
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
Lymphoepithelioma-like hepatocellular carcinoma, case report
of a rare indolent subtype of hepatic cancer
Rajalakshmi Govalan1; Rola Saouaf2; Maha Guindi3; Ju Dong Yang4*; Nicholas Nissen5
1Department of Medicine, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
2Department of Radiology, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
3Department of Pathology and Laboratory Medicine, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
44Samuel Oschin Comprehensive Cancer Institute, Comprehensive Transplant Center, Karsh Division of Gastroenterology and Hepatology, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
5Samuel Oschin Comprehensive Cancer Institute, Comprehensive Transplant Center, Cedars-Sinai Medical Center, Los Angeles, CA, USA.
*Corresponding Author : Ju Dong Yang, MD, MS
Medical Director, Liver Cancer Program, Assistant Professor of Medicine, Karsh Division of Gastroenterology and Hepatology, Cedars-Sinai Medical Center.
Health Sciences Assistant Clinical Professor of Medicine, University of California, Los Angeles, 8900 Beverly Blvd, Los Angeles, California, 90048.
Tel: 310-423-1971, Fax: 310-423-2356;
Email: judong.yang@cshs.org
Received : Sep 09, 2022
Accepted : Oct 10, 2022
Published : Oct 17, 2022
Archived : www.jcimcr.org
Copyright : © Yang JD (2022).
Abstract
Background: Lymphoepithelioma - Like Carcinomas (LELC) of the liver are tumors of poorly differentiated epithelial cells with prominent lymphoid cell infiltration of the stroma. Unlike common primary liver cancers, LELC is a rare subtype of primary liver cancer with notably better prognosis. Unfortunately, available data and understanding of this unique cancer type is limited.
Case report: A 72-year-old Hispanic female with compensated cirrhosis due to treatment-naïve hepatitis C and Primary Biliary Cirrhosis (PBC) presented with chronic abdominal pain. Computed Tomography scan (CT) of her abdomen at that time showed nodular liver with a mass measuring 4.6 x 3.7 cm in the right hepatic lobe with heterogeneous enhancement on arterial phase associated with mild venous washout, concerning for Hepatocellular Carcinoma (HCC). She was lost to follow up but re-presented 4 years later with an interval increase in the liver mass to 6.4 x 4.8 cm. Staging work up was unremarkable and patient underwent resection of the mass. Histopathologic examination showed moderately differentiated HCC with massive lymphocytic infiltration within the tumor with lymphocyte outnumbering tumor cells and diagnosed as lymphoepithelial-like carcinoma-HCC. The patient remained asymptomatic with no tumor recurrence at 16 months post resection.
Conclusion: This report of an indolent course of untreated EBV positive LELC-hepatocellular carcinoma provides valuable insight about this rare tumor type
Keywords: Lymphoepithelioma - like carcinomas; Liver cancer; EBV associated lel-hepatocellular carcinoma; Case report; Histopathology; Immunology.
Citation: Govalan R, Saouaf R, Guindi M, Yang JD, Nissen N, et al. Lymphoepithelioma-like hepatocellular carcinoma, case report of a rare indolent subtype of hepatic cancer. J Clin Images Med Case Rep. 2022; 3(10): 2106.
Background
Lymphoepithelioma is a tumor of epithelial cells with dense infiltration of lymphoid cells. Researchers initially found them in the nasopharynx [1]. In subsequent years, tumors with similar histologic features in the extrapharyngeal sites called Lymphoepithelial-Like Carcinoma (LELC) were identified. In 2010, the World Health Organization recognized a similar rare histologic variant in the liver and termed it lymphoepithelioma-like carcinoma of both HCC and Cholangiocarcinoma (CCA) subgroup [2]. Primary HCC is a rapidly growing tumor with a doubling time of approximately four months, making it one of the leading causes of worldwide cancer-related mortality [3]. Even though some authors have suggested that the prognosis of LELC is better than conventional carcinomas, very few studies have looked at the clinical course in the literature [4]. Moreover, to our best knowledge, there is a lack of data on the natural progression of untreated as well as EBV-associated LELC-HCC, and this topic needs further investigation. We report a highly indolent clinical course of pre-treatment Lymphoepithelioma-Like Hepatocellular Carcinoma (LELC-HCC) associated with EBV that could help bridge this gap.
