable bench so both feet could be flat on the floor. Patients performed three trials of active range of motion first with their uninvolved and then their involved arm. These motions performed were maximum wrist extension and flexion (with finger flexion/extension), and active forearm supination and pronation. Maximum and minimum values for flexion/extension and pronation/supination were analyzed using Visual 3D software (Version 6, C-Motion, Inc., Germantown, MD).
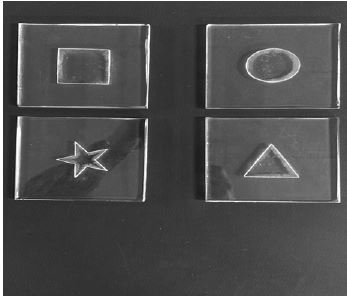
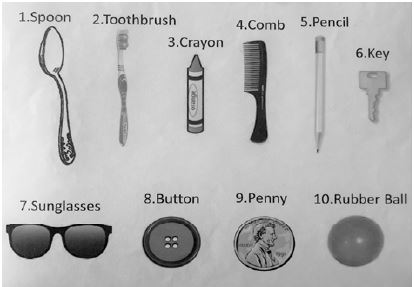
After removal of reflective markers, regardless of which arm is more involved, patients performed stereognosis assessment first with their right upper extremity and then with their left. Stereognosis assessment consisted of patient sitting in a chair and then placing their hand on a bedside table. Attached to the bedside table was a small curtain to prevent the patient from seeing the objects and shapes. Five different objects and four different shapes were placed under the patient’s hand (Figures 1 & 2). Patients were allowed to actively and freely touch objects and shapes for up to 5 seconds before naming. Patients were provided a diagram of objects and shapes and were asked to identify the object under their hand (Figures 3 & 4). Patient then received a score of 0 (incorrect) or 1 (correct identification) of each object and shape. Patients were not allowed to see the object or shapes at any time. Therapist did not inform patient if their answers were correct or incorrect.
Statistical analyses were performed with SPSS 26.1. Descriptive statistics and Spearman’s rank correlation coefficients between AROM and stereognosis scores were calculated.


Results
Sixty-two patients (26 females) met inclusion criteria. A majority (82%) of participants had Manual Ability Classification System (MACS) score of II, with the remaining 14 % score of I and 3 % score of III. Per family report, 50 (81 %) of the patients performed activities of daily living with one hand.
On average, the uninvolved arms demonstrated higher rates of correct identification of shapes and objects (p< 0.001). The uninvolved arms demonstrated more wrist (p< 0.001) and finger extension (p=0.002), and total excursions (p< 0.001) compared to involved arms. Uninvolved arms demonstrated more pronation (p=0.004), supination (p< 0.001) and total excursions (p< 0.001) compared to involved arms. (Table 1)
Table 1: Uninvolved and Involved arms means and standard deviations with p value of paired t-tests for stereognosis scores, wrist, finger and forearm active range of motions.
| Parameters | Uninvolved Arm Mean (Standard Deviation) | Involved Arm Mean (Standard Deviation) | p-value |
|---|---|---|---|
| Stereognosis Score of Correct Identified Shapes and Objects (%) | 87.3 (17.3) | 43.5 (33.4) | < 0.001 |
| Maximum Wrist Extension (°) | 74.6 (11.4) | 19.4 (34.2) | < 0.001 |
| Maximum Wrist Flexion (°) | 46.3 (10.4) | 45.0 (14.7) | 0.271 |
| Total Wrist Excursion (°) | 120.9 (14.3) | 64.4 (34.3) | < 0.001 |
| Maximum Finger Extension (°) | -20.1 (13.4) | -27.6 (16.2) | 0.002 |
| Maximum Finger Flexion (°) | 55.9 (15.3) | 55.3 (16.5) | 0.388 |
| Total Finger Excursion (°) | 35.8 (14.0) | 27.8 (13.5) | < 0.001 |
| Maximum Forearm Pronation (°) | 55.5 (15.2) | 49.9 (18.2) | 0.004 |
| Maximum Forearm Supination (°) | 69.4 (16.5) | 8.5 (36.9) | < 0.001 |
| Total Forearm Excursion (°) | 125.0 (23.4) | 58.4 (33.4) | < 0.001 |
Because correct identification of shapes and objects demonstrated strong correlation (r = .826), stereognosis scores are reported as a percent of total correct indemnifications for nine items. No relationship was observed between stereognosis scores and active range of motion for the uninvolved arms. For the involved arms, stereognosis score was moderately correlated with MACS (r = -.438). Stereognosis scores were moderately correlated with maximum wrist extension (r = .472) and total wrist excursion (r = .523). Weak correlations were observed between stereognosis scores and other AROM of fingers and forearms (Table 2).