Case report
A 72-year-old Hispanic female presented with acute on chronic abdominal pain. She suffered from compensated cirrhosis due to treatment-naïve hepatitis C, PBC, non-insulin dependent diabetes and hypertension. She had no family history of cancer. A bout 4 years prior to current presentation, she underwent a CT scan of the abdomen for right upper quadrant pain, which showed a 4.6 x 3.7 x 4.2 cm of the right lobe mass with the arterial enhancement and delayed washout. Unfortunately, she was lost to follow up. She re-presented with the right upper quadrant discomfort with repeat CT scan showing interval increase in the mass to 6.4 x 4.8 cm of the liver mass in the setting of the nodular liver and mild splenomegaly.
The patient had a good performance status. Physical examination was unremarkable with vital signs within the normal range of values. No jaundice or abdominal pain was observed.
Pertinent labs include platelet count 149,000 /μL, albumin 3.9 g/dL, international normalized ratio 1.0, bilirubin 0.5 mg/dL, alkaline phosphatase 173 U/L and Alpha-Fetoprotein (AFP) 11.5 ng/mL. Transaminases, and chemistry panel were normal. Hepatitis C test showed genotype 1a with the viral load of 6.3 log 10 international units per mL. Antimicrobial antibody was positive
Computed Tomography scan (CT) of her abdomen at that time showed nodular liver with a mass measuring 4.6 x 3.7 cm in the right hepatic lobe with heterogeneous enhancement on arterial phase associated with mild venous washout, concerning for HCC (Figure 1 A-B). She was lost to follow up and re-presented 4 years later with an interval increase in the liver mass to 6.4 x 4.8 cm (Figure 1 C-F). Subsequent PET scan confirmed the increased test signal in the mass.
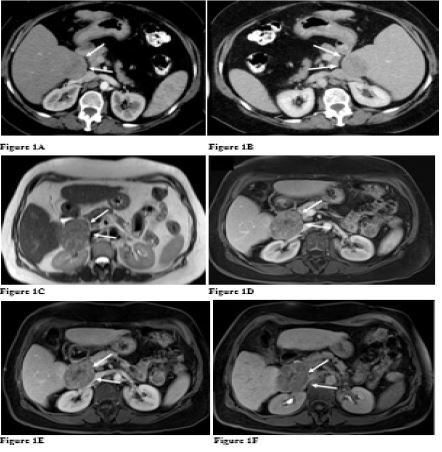
A. Axial CT arterial phase: Partly exophytic mass measuring 4.6 x 3.7 cm with enhancement and central area of hypoenhancement suggesting scar or necrosis.
B. Axial CT venous phase: Mass measuring 4.6 x 3.7 cm with washout of contrast relative to enhancement of liver.
C. MRI Axial T2 Haste: Well defined partly exophytic mass with high T2 signal compared to normal liver with interval increase in size measuring 6.4 x 4.8 cm.
D. MRI VIBE Late arterial phase Eovist contrast: Enhancement of mass with interval increase in size measuring 6.4 x 4.8 cm but with relative hypoenhancement compared to background liver.
E. MRI VIBE Delayed venous phase Eovist contrast: Washout of mass with interval increase in size measuring 6.4 x 4.8 cm in comparison to normal uptake of contrast by liver.
F. MRI VIBE Hepatobiliary phase Eovist contrast: Washout of mass with interval increase in size measuring 6.4 x 4.8 cm in comparison to normal uptake of contrast by liver.
*Mass indicated by white arrow.
The patient underwent segmental surgical resection of the right lobe liver mass, with resection of segments 5 and 6 of the right lobe. This was followed by saline cooled ablation and microwave ablation of the resection bed for margin extension. Staging work up was unremarkable. Gross examination showed a semi-firm, well circumscribed, single subcapsular tan-white mass without necrosis. There were scattered foci of hemorrhage (Figure 2A). Histopathologic examination showed moderately differentiated HCC with massive lymphocytic infiltration within the tumor with lymphocyte outnumbering tumor cells. Lymphoepithelioma-like HCC is composed of atypical large epithelioid cells which represent the malignant hepatocytes arranged in trabeculae. The tumor is massively infiltrated by large numbers of small lymphocytes (appearing as small dark blue dots) (Figure 2B). No lymphovascular invasion was identified, margins were negative. Immunohistochemical staining showed tumor cell immunoreactivity for the hepatocellular lineage markers, Hepar-1 and Arginase 1, confirming HCC with negative CK-19 (Figure 2C). In situ hybridization for Epstein Barr Virus (EBV) showed reactivity in a few of the inflammatory mononuclear cells in the background within the tumor (Figure 2D).
Based on the patient’s history, clinical presentation, imaging and pathology we diagnosed her with LELC-HCC. The patient had excellent prognosis with no tumor recurrence on surveillance at 16 months after her surgery. She was subsequently treated for Hepatitis C with successful viral clearance.
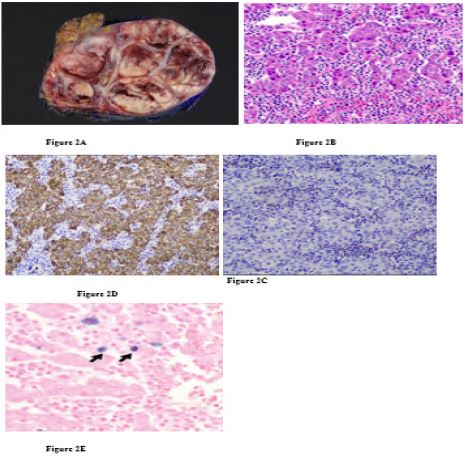
A.Macroscopic examination of this lymphoepithelioma-like HCC shows a tan well-circumscribed nodule, the appearance is not subtype specific.
B.Hepatocellular carcinoma (large pink atypical cells) with an abundance of intratumoral lymphocytes(Hematoxylin and eosin, magnification 200x)
C. Hepar-1 immunostain (brown) is positive in tumor cells confirming hepatocellular carcinoma and is negative in lymphocytes (Hepar 1 immunostain, magnification 200x)
D. Hepatocellular carcinoma cells negative for the Keratin 19 (an epithelial marker that is positive in cholangiocarcinoma) (keratin immunostain 200 magnification)
E. In situ hybridization for EBV show few positive nuclei of tumoral lymphocytes (arrows, magnification 400x)*EBV positive nuclei indicated by Black arrow.
Discussion
Primary LELC in the liver is a rare histologic variant of Hepatocellular Carcinoma (HCC). They are epithelial cell tumors of variable grades of differentiation with dense lymphoid stroma found in the liver [1,4]. The paucity of data on the natural progression of untreated LELC-HCC is partly due to similarities in the imaging pattern of typical HCC and LELC-HCC, leading to misdiagnosis and early initiation of treatment to prevent tumor progression [5]. There have been no reports to our knowledge of the prognosis of the untreated natural course of LELC-HCC. Our patient was lost to follow up for four years after the initial presentation with liver mass which allowed us to report a natural history of untreated LELC-HCC. As opposed to the rapid progression of typical HCC, our patient’s mass has only minimally grown over four years, demonstrating the highly indolent progression and unique characteristics of LELC-HCC.