Table 2: Spearman’s rho correlations coefficients of the involved arms for MACS, stereognosis scores, wrist, finger and forearm active range of motions. (N=62)
| Variables | (1) | (2) | (3) | (4) | (5) | (6) | (7) | (8) | (9) | (10) |
|---|---|---|---|---|---|---|---|---|---|---|
| (1) MACS | ||||||||||
| (2) Stereognosis Score | -.438 | |||||||||
| (3) Wrist Maximum Extension | -.282 | .472 | ||||||||
| (4) Wrist Maximum Flexion | .158 | -.155 | .173 | |||||||
| (5) Wrist Total Excursion | -.331 | .523 | .894 | -.198 | ||||||
| (6) Finger Maximum Extension | .099 | -.018 | -.055 | -.199 | .083 | |||||
| (7) Finger Maximum Flexion | .241 | -.262 | -.390 | .014 | -.357 | .676 | ||||
| (8) Finger Total Excursion | -.151 | .289 | .463 | -.290 | .615 | .357 | -.388 | |||
| (9) Forearm Maximum Pronation | -.144 | .121 | -.122 | -.192 | -.030 | -.073 | -.190 | .086 | ||
| (10) Forearm Maximum Supination | .238 | -.234 | -.494 | -.081 | -.487 | -.146 | .004 | -.239 | .350 | |
| (11) Forearm Total Excursion | -.301 | .329 | .532 | .015 | .554 | .135 | -.112 | .348 | .026 | -.893 |
Discussion
In 1958 Tachdjian & Minear reported sensory disorders were present in 42% of children diagnosed with CP [8]. The most common deficits were stereognosis, two-point discrimination and position sense. It is not until the last decade that studies have assessed sensory disorders for persons diagnosed with cerebral palsy for a renewed focus on the concept that cerebral palsy is a sensory and motor disorder. In their 2021 review of the literature Brun et al. reported all 20 studies consistently demonstrated a decrease in spatial tactile perception for CP populations [9]. Specifically, deficits in stereognosis, graphesthesia and two-point discrimination. Additionally, impairments in tactile perception were almost systematic, while impairments of proprioception and pain were more heterogenous across CP populations [9].
Russo et al. used structural equation model to assess the relationships between self-care and upper extremity impairments (spasticity, sensory function, and manual abilities) for children with hemiplegia [1]. In that study, self-care was directly affected by manual abilities and processing skills with indirect effects of sensation. In our current study, we identified weak to moderate correlations between stereognosis and active range of motion.
Park et al. assessed the relationship between MACS level andsensory processing (sensory sensitivity) of children diagnosed with CP hemiplegia [10]. Weak negative correlations were reported. In our study, we observed moderate negative correlationsbeen MACS level and stereognosis scores. These differences could support premise that proprioception is heterogeneous across CP populations.