The overall good prognosis of LELC-HCC might be due to the antitumor effect of the lymphocyte infiltrating the tumor. Most reported subjects had a CD4+ and CD8+-T cell predominance over B cells, which might have contributed to the cytotoxic antitumor effect in LEL- HCC [6]. In addition, Chan et al. performed whole-exome sequencing comparing LELC-HCC and typical HCC, which showed distinct molecular mutations of LELC-HCC (e.g., amplification of chromosome 11q13.3) strongly associated with the immune checkpoint signature [7]. Similar to LELC-HCC, studies that compared the outcome of patients with pulmonary LELC and gastric LELC also found them to be more favorable than that of non- LELC cases [8,9]. This prognostic advantage of Tumor-Infiltrating Lymphocytes (TIL) is also evident in other solid cancer types, including melanoma, Colorectal Cancer (CRC), breast and ovarian cancers. Pages et al. suggested that CRC infiltrated with memory and effector T cells were less likely to disseminate to lymphovascular and regional lymph nodes [10].
EBV is a herpes virus that plays a prominent role in the oncogenesis of epithelial and lymphoid tumors [9]. There have been reports of variable association of Epstein Barr Virus (EBV) with LELC depending on their site of origin. It is commonly associated with LELC of the nasopharynx, gastric, and lung carcinomas, while infrequently found in the bladder, breast, and uterine LELC subtypes [11]. Most of the reported EBV association with LELC in the hepatobiliary system are the cholangiocarcinoma subtypes, with only about 3 other cases of EBV association in the HCC subtype [12]. The HCC subtype in contrast is typically associated with HCV and HBV infections and they are thought to contribute to their immunogenicity [4]. Our patient was positive for HCV infection but the few EBV-positive mononuclear cell infiltration in our patient’s tumor is of unclear significance. It is not known if EBV directly contributes to the development of LELC or if it offers a protective effect by enhancing the immune response. Min et al. and a few other studies compared the clinicopathologic and prognosis of EBV positive and negative lymphoepithelioma-like gastric carcinoma patients. They proposed that EBV positivity is an independent predictor of favorable prognosis [13,9,14]. They attributed the survival advantage to the patients’ inflammatory response directed against the EBV proteins in the cancer cells. They found increased tumor-infiltrating lymphocytes, particularly cytotoxic CD8 positive cells, and lower mitotic rates in the EBV positive LELC cases than their counterparts [13]. In contrast, Si et al. presented an EBV positive LELC-HCC case with recurrent HCC 5 months post-liver transplantation with a poor prognosis. The recurrent tumor was devoid of lymphocyte infiltrate when the patient had immunosuppressive therapies in the post-transplant period [12]. This case further supports that the survival advantage in EBV positive LELC might be from an inflammatory response, and with immunosuppression, it likely loses its prognostic advantage. The survival benefit may be due to the EBV infection in our patient. However, given the rarity of EBV association with LELC-HCC, their role remains inconclusive and needs further investigation. Finally, denovo HCC recurrence contributes to a majority of late recurrence after curative cancer treatment. Intratumoral lymphocyte infiltration is shown to be a positive prognostic factor in many solid organ cancers including HCC. How this will affect denovo HCC development in the background liver remains unknown and should be further investigated in future studies.
Conclusion
To conclude, to the best of our knowledge, this is the first case to report the indolent natural progression of untreated LELC-HCC over four years and the fourth case to report EBV-associated LELC-HCC. The prognostic benefit might have been mediated by the anti-tumoral effect of immune cell infiltration into the tumor, further accentuated by the presence of EBV or HCV infection [15].
Declarations
Financial support statement: Dr. Yang’s research is supported by American College of Gastroenterology Junior Faculty Development Award, Department of Defense Peer Reviewed Cancer Research Program Career Development Award, National institute of Health (1K08CA259534-01A1) Cedars-Sinai Clinical Scholar award, and Huiying Foundation. The American College of Gastroenterology, Department of Defense, National institute of Health, Cedars-Sinai Medical Center, and Huiying Foundation had no role in the collection of data; analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Rest of the authors have no financial declarations.
Conflict of interest statement: Dr. Yang provides a consulting service for Exact Sciences, Gilead Sciences, and Eisai.
Rest of the Authors have no conflict of interest.
Patient consent declaration: Informed consent was obtained from the patient for publication of this report and any accompanying images by Dr. Ju Dong Yang
References
- Applebaum EL, Mantravadi P, Haas R. Lymphoepithelioma of the nasopharynx. Laryngoscope. 1982; 92: 510-514.
- FT Bosman FC, RH Hruban WHO classification of tumours of the digestive system. Third edition ed. Lyon, France: IARC Press; 2010.
- Nathani P, Gopal P, Rich N, Yopp A, Yokoo T, John B, et al. Hepatocellular carcinoma tumour volume doubling time: A systematic review and meta-analysis. Gut. 2021; 70: 401-407.
- Solinas A, Calvisi DF. Lessons from rare tumors: Hepatic lymphoepithelioma-like carcinomas. World J Gastroenterol. 2015; 21: 3472-3479.
- Chen CJ, Jeng LB, Huang SF. Lymphoepithelioma-like hepatocellular carcinoma. Chang Gung Med J. 2007; 30: 172-177.
- Chan AW, Tong JH, Pan Y, Chan SL, Wong GL, Wong VW, et al. Lymphoepithelioma-like hepatocellular carcinoma: an uncommon variant of hepatocellular carcinoma with favorable outcome. Am J Surg Pathol. 2015; 39: 304-312.
- Chan AW, Zhang Z, Chong CC, Tin EK, Chow C, Wong N. Genomic landscape of lymphoepithelioma-like hepatocellular carcinoma. J Pathol. 2019; 249: 166-172.
- Han AJ, Xiong M, Gu YY, Lin SX, Xiong M, et al. Lymphoepithelioma-like carcinoma of the lung with a better prognosis. A clinicopathologic study of 32 cases. Am J Clin Pathol. 2001; 115: 841-850.
- Song HJ, Srivastava A, Lee J, Kim YS, Kim KM, et al. Host inflammatory response predicts survival of patients with Epstein-Barr virus-associated gastric carcinoma. Gastroenterology. 2010; 139: 84-92.e2.
- Pagès F, Berger A, Camus M, Sanchez-Cabo F, Costes A, Molidor R, et al. Effector memory T cells, early metastasis, and survival in colorectal cancer. N Engl J Med. 2005; 353: 2654-2666.
- Adachi S, Morimoto O, Kobayashi T. Lymphoepithelioma-like cholangiocarcinoma not associated with EBV. Pathol Int. 2008; 58: 69-74.
- Si MW, Thorson JA, Lauwers GY, Dal Cin P, Furman J, et al. Hepatocellular lymphoepithelioma-like carcinoma associated with epstein barr virus: A hitherto unrecognized entity. Diagn Mol Pathol. 2004; 13: 183-189.
- Nakamura S, Ueki T, Yao T, Ueyama T, Tsuneyoshi M, et al. Epstein-Barr virus in gastric carcinoma with lymphoid stroma. Special reference to its detection by the polymerase chain reaction and in situ hybridization in 99 tumors, including a morphologic analysis. Cancer. 1994; 73: 2239-2249.
- Min BH, Tae CH, Ahn SM, Kang SY, Woo SY, Kim S, et al. Epstein-Barr virus infection serves as an independent predictor of survival in patients with lymphoepithelioma-like gastric carcinoma. Gastric Cancer. 2016; 19: 852-859.
- Wang S, Sun J, Chen K, Ma P, Lei Q, Xing S, et al. Perspectives of tumor-infiltrating lymphocyte treatment in solid tumors. BMC Med. 2021; 19: 140.