Study limitations
This study was limited to children diagnosed with cerebral palsy, hemiplegia. The majority of the participants were MACS level II which limits the ability to generalize the results of this study for children with CP. Additionally, the wide age ranges of participants could affect results of study because different developmental ages are represented. No cognitive tests were performed clinically; therefore, we could not assess the influence of cognitive skills. Four (6%) participants did not appear to understand stereognosis task because they scored less than 50% correct identification with their uninvolved sides. The dominant hand of each participant was not identified. However, previous work by Wingert et al. reported “classifying dominant side matched reported less involved side” for children with diplegia [11]. We did not provide any specific instructions regarding finger motions or wrist radial/ulnar deviation during AROM data collection. Which could have contributed to weak correlation of finger AROM and stereognosis scores. Lastly, because this was a retrospective study we did not report other extremity impairments, specifically, strength and spasticity because these were not consistently collected during each clinical visit.
Conclusion
The results of this study show that children with cerebral palsy, hemiplegia demonstrated weak and moderate relationships between stereognosis scores and with total wrist excursion and forearm excursions. Impaired stereognosis may contribute to decreased dexterity and fine motor skills. Thisimplies treatments to improve AROM may improve tactile discrimination abilities for persons diagnosed with CP. Future studies assessing relationships between stereognosis, AROM and functional abilities are warranted.
Declarations
Individual contribution of each author:
Hank White: Conceptualization, Methodology, Formal analysis, Investigation, Resources, Data acquisition, Project administration, Funding acquisition, Writing - Original Draft, Writing - Review & Editing
Joel Eastman: Investigation, Writing - Original Draft, Writing - Review & Editing.
Sam Augsburger: Conceptualization, Methodology, Software Programming, Funding acquisition, Visualization, Investigation, Supervision, Writing - Review & Editing.
Scott Riley: Conceptualization, Methodology, Funding acquisition, Writing - Review & Editing.
Henry Iwinski: Conceptualization, Methodology, Funding acquisition, Writing - Review & Editing.
Conflicts of interest and source of funding: None of the authors has a conflict of interest to report. This study was funded in part by Kosair Charities in Louisville, Kentucky.
Acknowledgements: Authors would like to thank Bobbie Edester, for her time and assistance in data collection, and processing.
References
- Russo RN, Skuza PP, Sandelance M, Flett P. Upper limb impairments, process skills, and outcome in children with unilateral cerebral palsy. Dev Med Child Neurol. 2019; 61: 1080-1086.
- Salkar P, Pazare S, Harle M. Effect of tactile stimulation on dexterity and manual ability of hand in hemiplegic cerebral palsy children. International Journal of Therapies and Rehabilitation Research. 2016; 6: 91-99.
- Auld ML, Boyd RN, Moseley GL, Johnston LM. Tactile assessment in children with cerebral palsy: A clinimetric review. Phys Occup Ther Pediatr. 2011; 31: 413-439.
- McLean B, Taylor S, Blair E, et al. Somatosensory Discrimination Intervention Improves Body Position Sense and Motor Performance in Children With Hemiplegic Cerebral Palsy. The American journal of occupational therapy: Official publication of the American Occupational Therapy Association. 2017; 71: 7103190060p7103190061-7103190060p7103190069.
- Baker R. Measuring Walking: A Handbook of Clinical Gait Analysis. Hoboken, New Jersey: Wiley; 2013.
- Whittle M. Whittle’s Gait Analysis. Oxford: Elsevier Ltd; 2012.
- Kadaba MP, Ramakrishnan HK, Wootten ME. Measurement of lower extremity kinematics during level walking. J Orthop Res. 1990; 8: 383-392.
- Tachdjian M, Minear W. Sensory Disturbances in the Hands of Children with Cerebral Palsy. J Bone Joint Surg Am. 1958; 40: 85-90.
- Brun C, Traverse E, Granger E, Mercier C. Somatosensory deficits and neural correlates in cerebral palsy: A scoping review. Dev Med Child Neurol. 2021; 63: 1382-1393.
- Park M. The Relationship between Sensory Processing Abilities and Gross and Fine Motor Capabilities of Children with Cerebral Palsy. J Korean Soc Phys Med. 2017; 12: 67-74.
- Wingert JR, Burton H, Sinclair RJ, et al. Tactile sensory abilities in cerebral palsy: Deficits in roughness and object discrimination. Dev Med Child Neurol. 2008; 50: 832-838.